In the DRC, school-age children are often neglected in malaria prevalence surveys, and therefore benefit less from malaria prevention measures compared to children under five years of age and pregnant women [57]. School-age children contribute to transmission because they may harbour a substantial malaria parasite reservoir [15, 45, 47, 49, 58], and thus represent a gap in the formulation of malaria containment strategies. Less attention has been given to investigating the genetic diversity of P. falciparum isolates in DRC compared to other malaria endemic countries.
This is the first study to provide a detailed assessment of allelic diversity and multiplicity of P. falciparum infections among the underserved school-age group in the DRC using the polymorphic regions of the genes coding for MSP1 and MSP2.
The purpose of the study was to evaluate the extent of P. falciparum diversity - including polyclonal infection frequency, the number of the alleles detected, and MOI - in asymptomatic and symptomatic individuals living in rural and urban areas of Kinshasa province, DRC. Our findings showed that no allelic families of pfmsp1 (K-, M-, and R-types) or pfmsp2 (F- and D-types) were exclusively restricted to either rural and urban settings, as well as asymptomatic and symptomatic infections; although the frequency of some alleles were more common in one site compared to another, in addition to differences based upon child health status.
The pfmsp2 gene was found to be genetically more diverse than the pfmsp1 gene in our study areas, in support of the findings of the majority of studies conducted in Africa [16, 34–36, 59]. This confirms that in many malaria-endemic African countries polymorphic pfmsp2 allelic families may be circulating in higher frequencies than those for pfmsp1. MSP1 block 2 has been proposed to be most significantly exposed to the host immune selective pressure based on the stable K-M-R frequency distribution in the endemic regions [25]. Escaping with 3 major alleles of MSP1 block 2 may have advantage compared to MSP2 which has only 2 major alleles. This may stimulate to diversity MSP2 repeat number polymorphism.
Symptomatic children have been shown to carry more polyclonal infections than asymptomatic children and those polyclonal infections increased with the level of parasitaemia regardless clinical status. In Cote d’Ivoire, Gnagne et al. (2019) found significant association of polyclonal infections measured by both pfmsp1 and pfmsp2 with an increase in parasitaemia but not with clinical status [60]; while in Southern Benin Lagnika et al. (2022) found that polyclonal infections were more prevalent in symptomatic malaria carriers than asymptomatic ones [61]. This may be due to the low power to amplify minor alleles in the low parasitemia samples.
Thus, further investigations are needed to establish the impact of clinical status and parasitaemia on multiplicity of infections.
Our study showed generally lower MOI than has been previously reported in the DRC, Cameroon, and Republic of Congo [33, 35, 36]. Conversely, our study showed higher MOI compared with reports from Grande Comore Island, Cote d’Ivoire, and Gabon [59, 62, 63]; while it was similar to an MOI report from Republic of Congo by Mayengue et al. (2011) [34]. These observations may indicate differences in malaria seasonal and transmission settings, and improvement of country-specific malaria intervention measures. Alternatively, it may be due to the heterogeneity of P. falciparum transmission which differs from one area to another, resulting in heterogenous malaria transmission rates throughout the area [49, 62, 63], as MOI measures malaria transmission or host acquired immunity or severity level [33, 53, 64]. For instance, some reports from the DRC and other countries showed a positive correlation of MOI with malaria recrudescence [33] and parasitaemia level [20, 34, 53]; and negative correlation between MOI and acquired immunity level [64]. Conversely, other studies did not find significant association of MOI with either parasitaemia or clinical status [36, 61]. However, the studies that established the relationship of MOI with either parasitaemia or clinical status did not associate them (parasitemia and clinical status), to minimize confounding factors. There is a need for further investigations to consider parasitaemia and clinical status together and their possible association with MOI. In Gabon and Grande Comore Island it has been shown that MOI may vary by region [63, 65], and decrease due to intervention measures and after the implementation of artemisinin combined therapies (ACTs) [62, 63].
