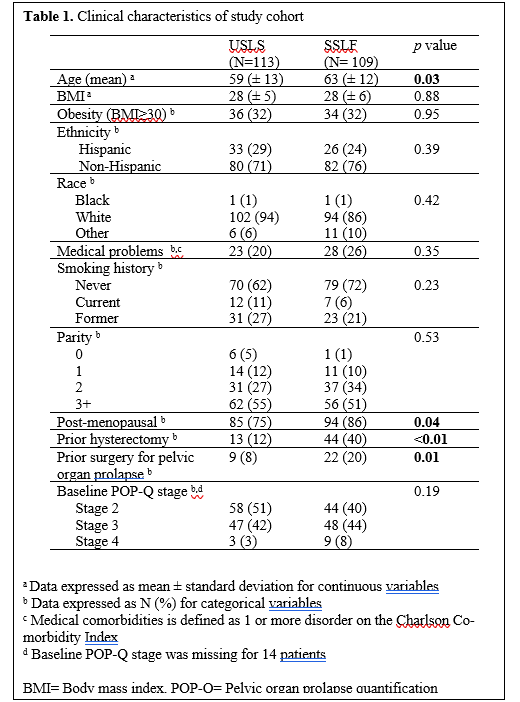
Between 3/2017-8/2019, 243 patients underwent L-USLS or SSLF. One patient in the L-USLS cohort was excluded due to planned concomitant bowel resection and 10 patients in the SSLF cohort were excluded (7 due to vaginal mesh use, 1 due to vaginal mesh excision, 1 due to concomitant umbilical hernia repair, and 1 due to sphincteroplasty). A total of 113 women in the L-USLS and 109 women in the SSLF cohort were included in the analysis. Overall, baseline characteristics were similar between the two groups (Table 1). Women in the SSLF cohort were older than those in the L-USLS cohort (63 vs 59, p =0.02). In addition, women who underwent SSLF were more likely to be post-menopausal, have a prior hysterectomy, and have a prior surgery for pelvic organ prolapse (all with p <0.05). There were no differences in POPQ measurements between groups, p=0.86.
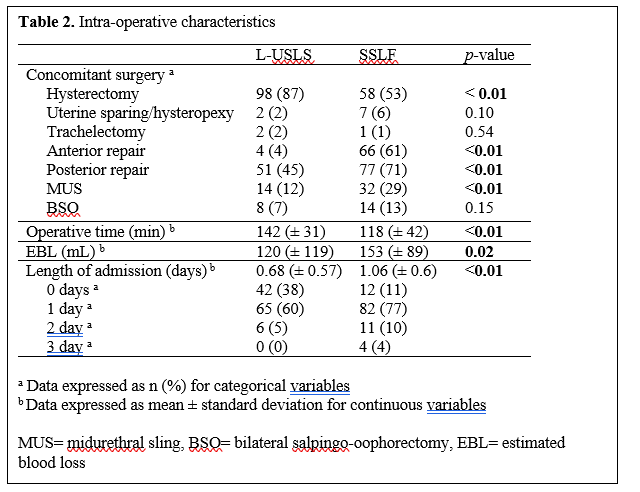
Concomitant procedures and intraoperative data are presented in Table 2. Hysterectomy was performed in 87% of patients in the L-USLS cohort and 54% of patients in the SSLF cohort (p <0.01). Uterine sparing hysteropexy was performed in 9 patients; 2 in the L-USLS group and 7 in the SSLF group. Fewer anterior and posterior vaginal repairs were required for L-USLS compared to SSLF (4% vs 61% and 45% vs 71% respectively, both p <0.01). Total operative time was longer for the L-USLS cohort (140 vs 118 minutes, p <0.01). In addition, average blood loss was lower in the L-USLS cohort (120 vs 152 mL, p = 0.02) and length of admission was shorter in the L-USLS cohort (0.68 vs 1.06 days, p= <0.01). After adjusted for age, co-morbidities, and concurrent procedures (hysterectomy, anterior repair, posterior repair, BSO, and MUS), the length of admission and operative time remained statistically significant, but blood loss was no longer statistically significant.
