3.1. Study inclusion
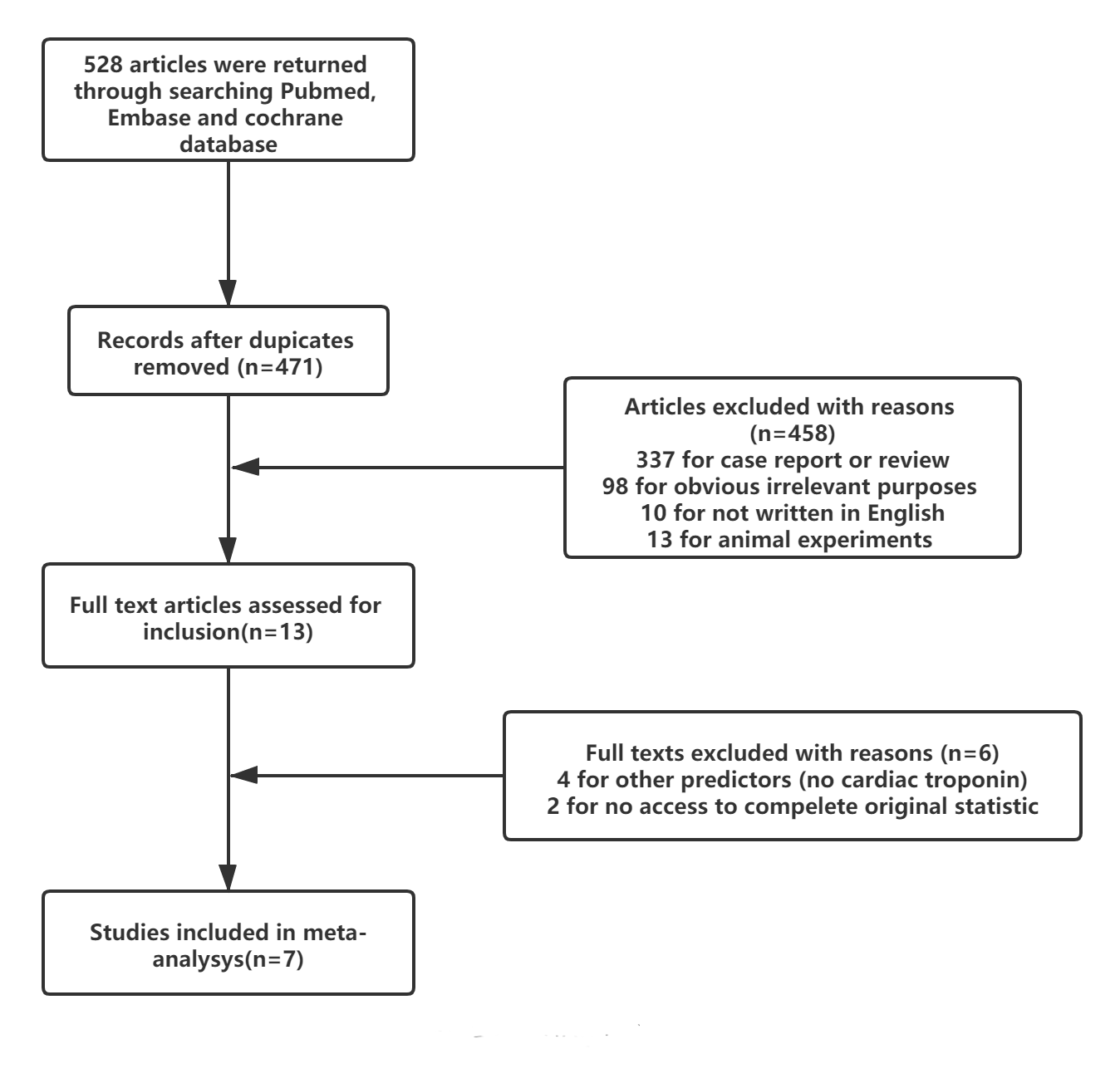
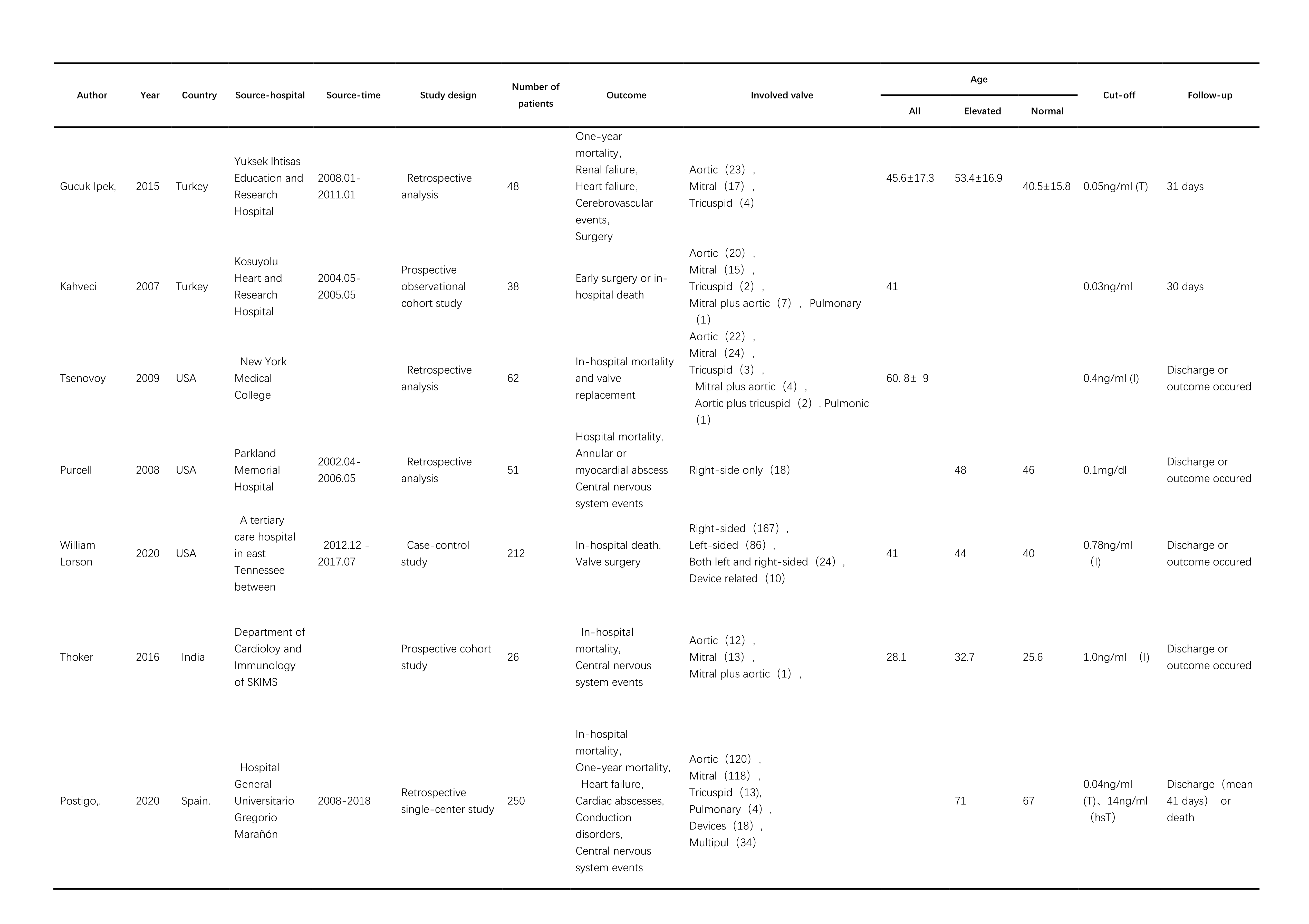
The initial literature search on databases identified 528 articles. After excluding the duplicates, 471 were selected for the further selection process. Of these, 458 were excluded after screening through the titles and abstracts, where the main reasons for exclusion were case or conference report, irrelevant to the objectives of our study, review articles, and animal experiments. A total of 