In total, 116 physicians completed the survey (Table 1). All respondents answered all required questions. Most participants (57%) were 41-60 years old. The majority (95%) were gynecologists and worked at academic (66%) or university (25%) hospitals. Most respondents (78%) worked in a higher position, such as senior physician or head of department, and in a certified breast cancer center (93%). Forty-three percent of participating physicians stated that one or more colleagues at their department were breast ultrasound specialists of at least DEGUM II level (DEGUM = German Society for Ultrasound in Medicine).
Table 1. Sociodemographic data of respondents.
|
Question
|
n (%)
|
|
Sex
Female
Male
Diverse
|
73 (63%)
42 (36%)
1 (1%)
|
|
Age
< 30 years old
30-40 years old
41-50 years old
51-60 years old
> 60 years old
|
2 (2%)
29 (25%)
33 (28%)
34 (29%)
18 (16%)
|
|
Specialty
Gynecology
Radiology
|
109 (95%)
6 (5%)
|
|
Department type
University hospital
Academic hospital
Hospital without academic affiliation
Practice / outpatient clinic
Mammography screening
|
29 (25%)
76 (66%)
10 (9%)
9 (8%)
2 (2%)
|
|
Current position
Resident
Specialist
Senior Physician
Head of Department
|
9 (8%)
16 (14%)
57 (49%)
34 (29%)
|
|
Is your department part of a certified breast cancer center?
Yes
No
|
108 (93%)
8 (7%)
|
|
Number of breast cancer cases treated at the department per year
< 100
100-200
201-300
301-400
> 400
|
5 (4%)
52 (45%)
26 (22%)
16 (14%)
16 (14%)
|
|
Highest DEGUM1) breast ultrasound qualification available at the department
None
DEGUM I
DEGUM II
DEGUM III
|
36 (31%)
30 (26%)
42 (37%)
7 (6%)
|
1) German Society of Ultrasound in Medicine (www.degum.de)
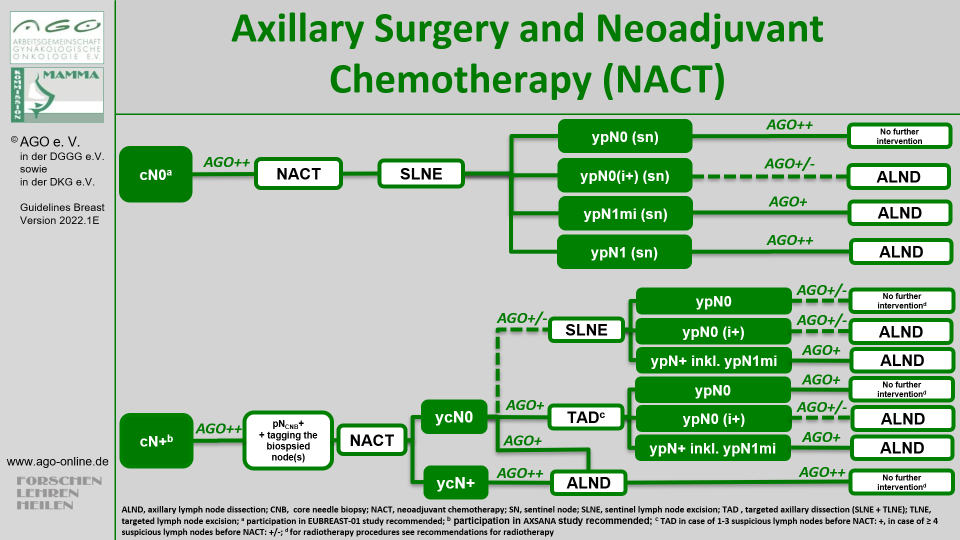
Axillary management in cN0 patients
In patients with clinically negative node status scheduled to receive NACT, 89% of respondents recommended SLNB after NACT (Supplementary Table 2). Four respondents stated that they perform SLNB both before and after NACT, depending on the individual case. They were asked to describe which factors this decision might depend on, and named the following:
- small HER2-positive tumors when pre-NACT SLNB may impact therapy choice
- dependent on ultrasound findings
- in case of a planned mastectomy to assess the indication for radiation therapy (in this case, SLNB may impact choice of reconstructive technique)
- age, prognosis
In case of a micrometastasis in a sentinel node after NACT, most respondents (44%) recommended no further axillary therapy, while 31% proposed completion ALND and 25% irradiation of the axilla.
