Our study aimed to investigate the microstate parameters in patients with unconsciousness and to evaluate the relationship of these parameters with the level of consciousness and clinical assessment scales. For this purpose, we compared the microstate analyses of the resting state EEGs of VS, MCS- and MCS + patients and healthy controls. This study is one of the few studies examining the microstate parameters of patients with DOC. In the results of our study, we determined that patients with DOC differed from healthy controls with changes in microstate parameters. In particular, we found that the transition probabilities of microstate D parameters and some microstate maps (A > B, B > A, D > B, C > D, D > C) correlated with consciousness level and clinical assessment scales. We believe that our findings will contribute to the consciousness disorders and microstate analysis literature.
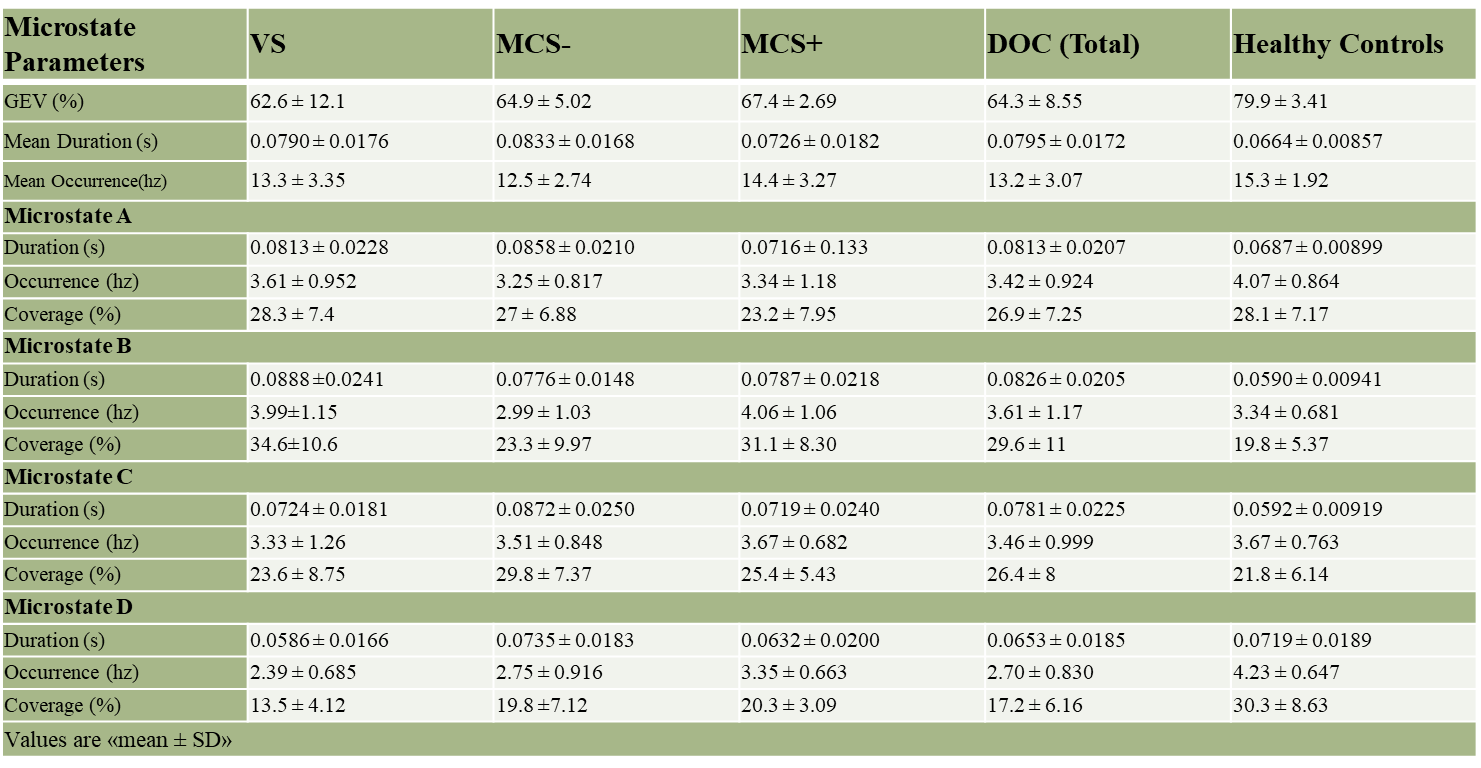
We analyzed the resting-state EEG data of VS, MCS, and healthy controls by separating them into four microstate maps. There was no significant topographic difference between the mean microstate maps of each group. Topographic maps of healthy controls were consistent with the literature (Khanna et al., 2015; Koenig et al., 2002; Michel & Koenig, 2018). This situation is essential in terms of comparability with the literature. While examining the microstate parameters, we used the mean topographic maps of our healthy control data, which formed our normals, as a template in all groups. According to this, In the DOC group, the total explained variance of the four microstate maps was significantly lower, as we expected. The literature has repeatedly reported that the total explained variance rate of the four microstate maps is above 70% in studies performed with healthy controls (Khanna et al., 2015; Koenig et al., 2002; Michel & Koenig, 2018). The decrease in the variance explained in the patient group shows that brain oscillations differ from healthy controls. However, we could not find a significant difference between the MCS and VS groups. Therefore, we think that the explained variance rate is a general parameter in showing consciousness disorders but not a sensitive enough indicator.
