Search results and Characteristics of the studies
As shown in figure 1 and table 1, totally 734 records were screened by title and abstract. Of which 35 publications were selected for full-text review and appraised for eligibility. As well cited references in these articles were inspected to identify additional reports. At last, 19 studies with 728 participants met the selection criteria for this review [3, 5, 10-13, 17, 20, 24, 28-37]. These studies comprised 16 full publications and 3 meeting abstracts. Among which, 10 were conducted in China, 5 in Europe, 1 in the USA, 2 in Iran, and 1 in Korea. Six of the 19 studies were RCTs with 234 participants, and the remaining 13 trials were sorted as nRCTs, including 7 prospective controlled studies with a total of 203 patients, and 6 historical controlled studies contained 291 participants. Ten trials were in adolescents or children, seven were in adults, one trial involved patients aging from 3 to 48 years old and 1 trial did not mention the average age of participants. Two trials were in patients with β-thalassaemia, one in severe aplastic anemia (SAA), thirteen trials were in patients with hematological malignancies, the remaining 3 trials contained patients with malignant or non-malignant hematonosis together. Six trials administered umbilical cord blood (UCB) HSCs, six trials delivered peripheral blood (PB) HSCs, four trials included patients received UCB, PB or bone marrow (BM) HSCs, whereas 3 trials didn’t report the source of HSCs. Four trials infused HLA-identical HSCs, thirteen trials delivered HLA haploidentical HSCs, the remaining 2 trials failed to mention. MSCs were extracted from BM in 9 trials, UCB in 8 trials, and two trials failed to cover the source of MSCs. In the intervention arms, MSCs were administered at a dose of less than 1×106 cells/kg in 4 trials, between 1×106 and 5×106 cells/kg in 11 trials, more than 5×106 cells/kg in 2 trials, and other 2 trials didn’t give information about this. The median durations of follow-up were within 1-year in 2 trials, between 1 and 2 years in 7 trials, between 2 and 3 years in 4 trials, 3 years and more in 4 trials, in the remaining two trials, the durations of follow-up varied greatly between groups, which were (3-28) and 7.4(1-22) months in MSCs groups, (32-110) and 24(1-107) months in control groups, respectively.
All patients received intensive conditioning regimens, GVHD prophylaxis and supportive care. Patients in the control groups underwent HSCT alone. Patients in the experimental groups received co-infusion of MSCs with allogeneic HSCs, both of which were administrated within day ‘0’ whenever allowed by the patient’s condition, otherwise within the coming 24h. The main outcomes were engraftments of platelet and neutrophil, acute and chronic GVHD, secondary outcomes included relapse rate, overall survival, non-relapse mortality or treatment related mortality, and immune reconstitution.
Risk of Bias analysis
Figure2 showed the quality assessment results for each study. No trial included more than 100 participants and some trials recruited participants even less than 20 [11, 24, 33-35]. Most studies in the 6 RCTs were at low risk of bias, but the 13 nRCTs were with higher risk according to the predefined methodological quality assessment tool.
Engraftment
Four RCTs and 10 nRCTs provided sufficient information of the neutrophil engraftment that differed from 10.5 to 29.82 mean days for the experimental group and from 12.31 to 28.1 mean days for the control group. We estimated the mean and standard deviation (SD) from the given sample size, median and range [25], Ghavamzadeh 2010 [37] and Kang 2017 [30] were not included in meta-analysis of this results as they only supplied the median values. Data from Baron 2010 [3] were ruled out for it defined neutrophil count of ≥1.0×109 cells/L as the standard of neutrophil engraftment. Results from Liu 2011 [17] and Ghavamzad 2017 [5] were not included because they monitored white blood cell (WBC) engraftment instead of neutrophil engraftment. Both meta- analysis of RCTs with 130 participants and nRCTs with 341 participants indicated that patients received MSCs co-infusion had a shorter time of reaching neutrophil recovery compared with the control group (4 RCTs: SMD -1.20, 95% CI -2.32 to -0.08, p = 0.04, I² = 86%; 10 nRCTs: SMD -0.54, 95% CI -1.05 to -0.03, p = 0.04, I² = 74%; Fig. 3a&b).
