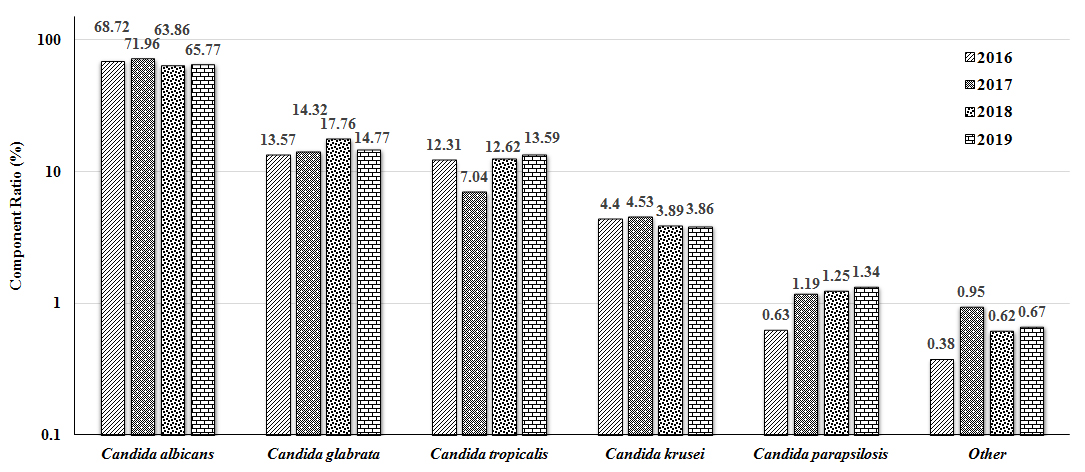
C. tropicalis is a common opportunistic pathogenic fungus, and its rates of detection have been increasing over the past years. In this study, a total of 2872 strains of Candida were detected in samples collected from 2016 to 2019, of which C. albicans accounted for approximately 70.00%, while C. tropicalis ranked third, accounting for 12.00%. Moreover, the overall species composition of Candida showed statistically significant differences between the detection years. Susceptibility to antifungal agents of C. tropicalis in our hospital showed that the resistance rate of C. tropicalis to azole antifungal drugs sharply increased. In this study, based on the increasing isolation rate and drug resistance rate of C. tropicalis, the distribution and drug susceptibility of C. tropicalis were analyzed, as well as the relationship between ERG11/UPC2 gene expression and resistance to azole antifungal drugs.
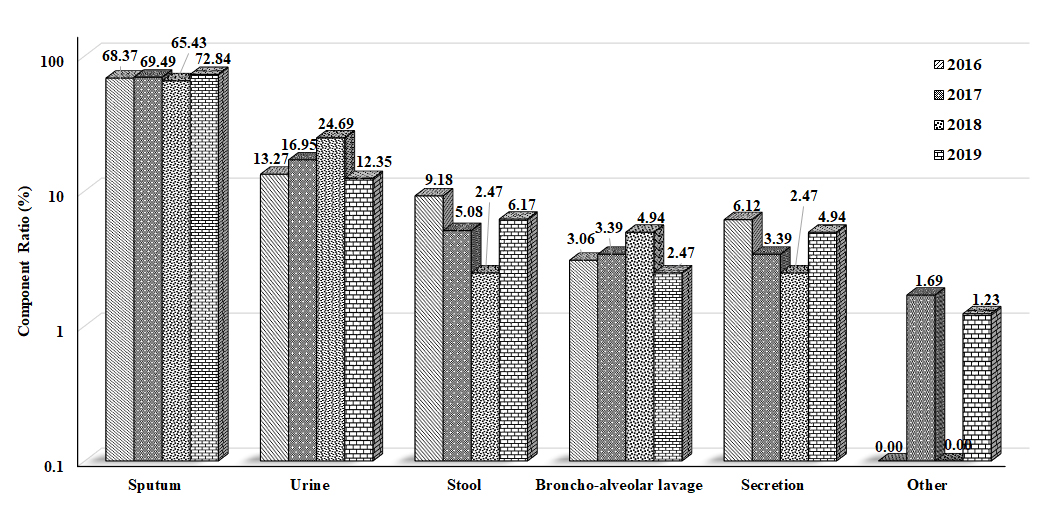
Our results showed that there was no significant difference in the overall species composition from C. tropicalis samples tested over these four years. Moreover, the main source of C. tropicalis was airway secretion, which might be related to that the C. tropicalis is one of the upper respiratory tract-colonized fungi and can be easily isolated; further, C. tropicalis has been shown to form biofilms on invasive catheters (such as tracheal tubes)[16]. Therefore, C. tropicalis with reproductive growth is often detected in airway secretions. In view of interference factors such as Candida colonization, a culture of sterile tissue or fluid should be recommended in the diagnosis of bronchopulmonary candidiasis. And then the final diagnosis should be made based on clinical manifestations and other fungal-related test results of the patients. In addition, C. tropicalis was detected in the mid-stream urine samples, with a detection rate of 13.00%-25.00%, which had increased over the years. This phenomenon might be related to the increasing number of patients treated with invasive urinary tract operations and/or the increase in the number of mid-stream urine samples sent for examination. C. tropicalis has strong adhesion, penetration and destructive abilities in relation to mucous membranes, and its resistance rate to azole antifungal drugs is higher than that of C. albicans[17]. However, it is difficult to distinguish contamination, colonization or infection from urine culture. In the diagnosis of urogenital tract infection, clinicians should consider the patient's clinical manifestations, white blood cells/hyphae in the urine and the result of puncture culture.