In DOC patients, the mean duration of microstates was significantly longer, and their frequency was significantly less. The literature has reported that the mean microstate durations increase and the frequencies decrease with age (Koenig et al., 2002). In a study conducted in 2012, it was determined that the average microstate durations were prolonged during deep sleep (NREM 3) (Brodbeck et al., 2012). In addition, in a recent study, it was reported that the mean microstate durations were prolonged in dementia with Lewy bodies, and this prolongation was negatively correlated with the functional connectivity of the basal ganglia network and the thalamic network; It was emphasized that this situation might be related to the slowdown in mental activities (Schumacher et al., 2019). However, studies conducted in recent years have shown that the average microstate parameters are prolonged in Alzheimer's patients (Tait et al., 2020). The increased mean duration was suggested as a finding reflecting cognitive decline, indicating that the conversion of microstate parameters to each other slowed down (Tait et al., 2020). There was no age difference between our patient and healthy groups. Mean duration and total frequency values did not successfully differentiate VS and MCS. Similar to the variance rate explained, we think these parameters are a general finding showing that the transition between microstates in patients with cognitive impairment slows down. Therefore brain oscillations slow down, but they are not sensitive enough to show the severity of the disease.
In DOC patients, the mean duration of Microstate A was prolonged, and its occurrence decreased. A study conducted in 2018 suggested that the incidence of Microstate A was a finding reflecting the prognosis of DOC patients (Stefan et al., 2018). Microstate A is defined as a network associated with the auditory network. The auditory network is associated with the bilateral superior and middle temporal gyrus, and the left middle frontal gyrus regions show functional connectivity (Britz et al., 2010). The changes we see in the parameters of microstate A may result from these regions being affected in DOC patients. In addition, Microstate A parameters did not distinguish VS-MCS sensitively, and it was not a sensitive parameter in showing the severity of the disease.
We found that the mean duration of microstate B was prolonged, and its coverage increased in DOC patients. Studies report that the duration or coverage of B is increased in patients with Parkinson's and dementia with Lewy bodies, and its duration is decreased in patients with schizophrenia (Chu et al., 2020; Nishida et al., 2013; Schumacher et al., 2019). Microstate B is a network location associated with the visual network. In this network, bilateral occipital areas and related subcortical structures show functional connectivity (Britz et al., 2010). Changes in MS B may indicate that these areas are affected in DOC patients. This parameter was also not found sensitive enough to show the severity of the disease.
In microstate C, similar to MS B, the mean duration was prolonged, and the coverage increased in DOC patients. Microstate C is a map associated with the saliency network. The anterior cingulate cortex, medial cingulate gyrus, left inferior frontal gyrus, left claustrum, right inferior frontal gyrus, and right amygdala show functional connectivity in this defined network (21). The changes we found in this parameter, in addition to reflecting the involvement of these areas, were still not sensitive enough to show the severity of the disease.
In microstate C, similar to MS B, the mean duration was prolonged, and the coverage increased in DOC patients. Microstate C is a map associated with the saliency network. The anterior cingulate cortex, medial cingulate gyrus, left inferior frontal gyrus, left claustrum, right inferior frontal gyrus, and right amygdala show functional connectivity in this defined network (Britz et al., 2010). The changes we found in this parameter, in addition to reflecting the involvement of these areas, were still not sensitive enough to show the severity of the disease.