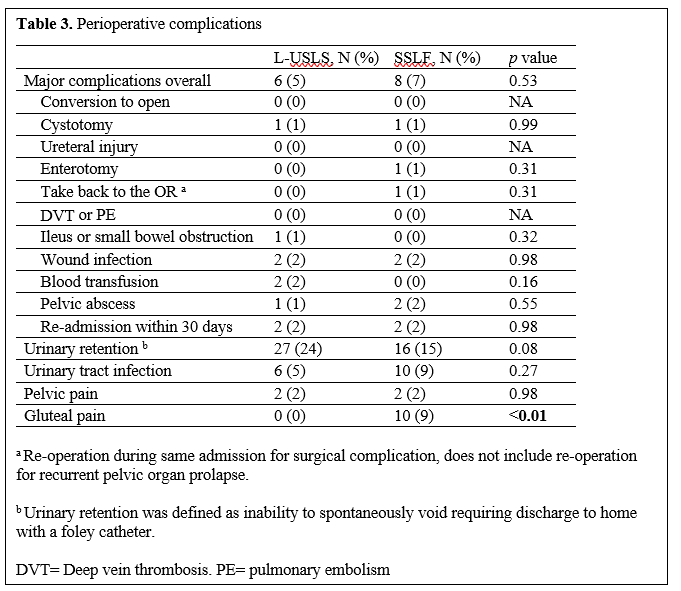
There was a similar rate of perioperative complications in both groups (5% vs 7%, p= 0.55), Table 3. Using the Clavien-Dindo grading scale, in the L-USLS cohort there were two Grade 1 complications, five Grade 2 complications and two Grade 3 complication. In the SSLF cohort, there were two Grade 1 complications four Grade 2 complication, and three Grade 3 complications. There was one cystotomy in both the L-USLS and SSLF cohorts, and one bowel injury in the SSLF cohort. All were recognized intraoperatively and repaired without postoperative sequelae. One patient in the SSLF cohort was taken back to the OR due bleeding at the vaginal cuff that was identified in the post-operative care unit. One patient in the L-USLS group experienced a small bowel obstruction which required bowel resection. This patient had a complex surgical history with resulting dense abdominal adhesions. There were two readmissions in each group; two for pneumonia, one for enterocolitis, and one for vaginal bleeding which did not require any intervention. Univariable logistic regression comparing outcomes between the two groups did not identify risk factors for complications (data not shown). Multivariable logistic regression was not performed due to the small number of complications identified.
Postoperative urinary retention was common; it affected 24% of women in the L-USLS cohort and 15% of women in the SSLF cohort (p = 0.08). Two women in the L-USLS cohort experienced persistent urinary retention after sling placement and required sling release. Urinary retention resolved in all women in the SSLF cohort. Urinary tract infection occurred in 5% of women in the L-USLS cohort and 9% of women in the SSLF cohort (p=0.27). Nine women in the SSLF cohort experienced gluteal pain post-operatively, one required removal of sutures due to persistent pain. Two women in each cohort experienced new pelvic pain post-operatively, one woman in the L-USLS cohort required local analgesic injection for treatment.
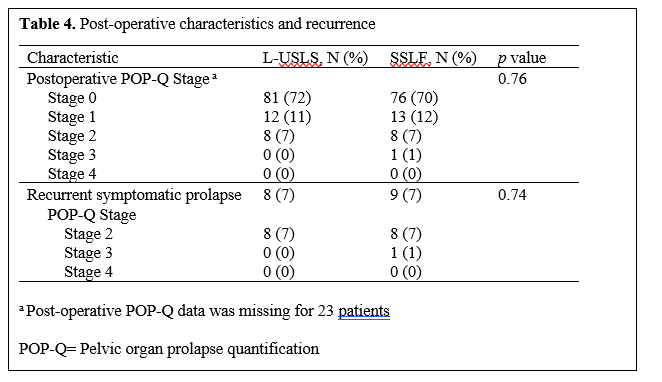
The median follow up in this cohort was 7 weeks (IQR 5.4-22.2 weeks), defined as date of surgery to last office appointment. Immediate post-operative POP-Q information was available for 89% of patients in the L-USLS cohort and 91% of patients in the SSLF cohort. At last clinic follow up, approximately 82% of patients in both groups had Stage 0 or Stage 1 prolapse (p= 0.76). In patients with follow up beyond 3 months, we aimed to characterize the short-term rate of recurrent prolapse. Prolapse recurrence was defined as prolapse of any compartment (anterior, apical, or posterior) beyond the hymen or retreatment for prolapse by either surgery or pessary. Recurrent pelvic organ prolapse occurred in 8 patients in the L-USLS cohort and 9 patients in the SSLF cohort (7% vs 7%, p= 0.43). Apical prolapse occurred in 5 patients in the L-USLS cohort, four underwent laparoscopic sacrocolpopexy and one underwent SSLF. Two patients in the SSLF cohort had apical prolapse, one underwent repeat SSLF and one elected for conservative management with physical therapy.
{kind=link}
{kind=link}
{kind=link}
{kind=link}