With regard to the platelet engraftment, we did not include the study by Ghavamzadeh 2010 [37] and Kang 2017 [30] for lack of usable data; data from the studies by Baron 2010, Ning 2008 and MacMillan 2009 [3, 20, 31] were not included because they defined platelet count of ≥100×109 cells/L or ≥50×109 cells/L as the standard of platelet recovery. As a result, only 4 RCTs and 10 nRCTs were selected for synthesis, the engraftment time differed from 8.71 to 52.05 mean days for MSCs co-infused groups and from 16.02 to 78.94 mean days for the controlled groups. Both RCTs with 157 participants and nRCTs with 381 participants revealed that the patients from the MSCs co-infusion group had a faster recovery of platelet than those from HSCT alone group (4 RCTs: SMD -0.60, 95% CI -1.17 to -0.02, p = 0.04, I² = 63%; 10 nRCTs: SMD -0.70, 95% CI -1.24 to -0.16, p = 0.01, I² = 79%; Fig. 3c&d).
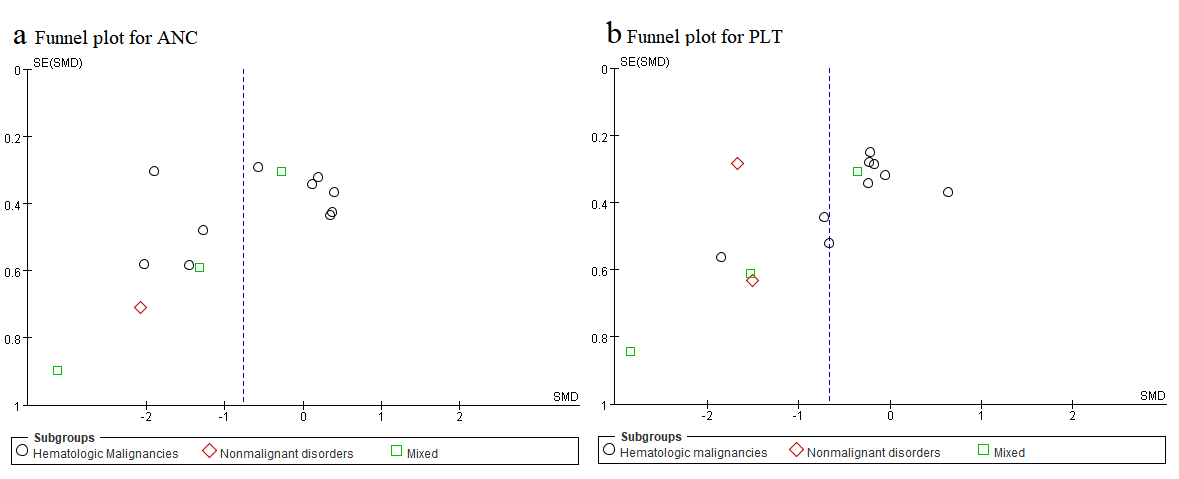
According to the funnel plot as showed in Additional file 6, publication bias was obvious for the outcomes of ANC and PLT engraftment. Meanwhile, statistical heterogeneity existed as indicated by the Tau²,Chi2 and I2 tests (Fig. 3a,b,c&d). Thus, we adopted random-effect model and performed sensitivity one-out analyses to estimate the relative contribution of each single study to the overall heterogeneity. When the study of Wu 2013b [35] was abandoned, the score of I2 sharply decreased from 63% to 0% in the meta-analysis of PLT engraftment in RCTs, which may be accounted by that it was the only trail that used MSCs in excess of 5×106 cells per kilogram; no significant I2 changes were observed in the other 3 meta-analysis.