Our study did not find a significant difference of overall MOI, pfmsp1 MOI, or pfmsp2 MOI between the two study areas (rural versus urban), despite the fact that a previous report from the same areas and time period showed that the odds of the transmission of Plasmodium infections were five-fold higher in the rural versus urban area [49]. However, the mean MOI in the rural area was slightly, but not significantly, higher than that in the urban one. In Senegal, Ndiaye et al. (2020) showed that MOI was significantly higher in a rural area than in an urban setting [65]. To date, the majority of studies have established: i) a correlation between genetic diversity of P. falciparum populations and the intensity of transmission in malaria-endemic areas, ii) that P. falciparum genetic diversity is higher in hyperendemic areas than in low-endemic settings [42, 66–68], and iii) polyclonal infection prevalence decreases with a reduction in malaria transmission [68–72]. Our data suggests that pfmsp1 and pfmsp2 allelic diversities are not influenced by the level of transmission between the two zones. However, lower polyclonal infections and MOI in Selembao urban HZ may reflect the lower malaria transmission level in that area, which agrees with studies conducted in hypoendemic areas [37, 49, 73]; and compared to the higher polyclonal infection found in Mont-Ngafula 2 rural HZ, which reflects its malaria hyperendemicity as shown in hyperendemic malaria areas in Africa [49, 74–76]. Hence, spatiotemporal analyses are needed in different provinces and in different areas within and among the DRC provinces to characterize and better understand the parasite complexity in the DRC.
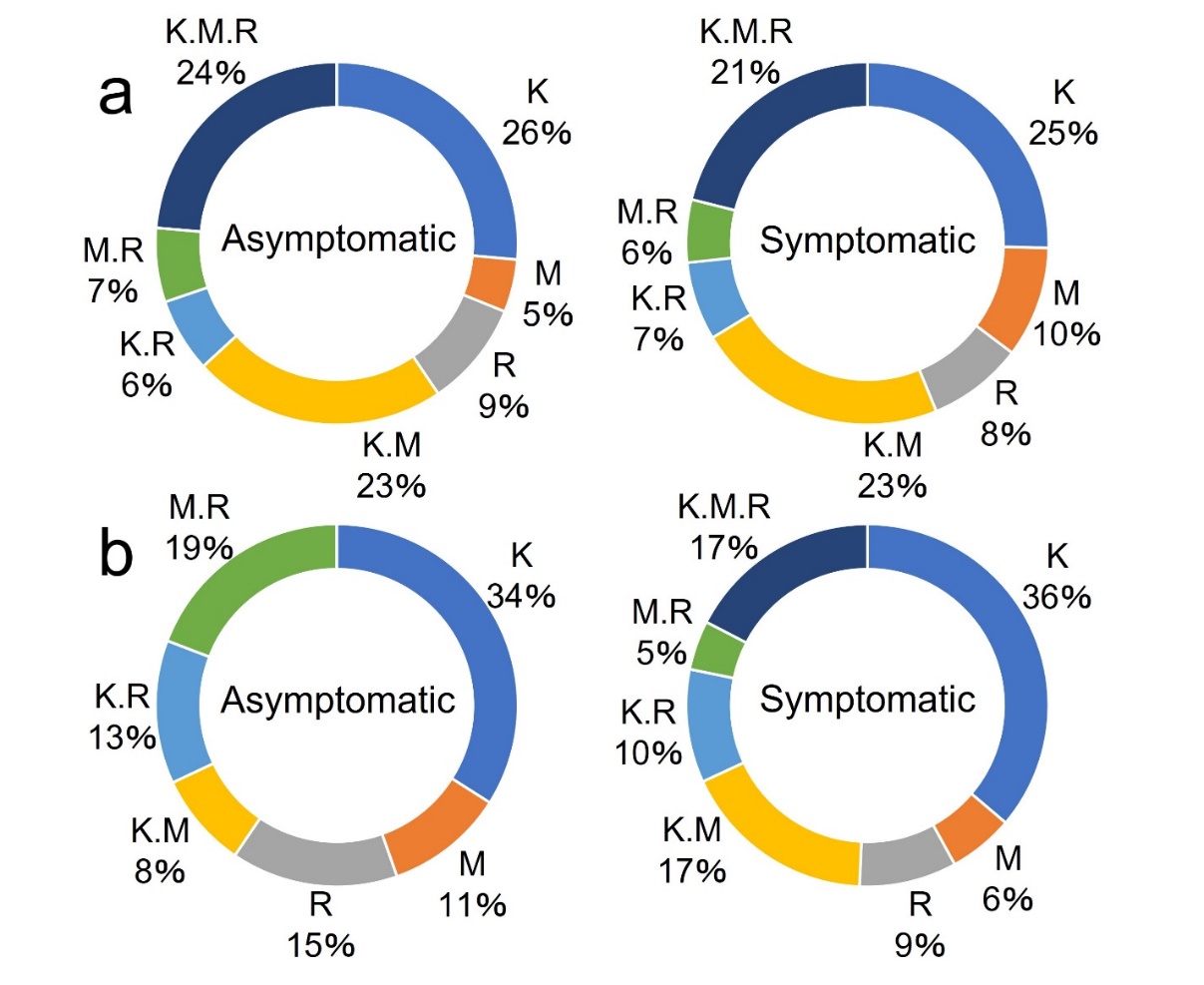
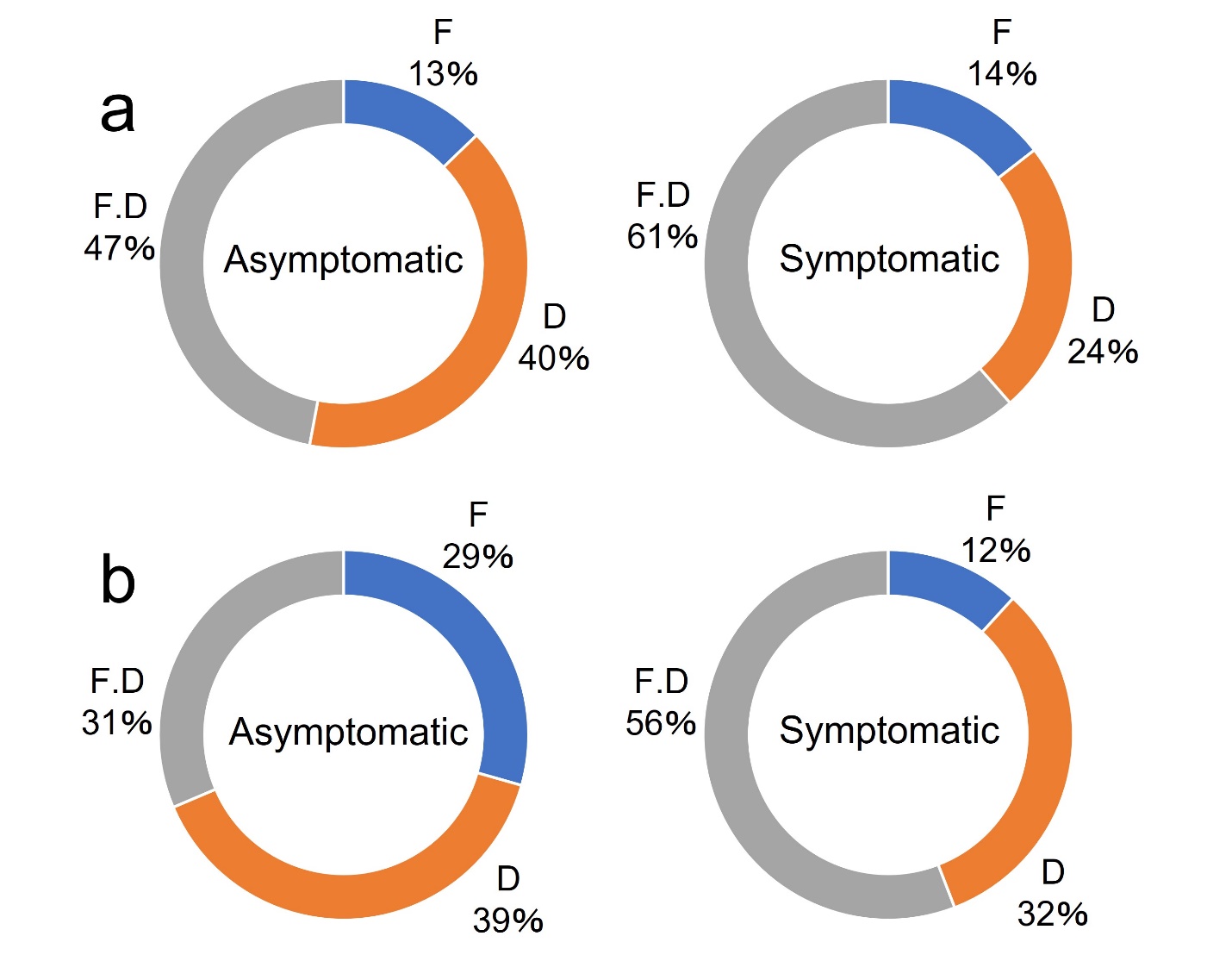
Our findings showed the predominance of single pfmsp1 K- and M-type alleles in P. falciparum mono-species infections and that of the K/M/R triple pfmsp1 alleles in mixed-species infection with P. falciparum regardless of malaria clinical status.For the pfmsp2 gene, the D-type allele was more frequent in P. falciparum mono-species infections, while the F/D-types double infection was more frequent in mixed-species infections in both symptomatic and asymptomatic carriers. The diverse distribution of pfmsp1/2 alleles within P. falciparum mono- and mixed-species infections may be explained based on findings from experimental [77, 78] and clinical [79, 80] studies that have shown cross-species immunity within hosts coinfected by multiple Plasmodium species. This situation may be influenced by within-host competition between species independent from the immunity: Tang et al (2019) showed that a mixed infection of two rodent malaria parasite species could increase the severity and parasite densities in the mouse host [81]. Studies are needed to assess the immunity-independent influence of mixed-infections of human Plasmodium within hosts.