In this study, our results showed that there were no significant differences in the resistance rate of C. tropicalis to azole antifungals between these four years, but the resistance rate had been increasing year by year (with the rate of resistance to fluconazole being as high as 39.51%[32/81]). The increased resistance rate of C. tropicalis to azole antifungal drugs might be related to the easy application of such drugs and the relatively mild adverse reactions[18]. In the clinic, a large number of patients with high-risk factors for invasive candidiasis were subjected to prophylaxis therapy or empirical therapy by using azole drugs to prevent the infection of Candida[19], however, long-term application of these drugs could easily lead to the emergence of azoles-resistant strains[20-21].. Therefore, in order to slow the increase of azole-resistant C. tropicalis, the cooperation of multidisciplinary teams in hospital can make clear the diagnosis of disease, improve treatment and control antibiotic use. In addition, the diagnosis of candidiasis should be according to the high-risk factors, manifestations, etiological tests, diagnosis guidelines, etc.; the treatment of candidiasis should refer to the laboratory antifungal susceptibility test, antigen test, epidemiological characteristic, etc.; only in this way can we reasonably use azoles and avoid the prevalence of azoles-resistant Candida[22-24].
Moreover, in this study, the ERG11 and UPC2 genes of 50 strains of C. tropicalis were assessed, and our results showed that the relative expression level of the ERG11 gene in the drug-resistant group was higher than it was in the susceptible group, which is in line with the findings from Jiang et al.[25] regarding the high expression of ERG11 in fluconazole-resistant C. tropicalis. ERG11 overexpression could increase the amount of 14-DM in cells, which ensures ergosterol synthesis and the normal growth and reproduction of Candida, therefore leading to azole drug resistance[26-27]. Moreover, Jiang et al.[25] cloned Y132F and S154F ERG11 mutants from C. tropicalis and introduced them into Saccharomyces cerevisiae (S. cerevisiae) and showed that the sensitivity of S. cerevisiae to azole antifungal drugs, especially fluconazole, was decreased. These results suggest that Y132F and S154F are involved in the resistance of C. tropicalis to fluconazole. Moreover, our results showed that the expression level of UPC2 in the resistant group was also higher than that of the susceptible group, indicating that the overexpression of UPC2 may cause C. tropicalis to become resistant to azole antifungal drugs, which was consistent with the findings from Jiang et al.[28]. In this study, the correlation analysis of the ERG11 and UPC2 mRNA expression levels in C. tropicalis showed that there was a linear positive correlation between the genes in the drug-resistant group. These results indicated that when UPC2 was over-expressed in the fluconazole-resistant C. tropicalis, ERG11 would also be over-expressed. Therefore, the expression level of ERG11 might increase with the over-expression of UPC2. It has been shown that UPC2 has transcriptional regulation in C. albicans[13] and the over-expression of UPC2 in the fluconazole-resistant C. albicans can induce the over-expression of ERG11[29-30]. Therefore, our results suggest that the over-expression of UPC2 in the fluconazole-resistant C. tropicalis may effectively promote the over-expression of ERG11, and then increase the ergosterol synthase in cell membrane and cause the resistance to azole antifungal drugs in C. tropicalis, especially fluconazole. However, Choi et al.[31] sequenced the UPC2 gene in C. tropicalis, and their results showed that the amino acid substitutions caused by mutations in the gene appeared not only in the resistance group overexpressing ERG11, but also in the susceptible group with no ERG11 overexpression. So far, no effective missense mutation has been detected in the UPC2 of fluconazole-resistant C. tropicalis, and therefore the reason for the over-expression of UPC2 needs further study. If the expression of ERG11 and UPC2 genes can be routinely detected in clinic, the resistance of C. tropicalis to azole antifungal drugs can be evaluated according to the gene expression levels, which might provide more valuable guidance to the treatment of C. tropicalis infection. Drug resistance might also be related to multiple factors, and in a few drug-resistant C. tropicalis without ERG11 and UPC2 overexpression, the mechanisms underlying drug resistance might be related to efflux pumps[32] and biofilm formation[33]. To fully understand the drug resistance mechanisms of C. tropicalis, it is necessary to comprehensively study the impacts of the mechanism on drug sensitivity. Based on these findings, further in-depth studies are still needed to investigate the transcriptional regulatory function of Upc2p in drug-resistant C. tropicalis and to explore how UPC2 overexpression regulates ERG11, thus leading to drug resistance to azole antifungal drugs.
{kind=link}
{kind=link}
{kind=link}