Axillary management in cN+ patients
In case of suspicious axillary nodes at the time of diagnosis, 64% of respondents recommended a minimally invasive biopsy to all patients, confirming the nodal status, while 34% advised it to selected patients only, and did not offer minimally invasive biopsy in case of unequivocally positive node status upon imaging (n = 19), in cases with high tumor load in the axilla including level I to III (n = 27), in cases with at least 2 (n = 4) or at least 4 (n = 13) suspicious nodes (Table 2). Other reasons for the omission of a confirmative biopsy were nodes located in a direct proximity of blood vessels, leading to an increased complication risk (n = 3) and high patient age (n = 2). The vast majority performed core needle biopsy instead of fine needle aspiration.
TAD was recommended to most patients converting from a clinically positive a to clinically negative node status through NACT (cN+ → ycN0) by 91% of respondents, followed by ALND (16%) and SLNB (5%). None of the respondents chose targeted lymph node biopsy as the technique of choice in this setting.
Table 2. Current approach to axillary treatment in cN+ patients in the neoadjuvant setting.
|
Question
|
n (%)
|
|
Do you recommend cN+ patients a minimally invasive confirmation of lymph node status?
No
Yes, always
Yes, but not in all patients
|
2 (2%)
74 (64%)
40 (34%)
|
|
Which technique of minimally invasive biopsy do you usually perform?
Core biopsy
Fine needle aspiration
I do not perform minimally invasive biopsies
|
106 (91%)
5 (4%)
5 (4%)
|
|
Which axillary staging technique do you recommend for most of your cN+ patients converting to ycN0 status?
Axillary lymph node dissection
Targeted axillary dissection (TAD)
Sentinel lymph node biopsy
Targeted lymph node biopsy
|
19 (16%)
91 (78%)
6 (5%)
0 (0%)
|
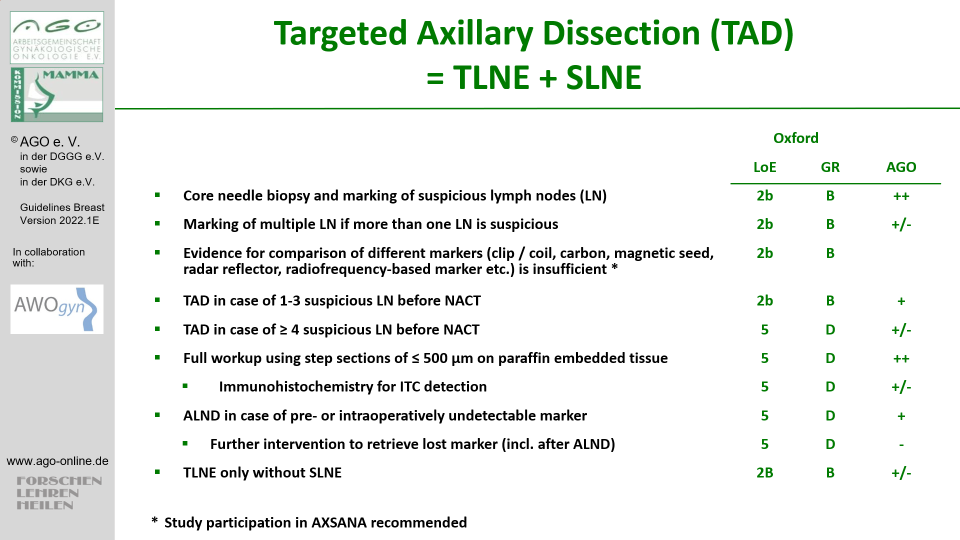
Nearly all respondents were familiar with TAD, and 82% stated that the technique was offered at their department (Table 3). In 47% of cases, considerable experience with TAD has been gathered so far (at least 30 procedures performed), and 70% of respondents reported that their department takes part in or plans to join the international AXSANA study (http://axsana.eubreast.com). While the majority of respondents recommended TAD to all cN+ patients converting to ycN0, 43% offered the technique to selected patients only. This group was asked which factors influenced their decision whether to offer TAD or not. The free-text answers were (multiple answers were allowed):
- number of suspicious nodes (85%); 18 respondents reported that they offer TAD to patients with:
- 1 suspicious node: 2 (11%)
- 2 suspicious nodes: 9 (50%)
- 3 suspicious nodes: 5 (28%)
- 4 suspicious nodes: 2 (11%)
- inflammatory breast cancer (5%)
- good response to NACT in the breast (2%)
- tumor biology (2%)
- age (2%)
- depending on the surgeon (7%)
Table 3. Current approach to targeted axillary dissection.
