Study population
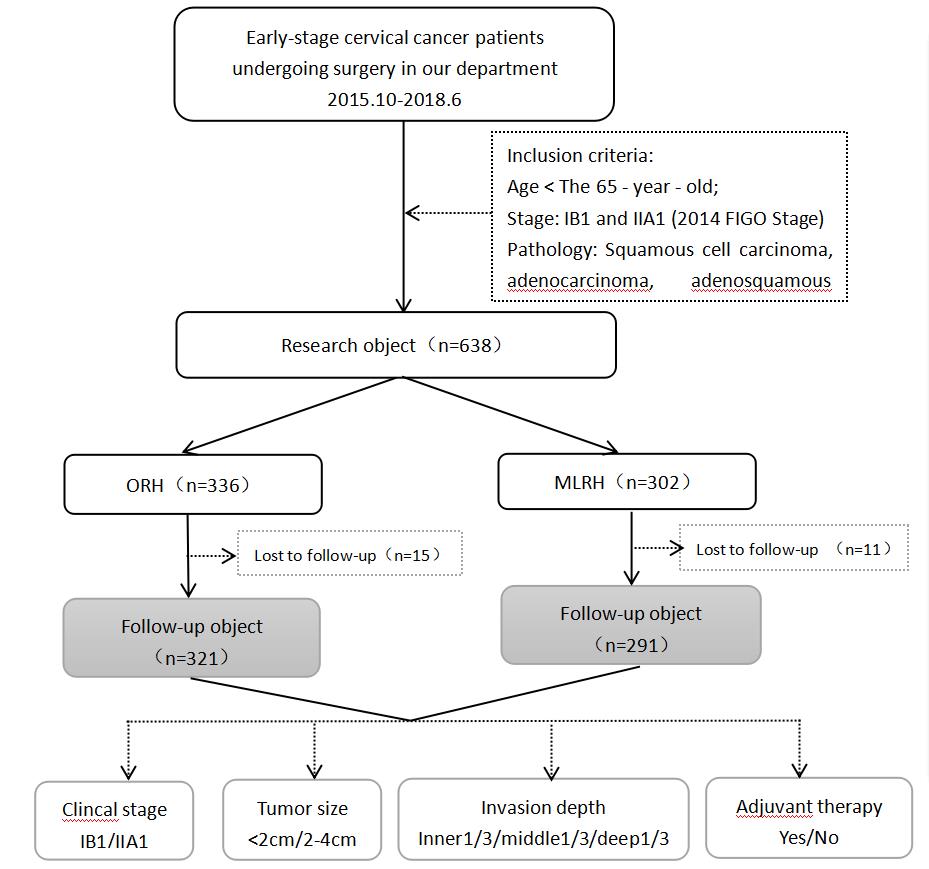
A total of 638 patients with clinical early stage cervical cancer undergoing radical hysterectomy between October 2015 and June 2018 were included. Patients were divided into the ORH group (n=336) or MLRH group (n=302). The patients selected the surgical approach. The study was approved by the local ethics committee and conducted in accordance with the Declaration of Helsinki as revised in 2013. The specific inclusion and grouping process is presented in the Additional file 1.
Inclusion criteria were as follows: 1) age < 65 years; 2) clinical stages: IB1 and IIA1 (2014 FIGO staging system); and 3) pathological type: squamous cell carcinoma, adenocarcinoma, and adenosquamous carcinoma. Exclusion criteria were as follows: 1) age > 65 years; 2) clinical stages: IA1, IA2, IB2, IIA2, IIB, III, and IV (2014 FIGO staging system); 3) histologic types: neuroendocrine carcinoma, clear cell carcinoma, serous carcinoma, small cell carcinoma, or minimal deviation adenocarcinoma; 4) neoadjuvant chemotherapy or radiotherapy before surgery; and 5) severe systemic underlying diseases, immune diseases, mental illness, or other malignancies.
Operative procedure
Based on Querleu and Morrow’s classification, all patients underwent primary type C hysterectomy and pelvic lymph node dissection (with or without para-aortic lymph node sampling). A subset of patients underwent double appendectomy. All surgeries were conducted in the same manner by a professional certified gynecologist.
ORH group
After induction of general anesthesia, patients were placed in the supine position. A median longitudinal incision was made from the symphysis pubis to 4 cm above the navel in the abdomen. The open pelvic cavity was explored, pelvic lymph node was dissected, and extensive hysterectomy was performed.