In addition, we conducted subsets analyses (details were shown in Additional file 7) according to the dose of MSCs where all the studies were sorted into three groups. The study of Xiao 2013 [24] was excluded as it failed to document the dosage of MSCs. These analyses manifested that with the increase of MSCs dose, hematopoietic recovery was more effective. Although the results of subsets in nRCTs with MSCs among 1×106 to 5 ×106 cells per kilogram were not obvious, which may partly be attributed to the potential confounders of the study design. However, as the number of included studies and sample size in some subgroups were limited, all these results should be explained with caution.
GVHD
The incidence of grade Ⅰ-Ⅳ aGVHD was reported in 3 studies [17, 20, 35]. Study of Ghavamzad 2010 [37] only provided the data of grade Ⅲ-Ⅳ aGVHD; Mareika, 2016 [32] covered the occurrences of grade Ⅱ-Ⅳ and grade Ⅲ-Ⅳ aGVHD; the study of Xiang 2017 [10] wasn’t included as it did not report this outcome. Among the 13 nRCTs, nine studies reported the incidence of overall aGVHD; two [3, 31] provided only the data of grade Ⅱ-Ⅳ aGVHD; and the remaining 2 studies [24, 29] did not mention this outcome.
Regarding the incidence of grade Ⅰ-Ⅳ aGVHD, no statistical significance was observed in the meta-analysis including 3 RCTs with 98 cases (RR 0.84, 95% CI 0.59 to 1.19, P = 0.33, I² = 0%; Fig. 4a). Whereas in the meta-analysis including 9 nRCTs with 377 participants, it showed that patients with MSCs co-infusion had a significantly lower rate of grade Ⅰ-Ⅳ aGVHD incidence than the control group (RR 0.74, 95% CI 0.60 to 0.91, P = 0.005, I² = 0%; Fig. 4b). No difference was found between groups in outcomes of grade Ⅱ-Ⅳ, grade Ⅲ-Ⅳ and grade Ⅰ-Ⅱ aGVHD, from neither meta-analysis with RCTs nor that with nRCTs (Fig.4a&b).
Among the19 candidate studies, three [3, 29, 37] did not provide information about cGVHD incidence, two [11, 32] presented only the incidence of extensive cGVHD without data about the number of people who developed limited cGVHD. As a result, 4 RCTs with 156 participants (RR 0.53, 95% CI 0.33 to 0.87, P = 0.01, I²= 25%; Fig. 5a) and 10 nRCTs with 380 participants (RR 0.50, 95% CI 0.33 to 0.75, P = 0.001, I²=0%; Fig. 5b) were separately included in meta-analysis for the overall occurrence of cGVHD, both results of RCTs and nRCTs suggested that MSCs co-infusion could significantly reduce the overall incidence of cGVHD.
Specifically, in the outcome of limited cGVHD, no statistical significance was found between groups. However, patients in the MSCs group had a lower risk of extensive cGVHD compared with the control groups, as demonstrated by the meta-analysis with 8 nRCTs (RR = 0.37, 95% CI 0.17, 0.81, I² = 0%, P = 0.01; Fig 5b), meanwhile, there was a slightly trend from meta-analysis with 4 RCTs (RR = 0.44, 95% CI 0.17, 1.09, I²= 0%, P = 0.08; Fig. 5a).
Both funnel plots for aGVHD and cGVHD (Additional file 8) showed asymmetry, indicating the existence of publication bias. The statistical heterogeneity was not significant as indicated by the Tau²,Chi2 and I2 tests.
Overall Survival
Totally, there are 14 trials estimated the effect of MSCs co-infusion on overall survival of HSCT recipients, of which four studies were excluded [11, 5, 12, 13] for they failed to provide sufficient information that could be transformed into logHR and SE. With the rest of 4RCTs (164 participants) and 6 nRCTs (231 participants), the outcomes of meta-analysis (HR 1.54, 95% CI 0.81 to 2.93, P = 0.18, I² = 0%, Fig. 6a; HR 0.60, 95% CI 0.35 to 1.02, P = 0.06, I² = 34%, Fig. 6b; respectively) suggested no statistically significant difference of OS between groups. Publication bias was not obviously visualized from the funnel plot of OS, which was shown in Additional file 9a. Statistical heterogeneity was not significant as indicated by the Tau²,Chi2 and I2 tests.
