Chronic rotator cuff tears, which affect the patients’ quality of life, lead to global burden with severe health-care and socioeconomic consequences. Many studies have demonstrated that several anatomical factors of acromion and greater tuberosity are associated with chronic rotator cuff tears. Kanatli U et al.[16] and Balke M et al.[17] have indicated that on shoulder X rays, the lateral acromion angle (LAA), which reflects the glenoid inclinations of patients with full-thickness rotator cuff tears, is significantly higher than that in controls without rotator cuff tears. Moor BK et al.[19] and Nyffeler RW et al. [21] have demonstrated that the acromion index (AI), which quantifies the acromial coverage exhibits the same results mentioned above. In contrast, some other researchers have found that the inclination and extension of the acromion are not correlated with the morbidity of partial rotator cuff tears, and no significant differences among different types of chronic rotator cuff tears[20]. Most footprints of the rotator cuff tendons are distributed around the greater tuberosity, which is close to the position of the acromion, so the characteristics of greater tuberosity may distribute to chronic rotator cuff tears. Previous studies have reported that the reduction in bone density of the greater tuberosity leads to decrease in strength of the rotator cuff attachment, which causes chronic rotator cuff tears[23]. Cystic changes in the front of greater tuberosity are also closely related to rotator cuff tears[27]. However, the relationship between the morphological features of greater tuberosity and chronic rotator cuff tears is unclear. Similar to previous research on the morphological characteristics of acromion, we selected the parameters that reflect greater tuberosity morphology including abduction angle, width and height, to determine their relations with different types of chronic rotator cuff tears.
Although most previous studies have measured the morphological parameters of acromion from shoulder X rays, initially the LAA and AI were measured on the oblique coronal plane of MRI[28, 29]. In this study, we also measured the morphological parameters of greater tuberosity on the oblique coronal plane of shoulder MRI, which enabled standardized and accurate evaluation among different research objects under the same position and in different scanning planes.
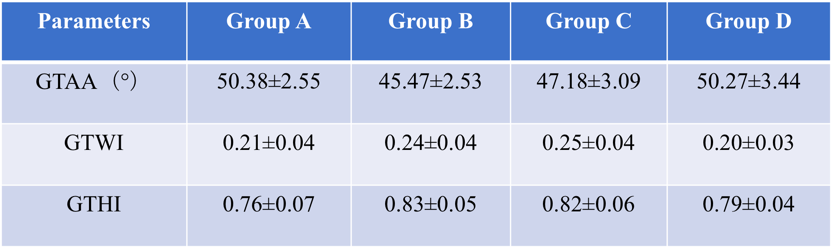
The GTAA measured in this research is a dynamic parameter that could reflect the abduction degree of greater tuberosity when the articular side of supraspinatus tendon is pinched against the posterior-superior glenoid rim. According to the GTAA analysis, we found that the GTAA of patients with articular-side and full-thickness rotator cuff tears was significantly less than that of the controls, whereas the GTAA of patients with bursal-side rotator cuff tears was not obviously different from that of the controls. This finding suggested that the reduction of the GTAA was a risk factor for articular-side and full-thickness rotator cuff tears and had no significant correlation with bursal-side rotator cuff tears. Supposedly, when the shoulder joint abducts, the greater tuberosity with low GTAA will collide with the posterior-superior glenoid rim more frequently, which gradually leads to articular-side rotator cuff tear. Moreover, the GTAA exhibited no significant difference between the articular-side tear group and the full-thickness tear group, which suggests that the full-thickness rotator cuff tears may originate from articular-side tears.
To study the morphological features of greater tuberosity, except its dynamic parameter GTAA, it is necessary to determine whether the static parameters of greater tuberosity are associated with different types of chronic rotator cuff tears. In this study, the GTWI and GTHI respectively reflected the extents of the greater tuberosity being convex outward and upward in the proximal humerus. The results demonstrated that the greater tuberosity of the patients with chronic articular-side and full-thickness rotator cuff tears was more convex outward and upward than that of the patients with bursal-side tears and the controls. The results suggest that increased width and height indices were risk factors for chronic articular-side and full-thickness rotator cuff tears. Moreover, the results from the articular-side tear group exhibited no significant differences from those of the full-thickness tear group, which suggests again that the full-thickness rotator cuff tears may originate from articular-side tears. Based on anatomy, if the greater tuberosity gets widened and heightened due to hyperostosis and osteophyte, when the shoulder abducts, collision and friction between the articular-side of supraspinatus tendon and the posterior-superior glenoid rim are increased, gradually result to chronic rotator cuff tears. Simultaneously, the morphological changes of greater tuberosity may be a secondary response to chronic rotator cuff tears. Davidson et al.[30] reported a case of a 23-year-old right-handed professional baseball pitcher with an articular-side rotator cuff tear. An exploration of the pathogenesis revealed that frequent abduction and external rotation led to an articular-side tear of the supraspinatus tendon that pinched against the posterior-superior glenoid rim, which supports our research results and mechanisms.
Our study find that the greater tuberosity abduction angles are smaller, but greater tuberosity are more convex outward and upward in patients with articular-side or full-thickness rotator cuff tears, than in patients with bursal-side rotator cuff tears or in controls. Chronic articular-side and full-thickness rotator cuff tears are related to the morphology of greater tuberosity, which can assist us to estimate the type of chronic rotator cuff tears when we have difficulty in differential diagnosis via shoulder MRI, and to find the supraspinatus tendon’s tear position under arthroscopic surgery more quickly.
Certainly, our study has several limitations. Firstly, the number of enrolled patients was small, and the specific duration of disease was not considered. Secondly, chronic rotator cuff tears result from multiple factors. Except for the parameters mentioned in our study, whether other morphological features of the shoulder joint distribute to different types of chronic rotator cuff tears needs to be explored in the future.
{kind=link}
{kind=link}