MLRH group
Patients adopted the bladder lithotomy position, and five puncture holes were selected after establishing artificial CO2 pneumoperitoneum. A series of measures were incorporated to prevent tumor spillage based on general laparoscopic procedures: 1) avoiding the use a uterine manipulator by using an acutenaculum to push and pull the suture for manipulating the uterus through the fifth puncture; 2) immediately bagging the whole pelvic lymph node after resection; 3) resecting the paracervical main sacral ligament and anterior lobe of the bladder cervical ligament first after lymph node dissection; 4) cutting off the vagina after stapler closure and removing the uterus after vaginal pouch suture; 5) flushing the open pelvic cavity repeatedly with double-distilled water throughout the operation; and 6) reducing the postoperative pneumoperitoneum pressure by maintaining the pneumoperitoneum pressure at 11 mmHg. Specific procedures are depicted in the Additional file 2.
Follow-up
All patients were followed up every 3 months in the first 2 years, every 6 months in the next 3–5 years, and then once a year. All patients (except those who were deceased) were followed up until December 31, 2020.
Research variables
General clinical characteristics included age, body mass index (BMI), clinical stage, histological grading, pathological type, tumor size, intermediate-risk and high-risk factors, and adjuvant therapy. Clinical stage referred to the FIGO staging method. To determine tumor size, preoperative evaluation of the maximum diameter of the tumor measured according to gynecological examination was performed. Intermediate-risk factors included tumor diameter, invasion depth, and vascular tumor thrombus positivity. High-risk factors included positive results for para-uterine and vaginal margin and lymph node metastasis. The pathological results of the patients included in this study suggested that both para-uterine and vaginal margins were negative; thus, they