Relapse Rate
Eleven studies reported the occurrence of relapse in both the MSCs group and the control group, but studies by Ball 2007 [13] and Daganzo 2009 [28] were excluded for reason of varied follow-up time between groups. Both the meta-analysis for 5 RCTs with 186 participants and 4 nRCTs with 184 participants (RR 1.34, 95% CI 0.74 to 2.43, P = 0.34, I² = 13%, Fig. 7a; RR 0.74, 95% CI 0.45 to 1.22, P = 0.24, I² = 0%, Fig. 7b; respectively) suggested no difference between patients given MSCs co-transplantation and those were not. Apparent publication bias was observed from the funnel plot of RR (Additional file 9b) and statistical heterogeneity was not significant as indicated by the Tau²,Chi2 and I2 tests.
TRM/NRM
For the non-relapse mortality or treatment related mortality (TRM/NRM), the meta-analysis results varied between the 3 RCTs with 100 participants and the 3nRCTs with 97 participants (OR 0.59, 95% CI 0.20 to 1.73, P = 0.34, I² = 0%, Fig. 7c; OR 0.18, 95% CI 0.06 to 0.54, P = 0.002, I² = 0%, Fig. 7d; respectively). But all of the odds ratios are no more than 1 and no statistical heterogeneity was observed, we could draw that there was still a slightly trend that patients infused with MSCs may have a lower risk of TRM/NRM. Of which the funnel plot was not applicable for the small number of studies. The statistical heterogeneity was not significant as indicated by the Tau²,Chi2 and I2 tests.
Immune reconstitution
Multiple studies had investigated the effect of MSCs co-transplantation in allo-HSCT on the immune reconstitution. However, it was difficult to combine all these data from each trial because of varied parameters and time points, we just made a qualitative description.
In the study of Ball 2007, the recovery time of natural killer cells at 28 days post transplantation was faster in recipients received MSCs co-infusion compared with the controls [13]. The research by Xiang 2017 [10] showed that the levels of lymphocytes subpopulations and immunoglobulins in patients treated with MSCs were statistically higher than the control group at 1st, 3rd and 6th month post transplantation. While the other seven trials [3, 5, 11, 17, 28, 32, 34] found no differences in the time of lymphocyte recovery post transplantation between two groups (details were shown in Additional file 5).
Analyses of patient subgroups
In the end, we conducted subgroup analysis based on the type of disease (malignant versus nonmalignant), HLA matching (HLA identical versus haploidentical) and average age (children and adolescents versus adults) by combining all the RCTs and nRCTs together (details were presented in Additional file 10-15; merged results were shown in table 3).
For malignant patients, risks of developing aGVHD, cGVHD and NRM were significantly reduced with MSCs co-transplantation; while for those with nonmalignant disorders, MSCs co-transplantation could accelerate hematopoietic recovery in both aspects of ANC and PLT engraftment.
Recipients who received HLA-identical grafts could benefit in outcomes of cGVHD and OS from receiving MSCs co-transplantation. Whereas for those who undergoing HLA-haploidentical HSCT, MSCs co-transplantation could play a significant positive role in the outcomes of hematopoietic reconstitution (both ANC and PLT engraftment), significantly reduce the risk of developing GVHD (both aGVHD and cGVHD) as well as TRM/NRM.
For adults, people received MSCs co-transplantation could have a lower incidence of cGVHD than those were not. While for individuals younger than 18, the intervention of MSCs co-transplantation could improve hematopoietic reconstitution (both ANC and PLT engraftment), and reduce the risk of developing GVHD (both aGVHD and cGVHD) as well as TRM/NRM obviously.
{kind=link}