|
Question
|
n (%)
|
|
How much experience does your department have with targeted axillary dissection?
I have never heard of this technique
I have heard of this technique, but it is not used in my department
TAD is used in my department
|
1 (1%)
20 (17%)
94 (82%)
|
|
How many TAD procedures have been performed in your department so far?
< 30
≥ 30
|
50 (53%)
44 (47%)
|
|
Do you offer TAD to all or only selected cN+ → ycN0 patients?
All
Selected
|
54 (57%)
41 (43%)
|
|
Do you perform frozen section of target and sentinel lymph node(s)?
Yes
No
|
44 (45%)
54 (55%)
|
|
Does your department participate in the AXSANA EUBREAST-3 study?
Yes, already registered
Yes, study participation planned
No
|
64 (56%)
16 (14%)
35 (30%)
|
Abbreviations: TAD – targeted axillary dissection
Marking techniques
While the marking of axillary lymph node(s) in cN+ patients before NACT was supported by the majority of respondents (Table 4), it was used in selected patients only by 37%. The main factor influencing this decision was the number of initially suspicious lymph nodes. The marking procedure was undertaken during minimally invasive biopsy, i.e., as one procedure, by 53%, while 25% delayed the procedure until the histological/pathological report was available. The remaining 22% of respondents reported that the time point of lymph node marking may depend on:
- The probability of node metastasis
- The indication for NACT
- The indication for TAD
- Patient preference
In patients presenting with more than one suspicious node at time of diagnosis, 42% of respondents recommended marking of only one node, while 33% stated that they mark two nodes in such cases. A fifth (22%) answered that the number of marked nodes may vary and that factors influencing the number of marked nodes were e.g., the radiologist’s assessment or the number of biopsied nodes.
The most common marking technique was a clip/coil, used by 85% of respondents. Probe-guided detection techniques such as magnetic, radar reflecting, or radiofrequency markers were used less commonly (Table 4). Among clips/coils, different shapes and types are used:
- Tumark Vision: 38% (n = 23)
- HydroMark: 29% (n = 17)
- O-TWIST: 27% (n = 15)
- Müller-Schimpfle-Coil: 4% (n = 2)
- KliniMark: 2% (n = 1)
- Tumark Professional: 2% (n = 1)
Among respondents using clips/coils for lymph node marking, 86% performed preoperative wire localization and 42% intraoperative ultrasound to identify target lymph nodes. In case a clip/coil cannot be visualized on ultrasound, 54% recommended additional imaging, usually mammography or computed tomography, while the remaining 46% did not.
Table 4. Current approach to lymph node marking.
|
Question
|
n (%)
|
|
Do you recommend lymph node marking to your cN+ patients before NACT?