were excluded from the comparison. Adjuvant treatments included radiotherapy, chemotherapy, or concurrent chemoradiation therapy (CCRT) [15], which referred to the Sedlis standard.
Operative outcomes
Operative outcomes included the operative time, blood loss volume, number of lymph nodes harvested, normal bladder function recovery time, and postoperative complications. Normal bladder function recovery time was determined based on residual urine <50 ml by ultrasonography. Postoperative complications included urinary system injury, intestinal obstruction, peritonitis, thrombus, perineum and lower extremity edema, symptomatic lymphatic cyst, and delayed incision healing.
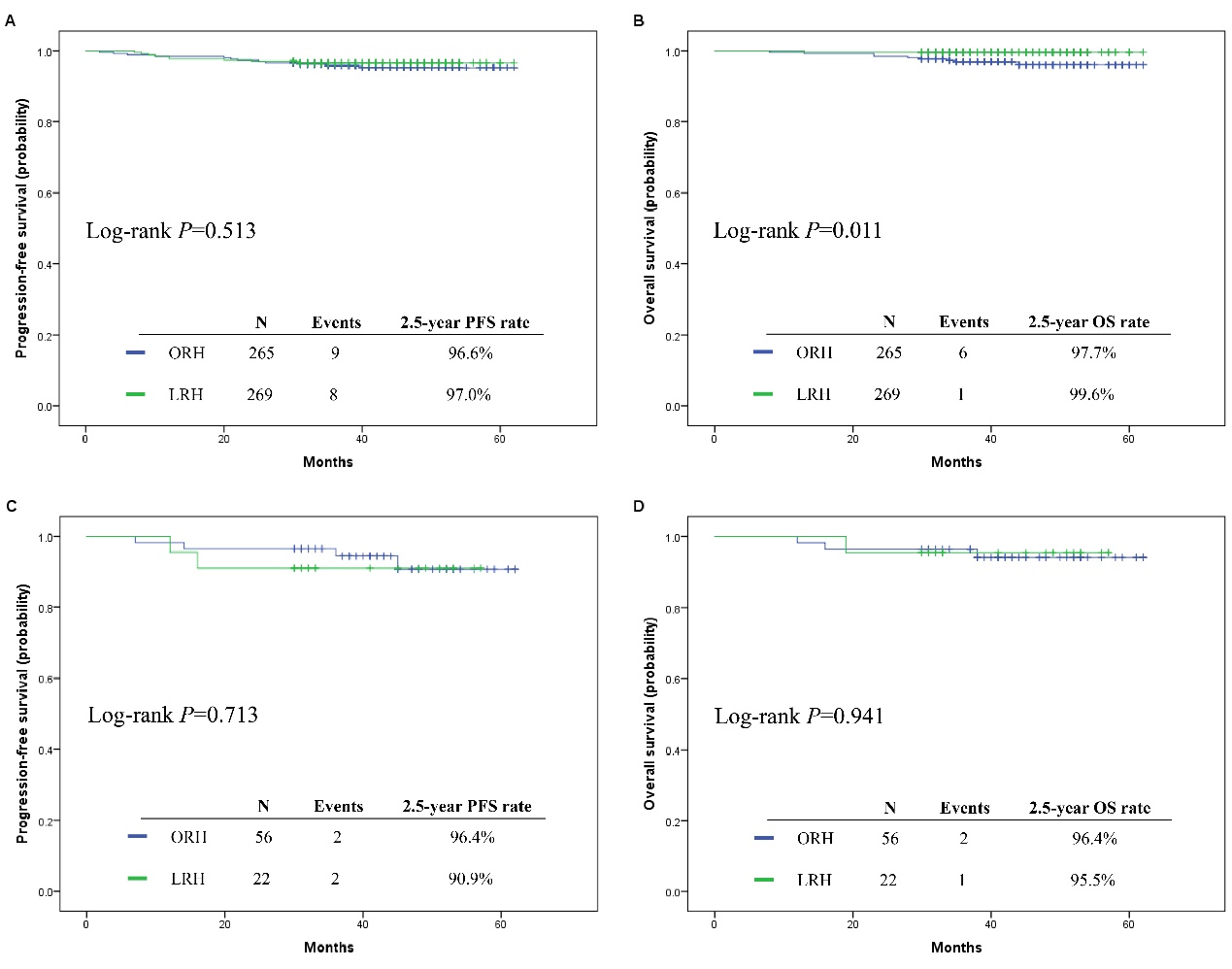
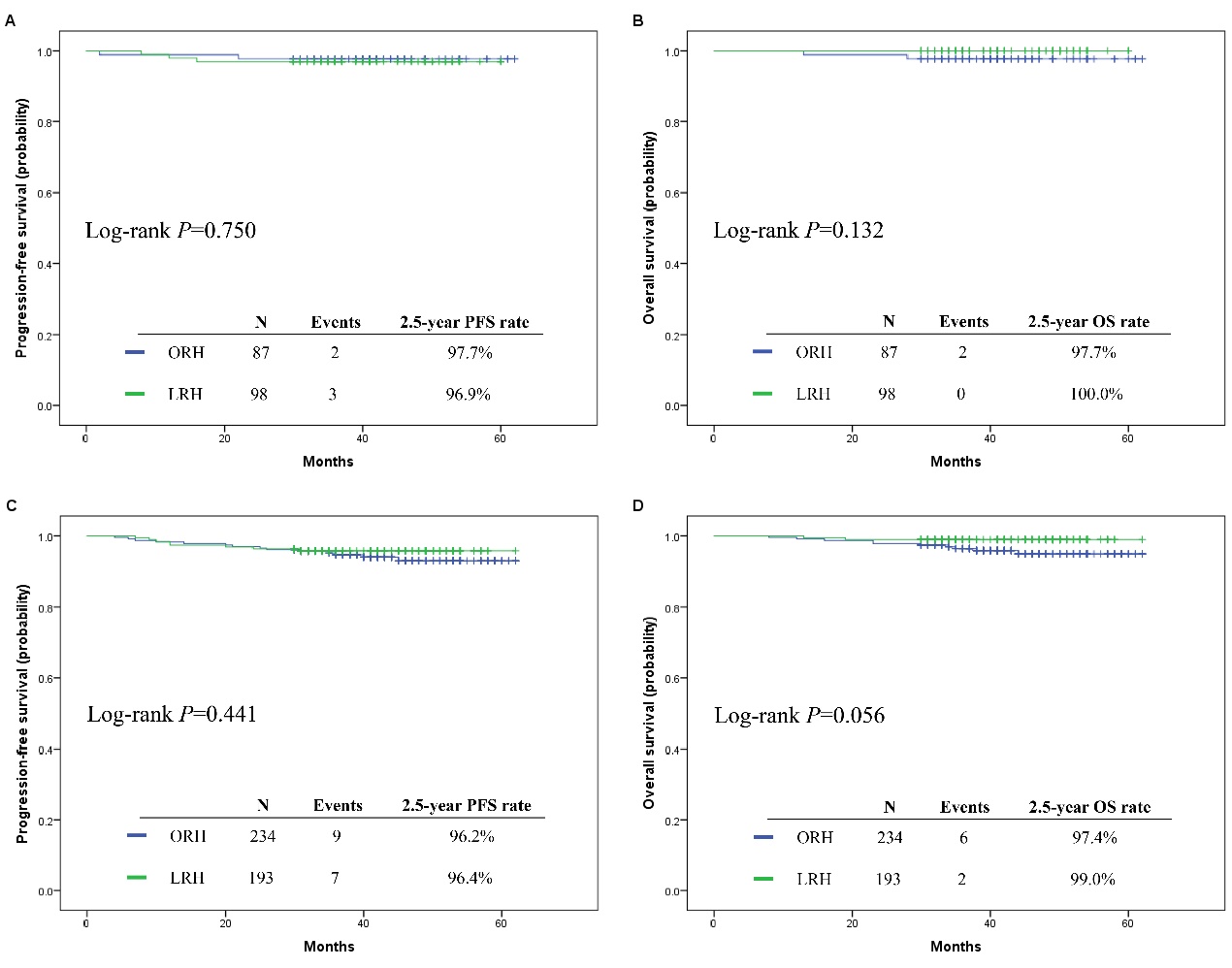
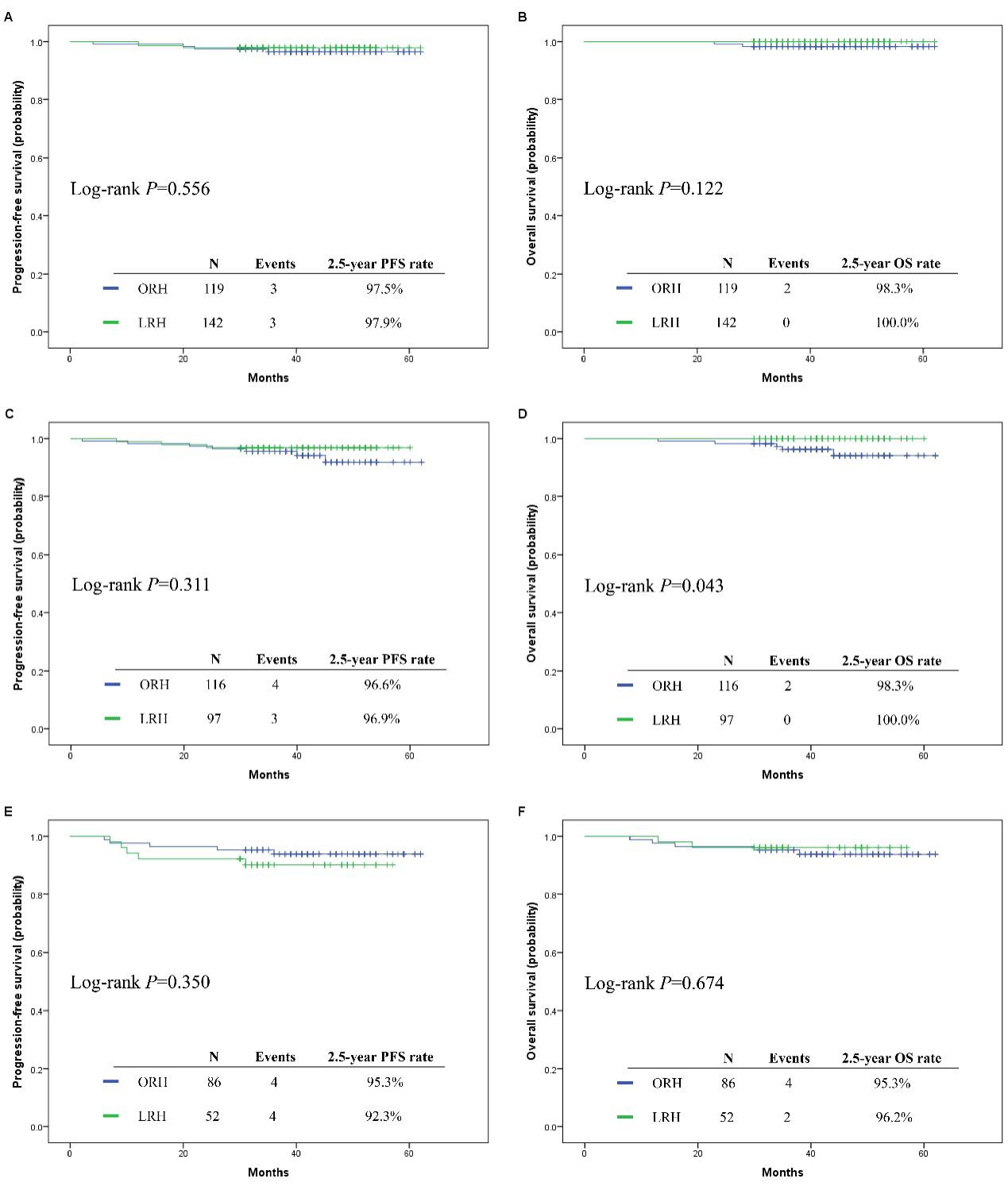
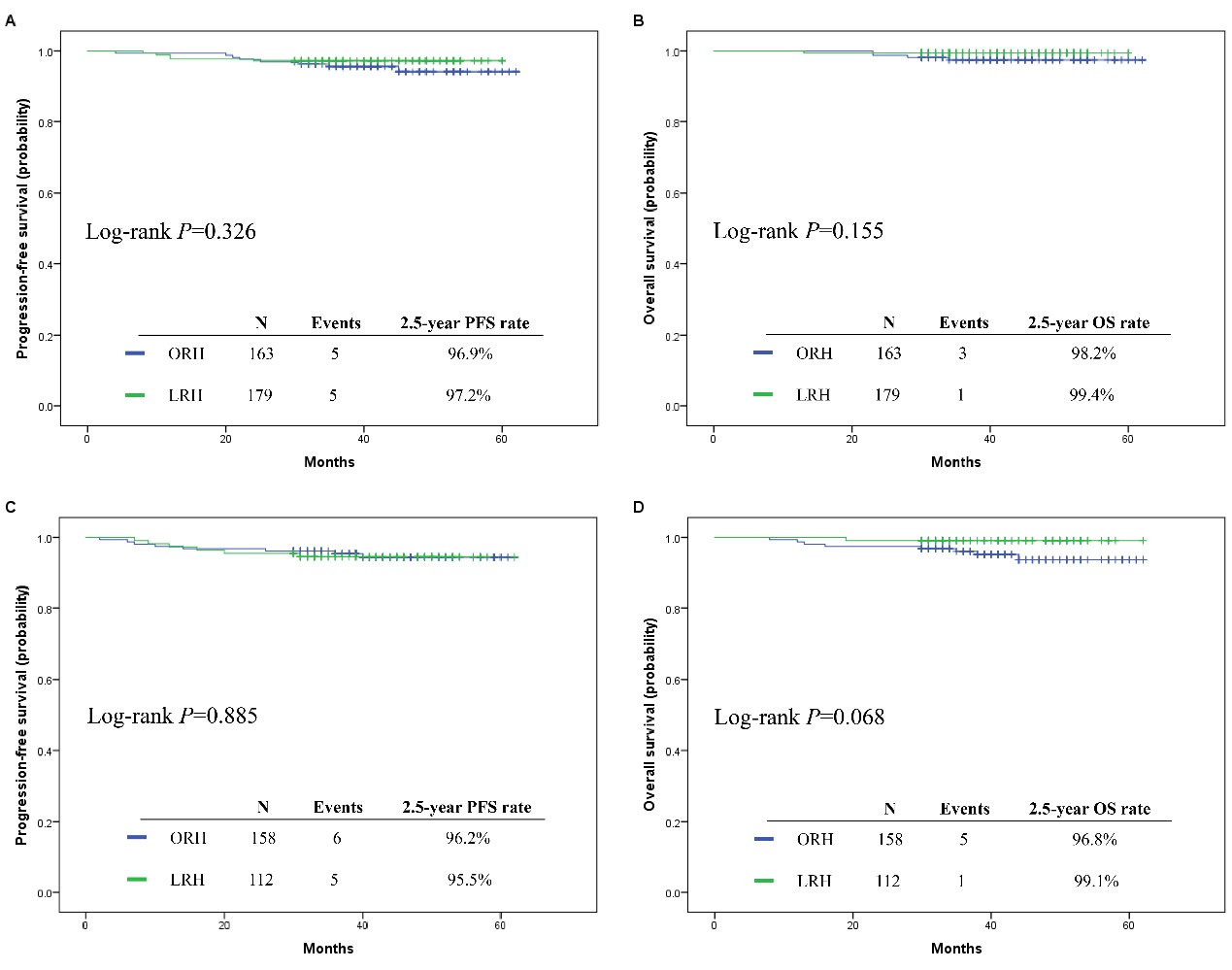
Survival prognosis included the 2.5-year DFS rate, 2.5-year OS rate, recurrence rate, recurrence pattern, DFS time, and OS time. Further analysis was completed by stratification of different factors. DFS time referred to the time between surgery and initial recurrence or death due to cancer. OS time referred to the time between surgery and death due to any cause. Recurrence pattern referred to pelvic local single metastasis or distant multiple metastasis. A Cox regression model was used to analyze the prognostic factors of early stage cervical cancer.
Statistical analysis
For comparisons of continuous variables, the Kruskal-Wallis test was used. For comparisons of categorical variables, the Pearson chi-square test was used. Survival outcomes were compared using Kaplan-Meier analysis with the log-rank test. In both univariate and multivariate analyses, we calculated hazard ratios and 95% confidence intervals using Cox proportional hazards regression models. Statistical analyses were performed using SPSS statistical software (version 25.0). P<0.05 was considered statistically significant.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}