When we examined the parameters related to the microstate D maps, we found that the coverage and occurrence decreased. These parameters also differed significantly between MCS and VS and correlated with clinical assessment scales. A study conducted in 2018 reported that the coverage of microstate D is the most sensitive parameter in differentiating VS and MCS patients (Stefan et al., 2018). The increasing coverage of microstate D was presented as a parameter indicating the severity of the disease. Surprisingly, in our study, the coverage in microstate D was associated with higher clinical scores, namely increased awareness. This difference may be due to methodological changes, we examined the 2–20 Hz frequency band, but the result found in the literature was only in the alpha frequency band. In a study conducted in 2012 examining the relationship between sleep stage microstates, it was reported that the incidence and frequency of Microstate D decreased as sleep deepened (Brodbeck et al., 2012). Publications show that microstate D's topography and parameters are also affected in Parkinson's disease and Alzheimer's disease (Chu et al., 2020; Ignacio Serrano et al., 2018; Pal et al., 2021; Tait et al., 2020). Microstate D is a map associated with the frontoparietal network, working memory network, and attention network (Britz et al., 2010). In particular, areas lateralized to the right, covering the right upper and middle frontal gyrus and the right upper and lower parietal lobules, show functional connectivity in this network. We think that the frequency and ratio of this map, which is associated with the frontoparietal network, are the most sensitive parameters in distinguishing DOC patients and showing the severity of the disease. Results of previous resting state network studies in DOC patients highlight the coexistence of a common disorder involving the associative cortices such as the midline of the frontoparietal network (i.e., anterior cingulate cortex-mesiofrontal and posterior cingulate cortex associated with internal awareness or self-related processes) and lateral network (i.e., prefrontal and posterior parietal area associated with environmental awareness) (Beuthien-baumann et al., 2003; Juengling et al., 2005; Laureys, Goldman, et al., 1999; Laureys, Lemaire, et al., 1999; Lull et al., 2010; Nakao et al., 2010; Silva et al., 2010). It has been shown that the connection in the midline frontoparietal cortex, also called the default mode network (DMN), reflects the consciousness level of DOC patients (Vanhaudenhuyse et al., 2010). A map reflecting DMN in microstate maps has not been reported by Britz et al.. However, Microstate D is mainly associated with the lateral frontoparietal network; this map we showed in our study to be sensitively affected in DOC patients may also reflect DMN.
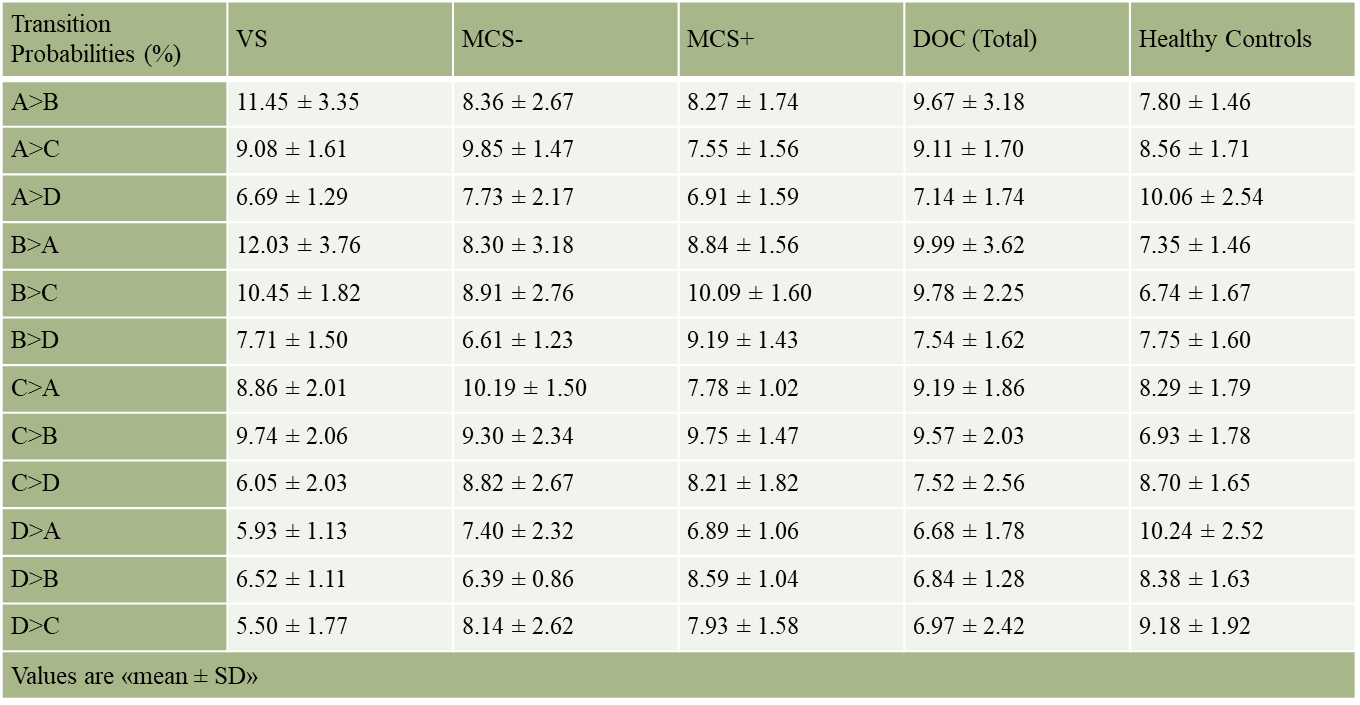
Examining the transition probabilities between microstate maps, we found that DOC patients are more likely to prefer transitions over Microstate B and less likely to transition over Microstate D. In particular, we found that A > B, B > A, D > B, D > C, C > D transitions were associated with clinical assessment scales. It is thought that transitions between microstates are not random (Khanna et al., 2015). More work is needed to link these transition possibilities with functional networks. Our study is the first to examine the probabilities of microstate transition in DOC patients and to investigate its relationship with clinical assessment scales.