In Southern Benin it has been shown that the prevalence of polyclonal infections and MOI as measured by polymorphisms in pfmsp1 and pfmsp2 were significantly lower in P. falciparum/P. malariae co-infected asymptomatic carriers compared to single species infection of P. falciparum and it was suggested that a decrease in genetic diversity and complexity of infection occurred in co-infection cases [82]. Conversely, our study showed an increase in polyclonal infection and MOI as measured by polymorphisms in pfmsp1 and pfmsp2 in infections with P. ovale and/or P. malariae co-infected with P. falciparum in asymptomatic subjects, although it was not significantly different in symptomatic subjects. Further studies are needed to provide more information on the consequences of within-host competition in mixed-species infections based on malaria clinical status.
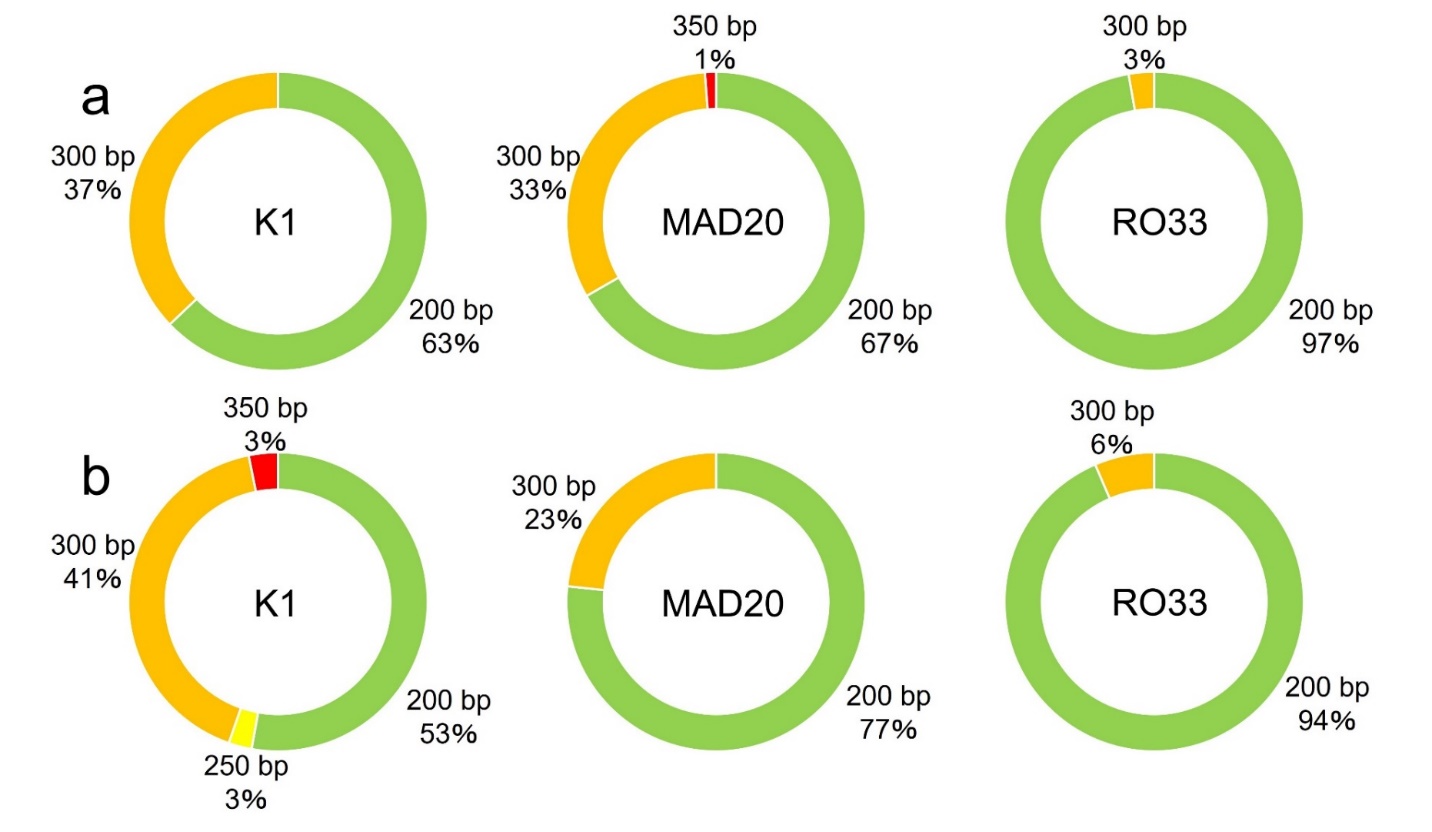
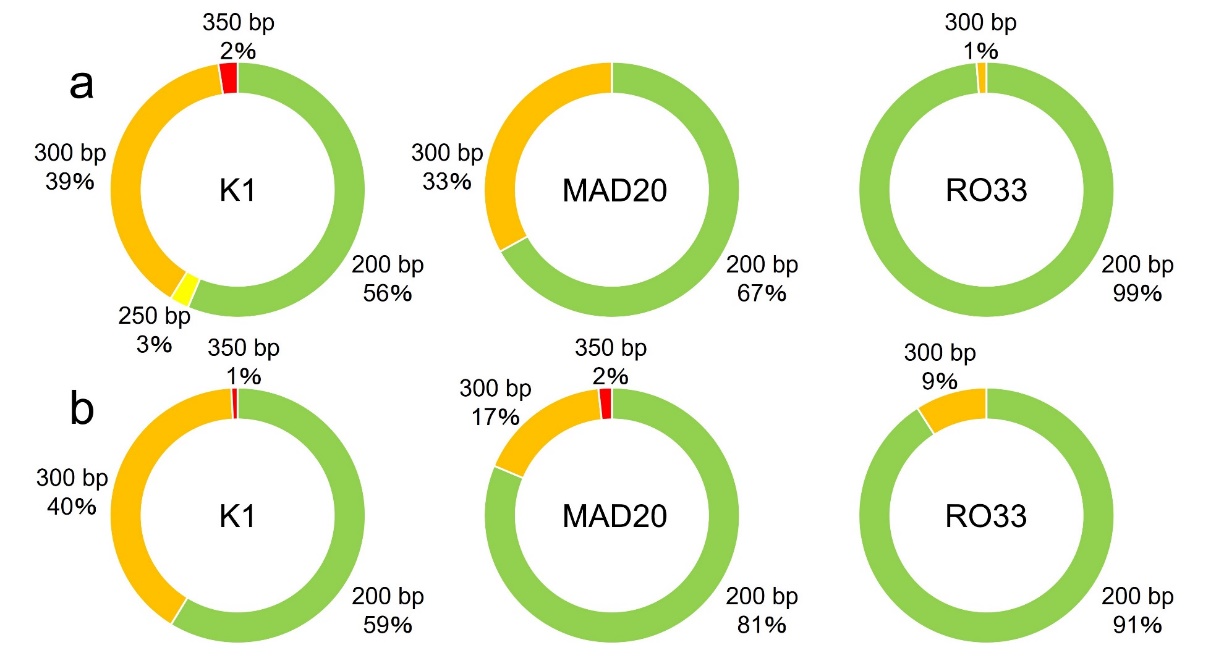
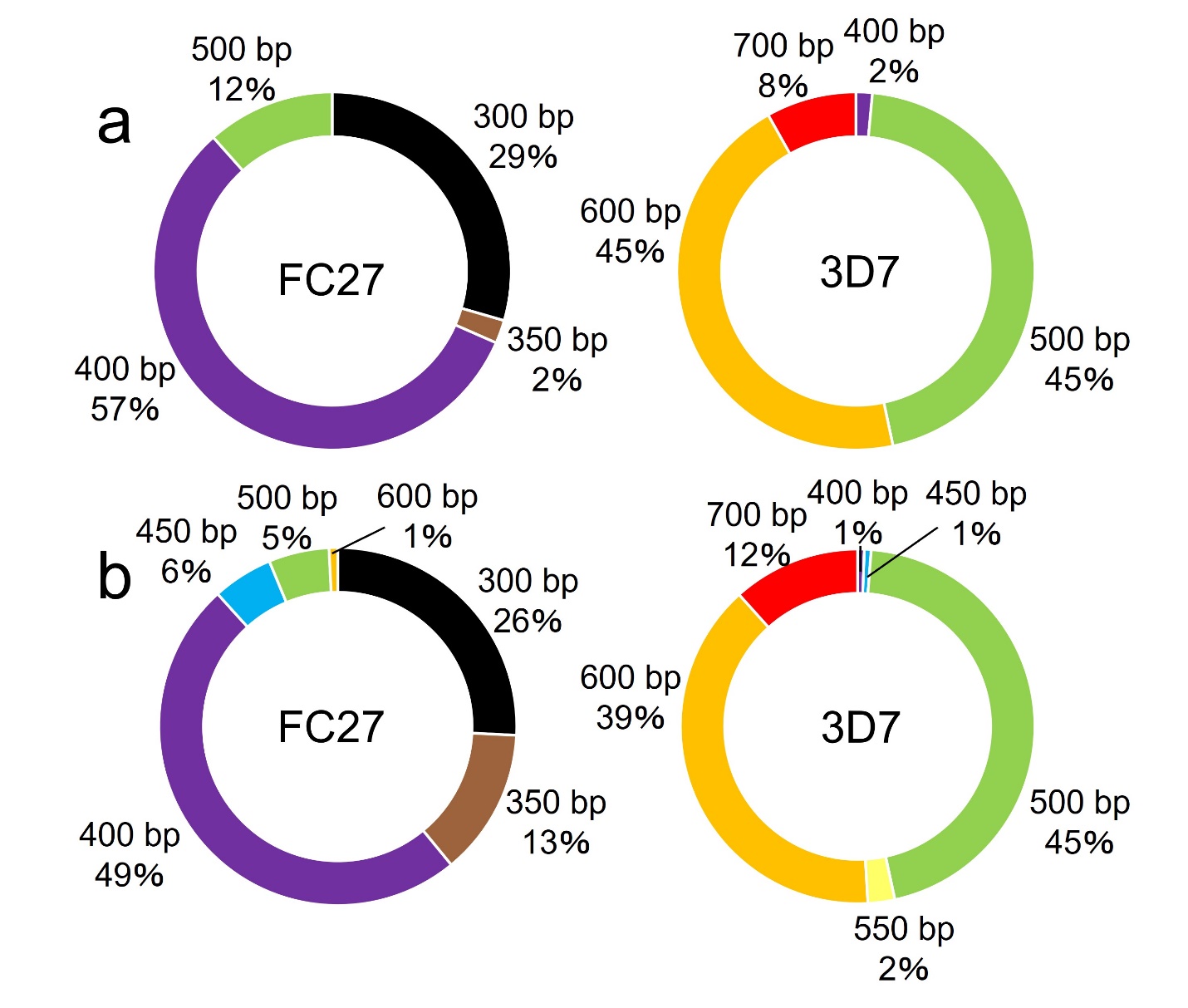
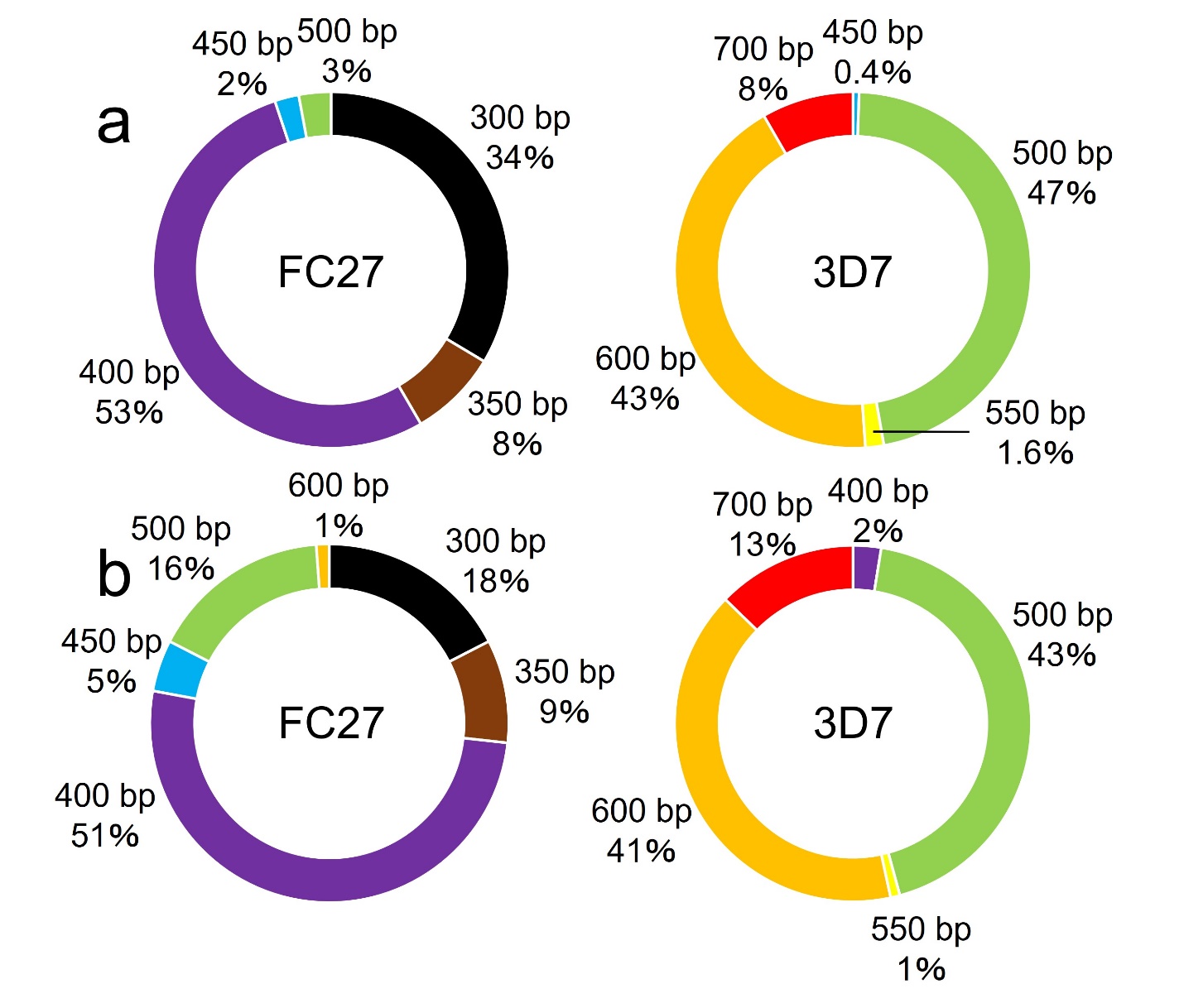
Our study found that for pfmsp1 the allele size around 200 bp dominated for all K-, M-, and R-types, regardless of the presence of symptoms and the rural and urban settings. This finding was also shown in Cameroon [19], Gabon [59, 83], Burkina Faso [16], Benin [84], and Republic of Congo [34]. For pfmsp2, the 400-bp F-type allele and the 500-bp D-type allele dominated, regardless of the presence of symptoms and the rural and urban settings. Among the F-type pfmsp2 allele, the 400-bp allele has also been shown to be frequent in Republic of Congo [34] and Burkina Faso [16]; whereas the 500-bp allele was more frequent in Cote d’Ivoire [59], the 600-bp allele in Gabon [59], and the 700-bp allele in Benin [84]. Among the D-type pfmsp2 allele, the 300-bp allele was more frequent in Republic of Congo [34], Cote d’Ivoire [59], and Burkina Faso [16]; while the 400-bp allele was more frequent in Gabon [59] and the 700-bp allele more frequent in Benin [84]. Future sequence analysis of genetic polymorphisms could confirm the similarities of these allelic families with those of other African countries [29, 35, 60, 83].
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}