No
Yes, to all patients
Yes, to selected patients
|
11 (10%)
61 (53%)
43 (37%)
|
|
Which marking technique do you currently use?
Ink
Magnetic seeds (e.g., MagSeed)
Radioactive seeds
RFID Tags (Radiofrequency marker, e.g., LOCalizer)
Radar-based markers (e.g., SaviScout)
Clips/Coils
|
4 (4%)
5 (5%)
4 (4%)
1 (1%)
1 (1%)
87 (85%)
|
|
When do you mark lymph nodes?
At time of minimally invasive biopsy
After the histological/cytological report
Both at time of minimally invasive biopsy and after the histological/cytological report
|
54 (53%)
26 (25%)
22 (22%)
|
|
How many lymph nodes do you mark, if more then one node is suspicious?
One node
Two nodes
Three or more nodes
Depends on other factors
|
43 (42%)
34 (33%)
3 (3%)
22 (22%)
|
Abbreviations: NACT – neoadjuvant chemotherapy
Detection rates of different markers
While 67% of respondents estimated the detection rate of their marker to be very good or good, 30% reported it was satisfactory and 2% that it was unsatisfactory (Supplementary Table 3). This was independent of the highest breast ultrasound qualification at the respondent’s department (Figure 1). In case of ink, magnetic seeds, radar reflecting markers and RFID tags, all survey participants described the detection rate as good or very good. In contrast, only 65% of respondents using clips/coils reported a good or very good detection rate. Detection rates of different clip/coil types are presented in Supplementary Table 4. Due to small absolute numbers, a reliable comparison of detection rates using different markers was not possible.
“Lost marker”
Thirty-nine out of 102 (38%) respondents reported that it had occurred at their department at least once that the retrieval of a marker placed before NACT could not be confirmed at surgery. Among these, 15 participants stated that no postoperative imaging was performed so that it remained unclear whether the marker was still residing in the patient or not. The remaining 24 respondents reported that in some cases, postoperative imaging confirmed marker removal at surgery, while in others the marker was still in situ. Different imaging modalities such as mammography / X-ray, (low dose) CT and ultrasound were used to search for the lost marker. When asked about the clinical consequences of a residual marker, 13 survey respondents answered that a second surgery was discussed individually with the patient.
MRI artifacts
Respondents using magnetic, radar reflecting, or radiofrequency markers were asked two additional questions about MRI after marker placement. One respondent using RFID tags and two using magnetic markers reported MRI artifacts, others did not perform MRI after marker placement. All three reported that the evaluation of MRI was “somewhat limited” due to artifacts.
Which factors influence attitudes of surgeons and radiologists towards axillary management?
High-volume departments were significantly more likely to employ at least one physician with an ultrasound qualification of DEGUM II or III (p < 0.001). DEGUM II/III ultrasound specialists were part of the team in 72% of departments treating over 300 cases per year. In contrast, only 34% of centers with ≤ 200 breast cancer cases per year had DEGUM II/III qualified staff. There was no correlation between highest DEGUM qualification in the department and attitudes of respondents towards axillary management in cN0 and cN+ patients. However, departments with DEGUM II/III qualification were significantly more likely to have experience with TAD compared to those with highest qualification DEGUM I or none (92% vs. 74% respectively, p = 0.018). In departments performing TAD, the number of procedures conducted so far did not correlate with the highest DEGUM qualification.
Interestingly, while 51% of respondents working in DEGUM II/III departments reported to offer TAD to selected but not all cN+ → ycN0 patients, 65% of participants from departments without DEGUM II/III qualification offered TAD to all patients (Fig. 2). This difference was not significant (p = 0.108). Respondents from larger departments were significantly more likely to offer TAD to selected patients only than those from smaller centers (39.3% in departments treating over 300 vs. 64.2% in ≤ 300 breast cancer cases per year, p = 0.026).
Respondents’ age, position and sex did not influence their attitudes towards axillary management. Answers did not correlate with the department type (university / academic vs. other).
{kind=link}
{kind=link}