13 studies were selected for full-text screening, following which 4[15, 25–27] were excluded because of discrepancy in cardiac markers being used (not cardiac troponin) or target population being examined were of other cardiac diseases, 2[28, 29] were eliminated because the original data were not accessible. Ultimately, a total of 7[30–36] studies were included for our meta-analysis (the PRISMA flow diagram was shown in Figure S1(Supplementary file 1)
3.3 Clinical Outcomes and meta-analysis
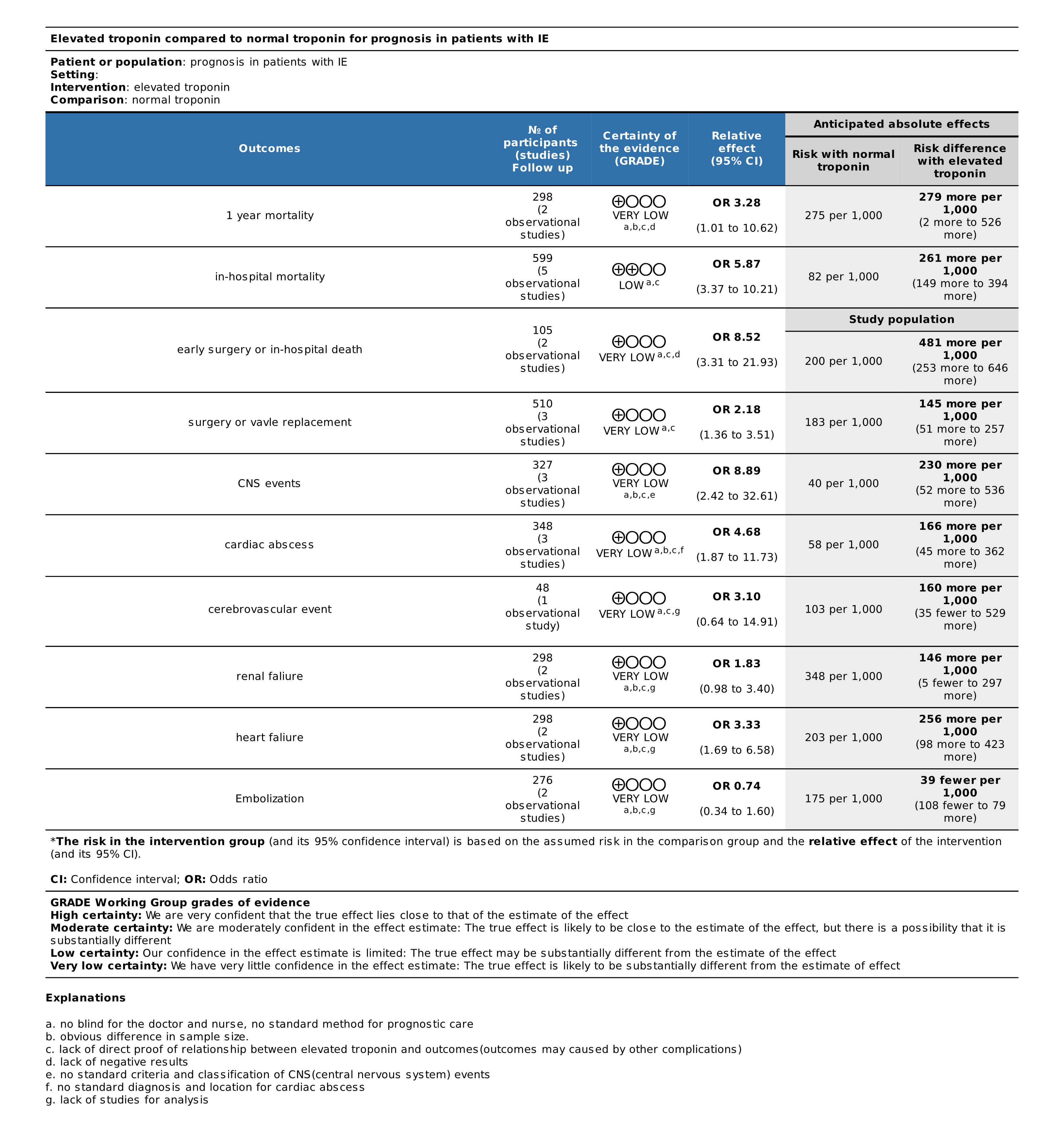
The anticipated absolute effects of each study for different outcomes were outlined in Table 2. Of all the clinical outcomes (n = 10) analyzed in our study, in-hospital mortality[37] was rated as ‘critical in importance’, embolization was rated as ‘not important’[38], while other outcomes were assessed as ‘important’. As the most important endpoint, in-hospital mortality achieved a risk difference of 279 /1000 (95%CI 2-526) with elevated cardiac troponin.
