Our meta-analysis included 21 studies with subgroup analysis of oral anticoagulation regimens in patients with TAVR with or without oral anticoagulant indication. Similarly, in patients with TAVR combined with atrial fibrillation who had an indication for oral anticoagulation, there was no significant difference in all-cause mortality and all-cause stroke in the VKA group compared with the NOACss group or in the VKA group compared with the VKA + SAPT group, while the VKA group alone had significantly fewer bleeding events compared with the VKA + SAPT group. We performed a comparison of SAPT with OAC in patients with TAVR without indication for oral anticoagulants, and although the results suggest no significant difference in the effect on outcome events between the two anticoagulation regimens described above, the veracity of the results should be interpreted with caution because of the small number of included studies.
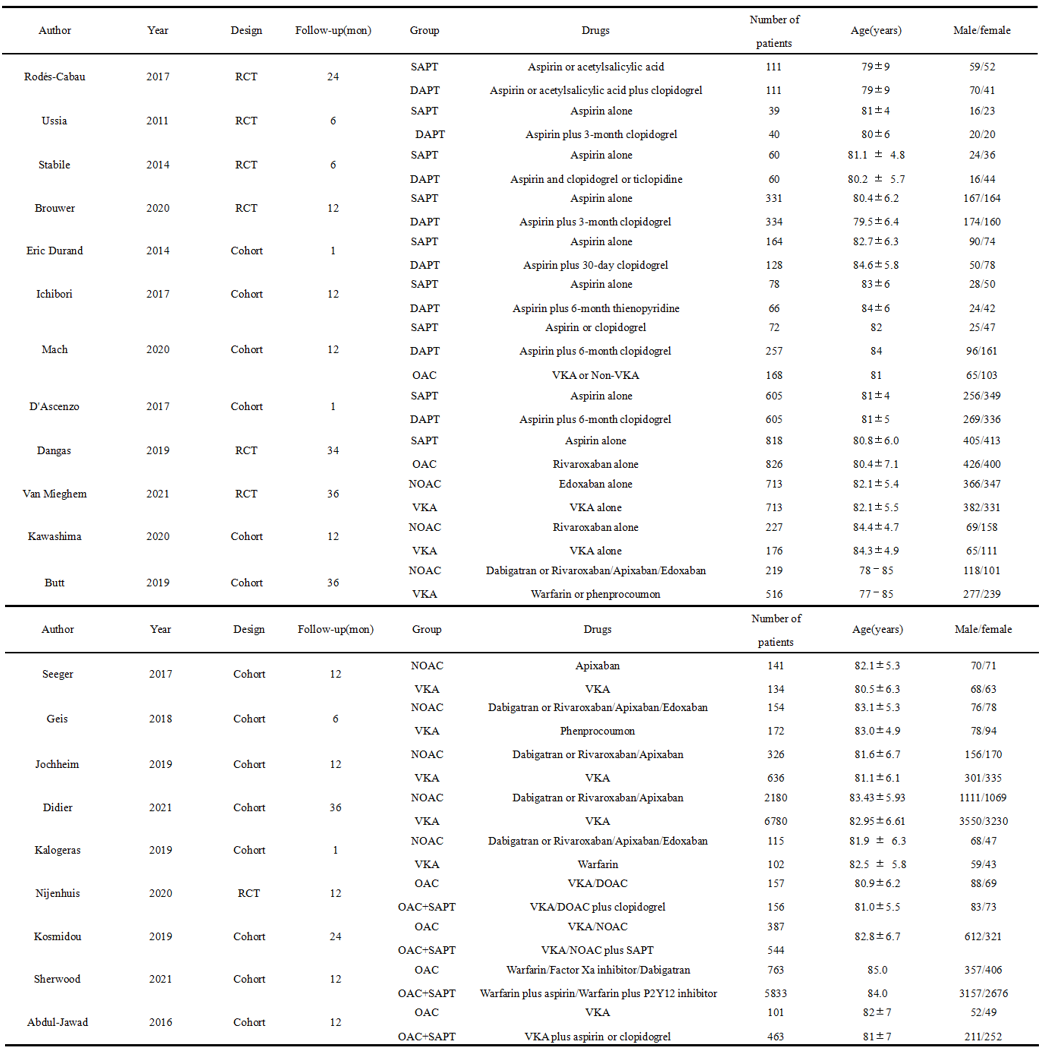
TAVR procedures are increasingly used in patients who are surgical candidates due to their less invasive nature, and therefore at the same time their postoperative related complications are gaining more and more attention. Current clinical outcome indicators for patients after TAVR include all-cause mortality, stroke, and bleeding events. Among them, stroke is the most serious adverse event among post-TAVR patients. Studies have shown that the incidence of severe or disabling strokes within 30 days in patients after TAVR ranges from 0–5% [41–44]. Despite the continuous refinement of the TAVR procedure, its postoperative antithrombotic regimen is still in its infancy compared to its technology itself. Current antithrombotic strategies suggest that intensive antiplatelet therapy before completion of endothelialization of the implanted valve can help reduce the risk of thromboembolism.Several randomized controlled clinical studies have compared different antiplatelet regimens in patients with TAVR without an indication for oral anticoagulants. Ussia et al. [27] used SAPT and DAPT to record major cardiovascular and cerebrovascular events (including death due to any cause, myocardial infarction, severe stroke, emergency or emergency transfer to surgery or life-threatening bleeding) in patients after TAVR surgery at 30 and 6 months, the results found no significant difference in the occurrence of major cardiovascular events between the SAPT and DAPT groups (30 days: 13% vs 15%, p = 0.71, 6 months: 18% vs 15%; p = 0.85), indicating that the strategy of adding clopidogrel to aspirin for 3 months was not superior to aspirin alone. Stabile et al [28] found no difference in 30-day safety endpoints, all-cause mortality, or cardiovascular mortality between the SAPT and DAPT groups, suggesting that patients after TAVR do not have increased morbidity and mortality without DAPT. The ARTE trial, in a study that ultimately included 222 patients, showed that aspirin mono-antiplatelet therapy reduced the risk of major or life-threatening bleeding events compared with dual antiplatelet therapy, but was not associated with an increased risk of myocardial infarction or stroke [26]. In contrast, a study by Brouwer et al [10] showed that in patients with TAVR without an indication for oral anticoagulation, the incidence of bleeding after 1 year on aspirin and the incidence of bleeding or thromboembolic events was significantly lower than after 3 months on aspirin plus clopidogrel.Similarly, the results of several observational studies have shown that aspirin alone does not increase the risk of postoperative valve dysfunction compared with dual antiplatelet, while also reducing the risk of perioperative complications and 30-day all-cause mortality with greater safety benefits [31, 32, 34]. Our results showed that SAPT was able to reduce bleeding events compared to DAPT, but DAPT was not superior to SAPT in terms of all-cause mortality and stroke events. Therefore, to avoid unnecessary overdosing and to reduce the financial burden on patients' families, SAPT therapy is more recommended for patients without oral anticoagulants after TAVR.