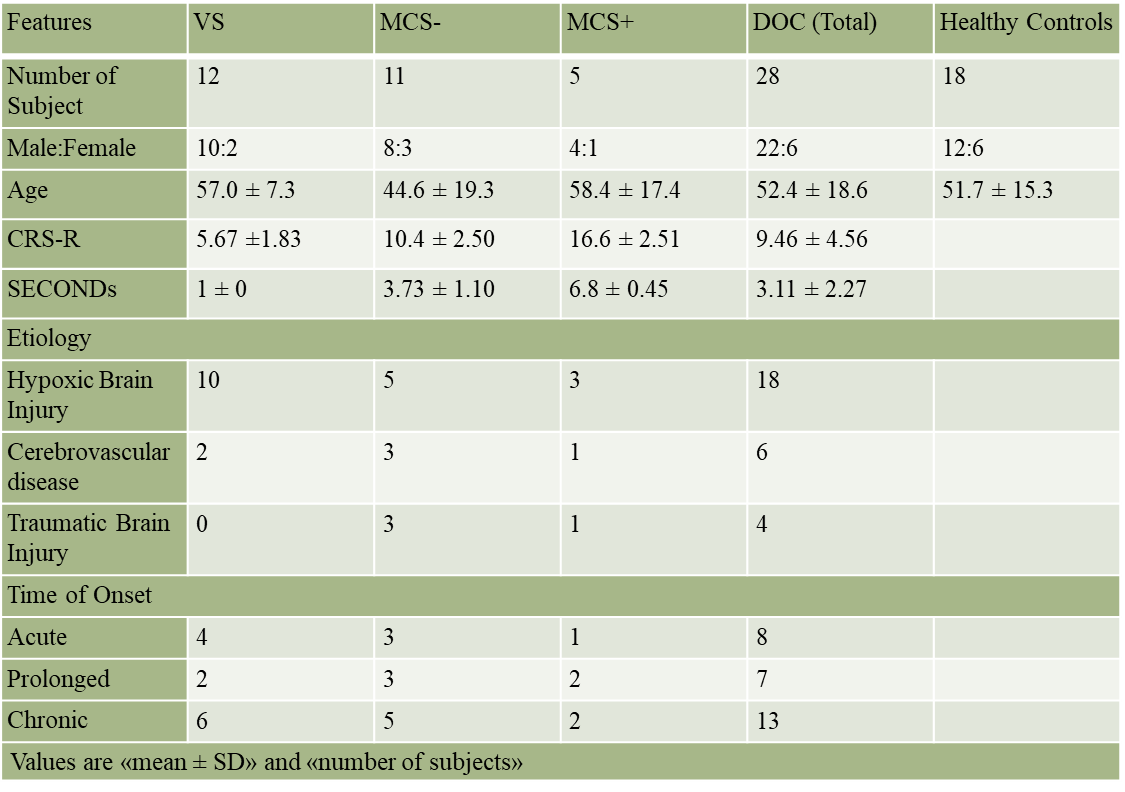
There are also some limitations of our study. First, we did not use a structural neuroimaging method in our study. The patient groups we examined were very heterogeneous. Different brain regions may be affected secondary to hypoxia, trauma, or cerebrovascular disease. In subsequent studies, structural brain imaging can also be used to provide better homogeneity of the groups. In our study, we examined four microstate topographies in the range of 2–20 Hz, which have been the most studied in the literature, as previously stated. Frequency ranges can be divided into the delta, theta, alpha, and beta frequencies; more detailed sub-analyses can be made, and more than four topographies can be examined; thus, more precise measurements can be made possible. Finally, we did not do a longitudinal follow-up in our study. In future studies, longitudinal follow-up can be carried out, comparing the prognosis of the patients with the microstate parameters, and the sensitivity of the microstate parameters can be investigated in determining the prognosis.
{kind=link}
{kind=link}
{kind=link}