In-hospital mortality was reported in 5[30–34] studies with no obvious heterogeneity detected (Chi² = 2.65, P = 0.62; I² = 0%) and thus, fixed-effects model was used. Patients with elevated cardiac troponin had a significantly higher in-hospital mortality than those with a normal level [OR = 5.87, 95% CI (3.37,10.21)]. Furthermore, 2 [33, 36]studies reported one-year mortality that comprised of a total of 298 patients, which demonstrated an elevated cardiac troponin as a significant risk factor among those diagnosed with IE [OR = 3.28, 95% CI (1.01,10.62)]. There were 2[30, 35] studies assessing early surgery and in-hospital mortality together in 105 patients, showing that patients with elevated cardiac troponin were associated with higher mortality or incidence of early surgery during hospitalization [OR = 8.52, 95% CI (3.31,21.93)]. Of those excluded studies, 2[28, 29] that did not have accessible original data also reported a higher mortality rate among patients with a higher cardiac troponin level than those with a normal level, with an OR of 7.0 [95% CI (1.7,28.6)] and 3.4 [95% CI (1.8,6.4)] respectively.
Incidence of surgery (valve replacement) was assessed by 3[33, 34, 36] studies comprised of a total of 510 patients. A higher proportion of patients (144/286, 50.35%) in the group of elevated cardiac troponin levels had undergone surgery, compared with 18.30% (41/224) of patients in the group of normal cardiac troponin level [OR = 2.18, 95% CI (1.36,3.51)].
Symptoms of the central nervous system were assessed in 3[31–33] studies. A significantly higher proportion of patients with an elevated cardiac troponin level (21.43,54/252) had symptoms of the central nervous system than those with a normal level (4.00%,3/75) [OR = 3.28, 95% CI (1.01,10.62)].
Besides, cardiac abscesses were examined as an outcome in 3[32, 33, 36] studies, comprised of a total of 262 patients with an elevated cardiac troponin level and 86 with a normal level. The incidence of cardiac abscesses of the two groups was 27.10% (71/262) and 5.81% (5/86) respectively, demonstrating a markedly increase in risk among those with a higher cardiac troponin level [OR = 3.28, 95% CI (1.01,10.62)].