There are also studies comparing the use of mono-antiplatelet versus oral anticoagulants in post-TAVR patients without an indication for oral anticoagulants.A study by Dangas et al [29] showed that rivaroxaban treatment was associated with a higher risk of death or thromboembolic complications and bleeding compared to an antiplatelet strategy. The results of Mach et al [33] found that patients treated with OAC had a higher risk of death than those treated with patients treated with SAPT had improved 1-year survival (p = 0.006). The results of our analysis suggest no significant difference in the impact of the two treatment regimens on clinical outcomes, but the implementation of such studies was limited because too few studies were included in our analysis, and the use of anticoagulants in TAVR patients without an indication for oral anticoagulants carries a risk of bleeding and some safety concerns. In conclusion, for safety reasons, there is insufficient evidence for the safety of OAC use in postoperative TAVR patients without indications for oral anticoagulants, and DAPT has not shown an advantage in reducing all-cause mortality, stroke, but rather, it increases the risk of bleeding events compared with SAPT, which may be the antithrombotic option of choice for patients with TAVR alone.
Patients with AF undergoing TAVR have a higher mortality rate than those without AF, and patients requiring anticoagulation have a higher mortality rate after TAVR [36]. In addition, new-onset AF after TAVR is associated with an increased risk of mortality, stroke, and major bleeding [37], so antithrombotics in TAVR combined with AF should be treated with more caution. In the last decade, DOAC has been introduced and proven to be a better option for patients with non-valvular AF [38]. Given the benefits and ease of use, DOAC is being used with increasing frequency in patients with TAVR requiring oral anticoagulant therapy [39]. Although current clinical practice guidelines for the management of AF patients include NOACs, there are no practice guidelines indicating the protocol for the use of NOACs in patients with post-TAVR combined with AF.A large randomized controlled study on anticoagulation regimens in patients with combined atrial fibrillation after TAVR showed comparable outcomes with edoxaban as with warfarin in terms of all-cause mortality, ischemic stroke, and intracranial hemorrhage. However, the incidence of major bleeding was higher in the edoxaban group than in the warfarin group, mainly due to more gastrointestinal bleeding [17]. In several other observational studies, there was no significant difference in the reduction of arterial thromboembolism, bleeding or all-cause mortality with DOACs compared to VKA in AF patients treated with TAVR [12, 19, 20, 22]. In addition, in a large observational study comparing DOACs and VKA for oral anticoagulation in patients with TAVR and pre-existing or incident AF between 2013 and 2018, DOACs were associated with comparable stroke outcomes and a significantly lower risk of bleeding, intracranial hemorrhage, and mortality at 1 year compared with VKA [40]. Similarly, several studies have shown that DOACs may be associated with lower long-term all-cause mortality, bleeding rates, and safety endpoints in patients with combined AF who were successfully discharged from the hospital after TAVR. In contrast, our meta-analysis suggested no significant differences in all-cause mortality, stroke, and bleeding events between VKA and NOACs used to treat patients with TAVR combined with AF. Therefore, the combined results of the above studies provide more support for preferential use of DOACs over VKAs in patients requiring oral anticoagulation therapy after TAVR.
In addition, there is controversy about the benefit of adding antiplatelet agents to OAC therapy after it has been activated in patients with TAVR combined with atrial fibrillation. A randomized controlled study showed that the incidence of severe bleeding at 1 month or 1 year with oral anticoagulation alone was lower than with oral anticoagulation plus clopidogrel in patients with TAVR receiving oral anticoagulation [16]. Several observational studies have shown that the use of OAC + APT does not reduce the risk of stroke, major adverse cardiovascular events, and all-cause mortality compared with OAC alone; instead, it increases the risk of serious or life-threatening bleeding [24, 25]. The results of our meta-analysis are consistent with the above-mentioned studies, and in patients with TAVR combined with AF, OAC alone has a better safety profile without increasing the risk of all-cause mortality and stroke.
Strengths and Limitations
This meta-analysis compared antithrombotic regimens in patients with or without oral anticoagulant indication after TAVR, including currently available randomized controlled clinical studies and observational studies with subgroup analysis of the different study protocols. However, our study has some limitations. We included a large number of observational studies in combination with randomized controlled studies, and all studies inevitably have some heterogeneity that has an impact on the veracity of the final results, and secondly, our study did not adjust for baseline characteristics, comorbidities, age, and other confounding factors in the original study.
{kind=link}