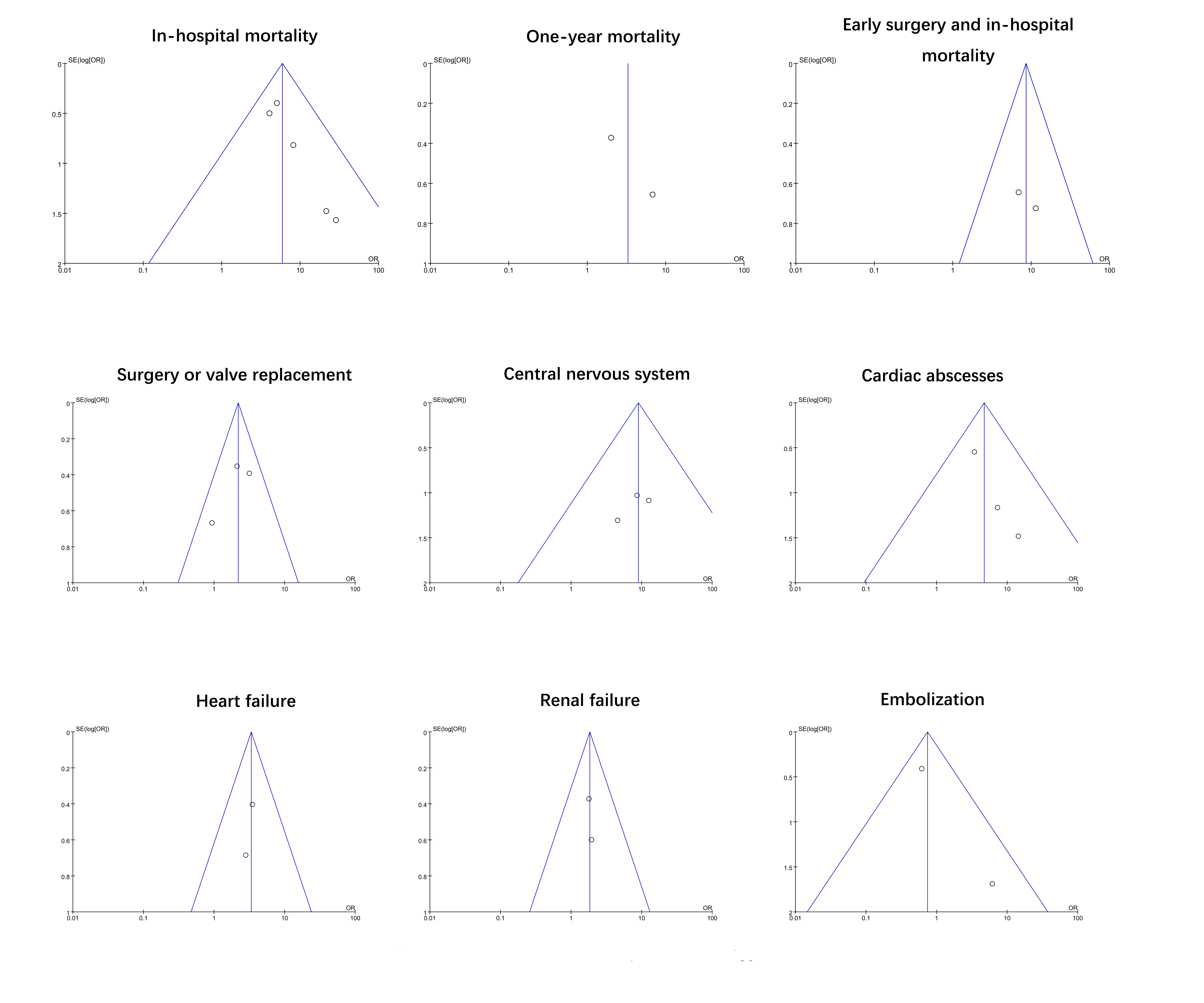
Furthermore, the incidence of cerebrovascular events was examined as an endpoint in 1[36] study only, with no association found with the levels of cardiac troponin [OR = 3.10, 95% CI (0.64,14.91)]. Similarly, no significant association was found between renal failure and embolization (assessed by 2 different studies) with the levels of cardiac troponin. On the other hand, patients with elevated cardiac troponin had a higher risk of heart failure (reported in 2 studies). The detailed analyses of all the clinical outcomes in association with cardiac troponin levels were shown in Fig. 1
Except for cerebrovascular events, all the other outcomes in the included studies were homogenous and thus, the fixed-effects model was applied in the meta-analyses for these outcomes. Apart from the outcome of one-year mortality, all the other clinical outcomes were recorded before hospital discharge.
3.4 Bias assessment
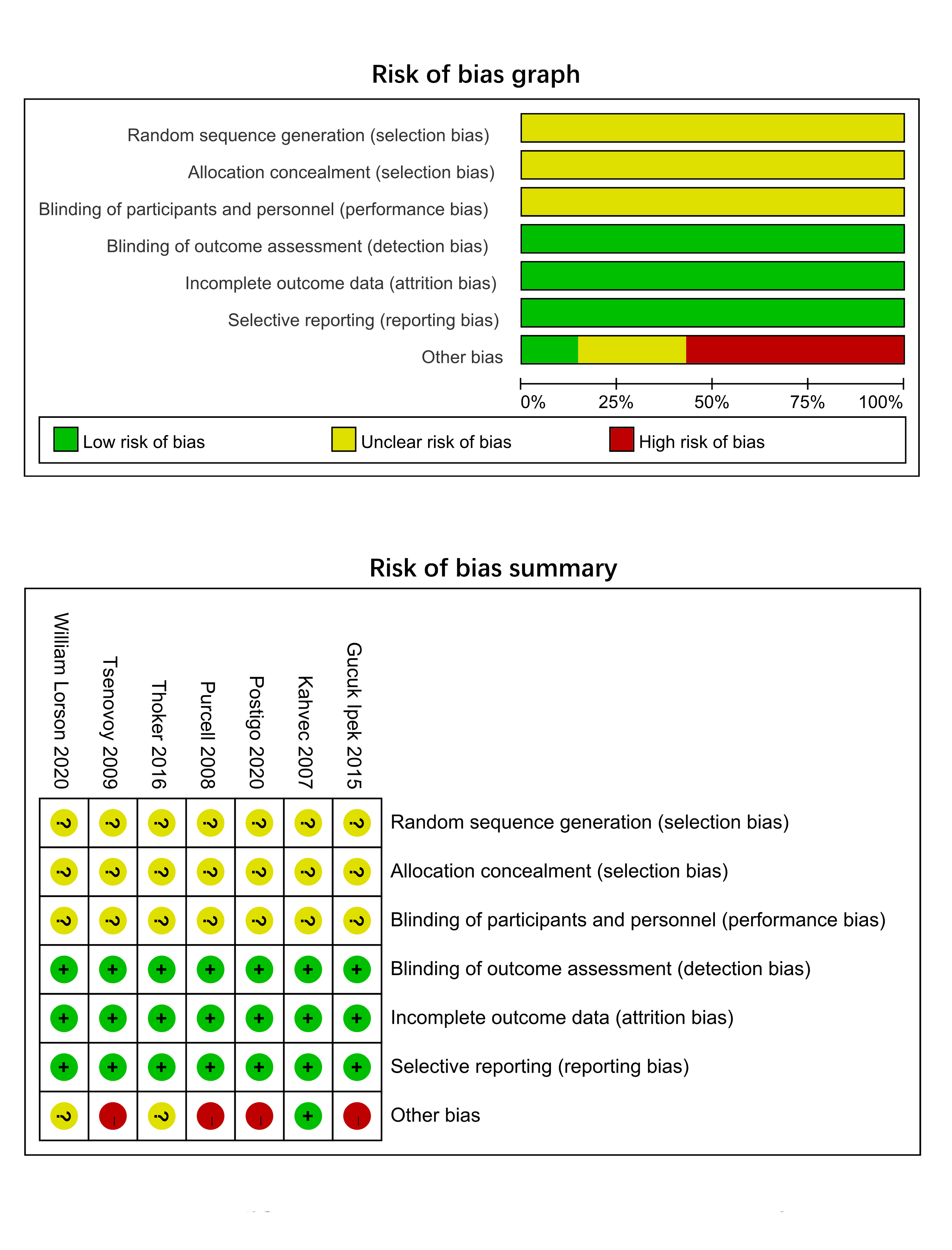
Included studies were subjected to bias assessment based on the Cochrane risk Assessment tool. All the studies were regarded as having a low risk for detection bias, attrition bias, and reporting bias. However, given that those included studies were not an RCT, the risk of selection bias and performance bias was unclear. The risks of other potential biases were outlined in Figure S2. The GRADE evidence profile demonstrated the quality and risk of bias individually for various outcomes. In 6 studies, the certainty of the evidence was rated as ‘very low’, while one study was rated as ‘low certainty’ (Table 2).
For in-hospital mortality, funnel plots revealed uniformity and symmetrical distribution, indicating no significant publication bias among these studies (Figure S3). However, publication bias of other outcomes could not be assessed due to lacking in numbers of included studies.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}