LDN is an indispensable part of many urological tumors, such as bladder cancer, prostate cancer and urothelial cancer. The role of LND in patients with renal cell carcinoma has been controversial in recent years. Patients with RCC and TT represents a unique population of patients, which were classified as T3 according to the TNM classification9. As we all know that according to the EUA guideline7, all patients with non-metastatic renal cell carcinoma and tumor thrombosis should be considered for surgery if patient status acceptable. However, LND could spend a long time especially in the patients with RCC and TT, but the benefits were unclear. Our research provides an opportunity to learn more about the role of LND on such unique patients.
From the baseline of our cohort we found between LND and no LND group, the clinic characteristics were relatively similar except the proportion of cN+. LND was more likely underwent in patients with cN + disease than in those with cN0. It reflects that the surgeon’s preference of LND using in the population with potential lymph node metastasis, which was consistent with published guideline. The operation time (357 min vs 307 min; p = 0.002) and hospital stay (12.6d vs 9.5d; p = 0.094) are much longer in the LND group, which means the LND can increased the difficulty of surgery and add the hospitalization expense. The complications were not increased in LND group, which were consistent with EORTC 30881 study that increased LND were not associated with more complications1. Besides, the recent ASSURE trial showed there were no differences in preoperative complications between the LND and no LND groups in non-metastatic RCC of high risk group11. Combined with our study, it appears that the safety of LND, even in the operation of patients with RCC and TT, may be acceptable.
Although EORTC 30881 did not show any improvement in progression-free survival in patients receiving LND, most patients in the study were classified as the localized or low grade RCC1. In the high- risk group, the survival benefit of LND were on the debate. Some retrospective analyses suggested that patients with high risk factors may benefit from LND2–6. Blute et al.2 and Crispen et al.5 found that patients with large tumor size (> 10 cm), high furhman grade, pT3-pT4, coagulative necrosis and sarcomatoid differentiation may benefit from LND. Capitanio et al.3,4,6showed LND in the high-risk population like bulky tumor (> 10 cm), locally advanced or metastatic RCC could improve CSS. However, Feuerstein et al.12 and Gershman et al.13 observed that LND did not improve either CSM or OS across all stages, as well as in patients with increased risk of LN metastasis.
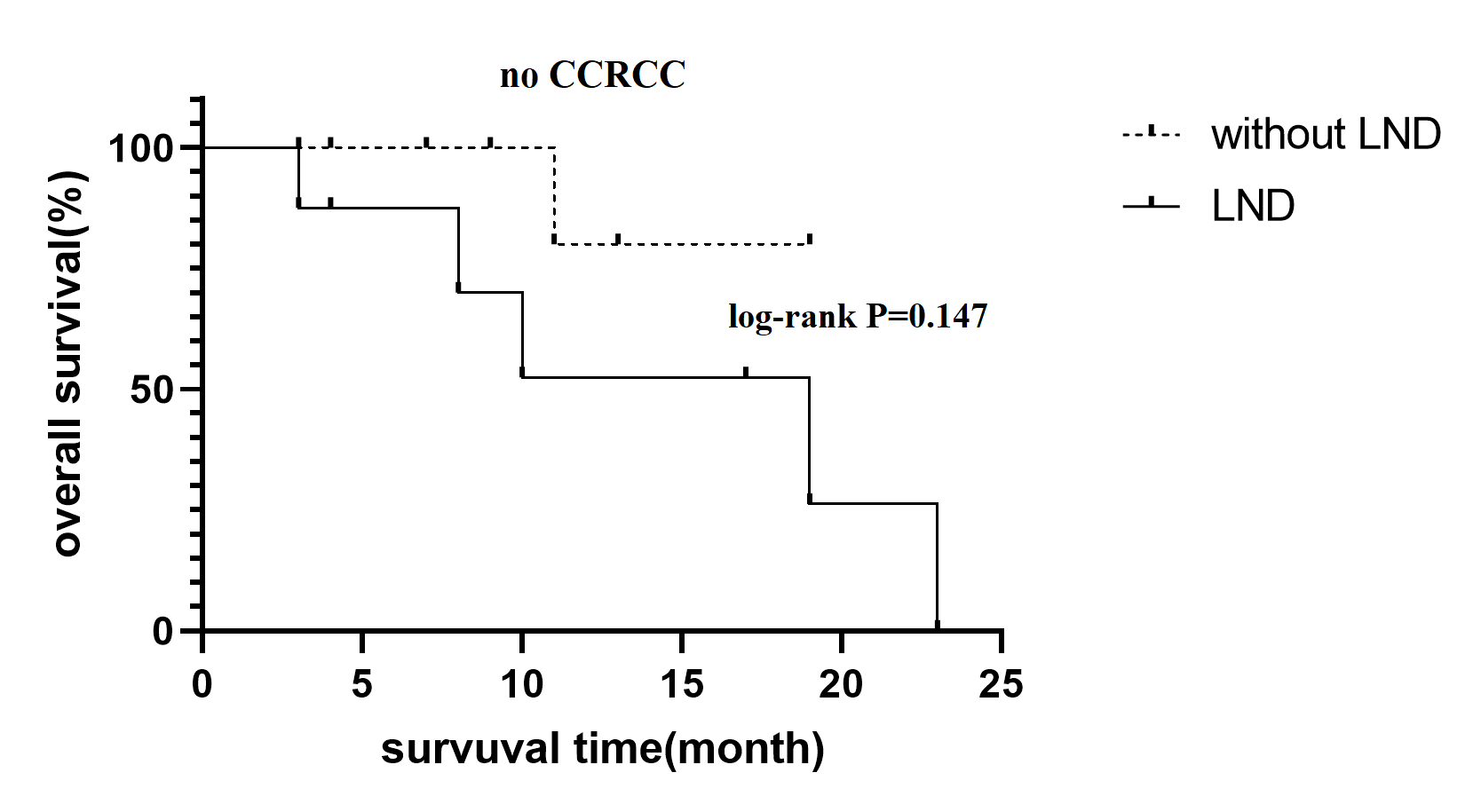
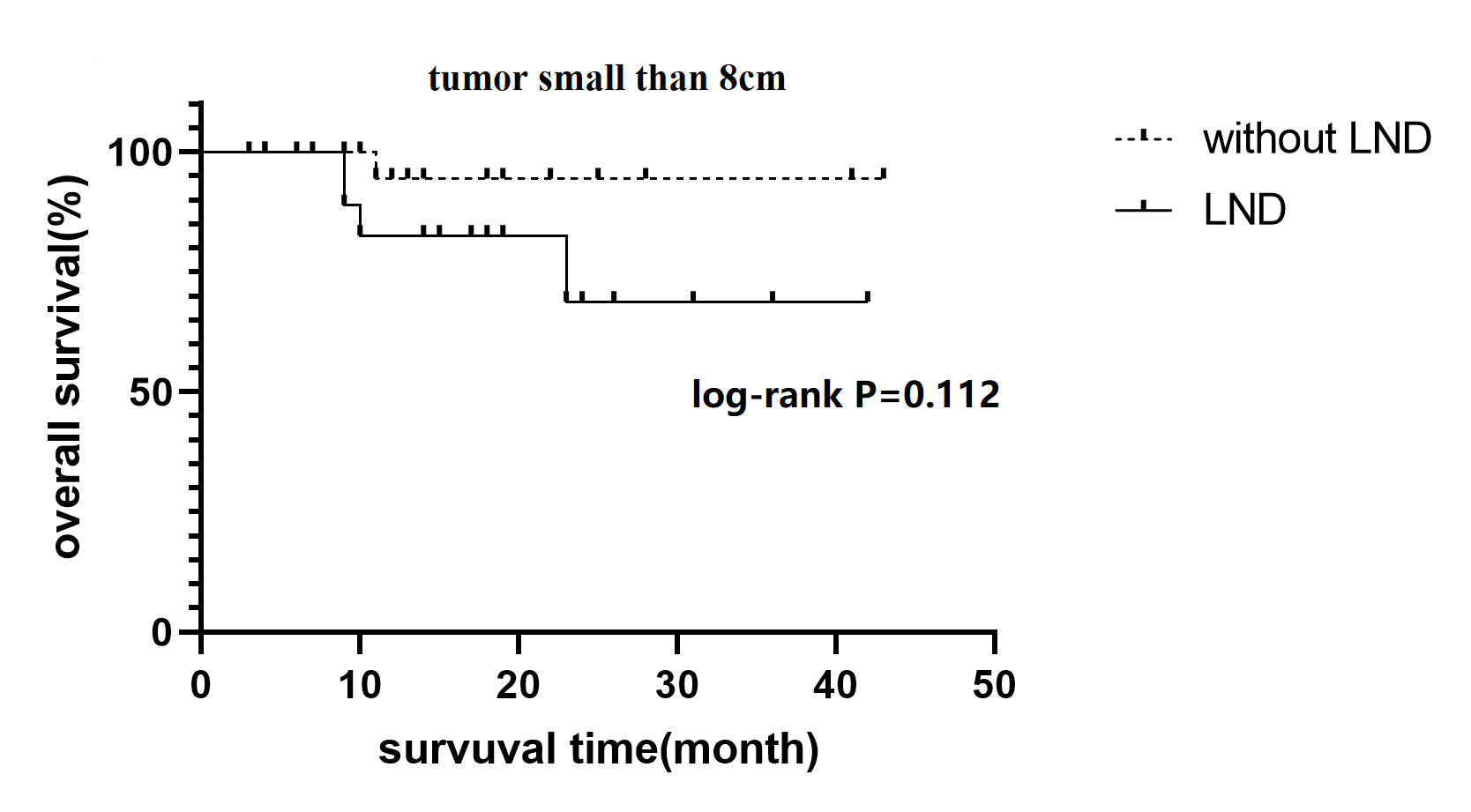
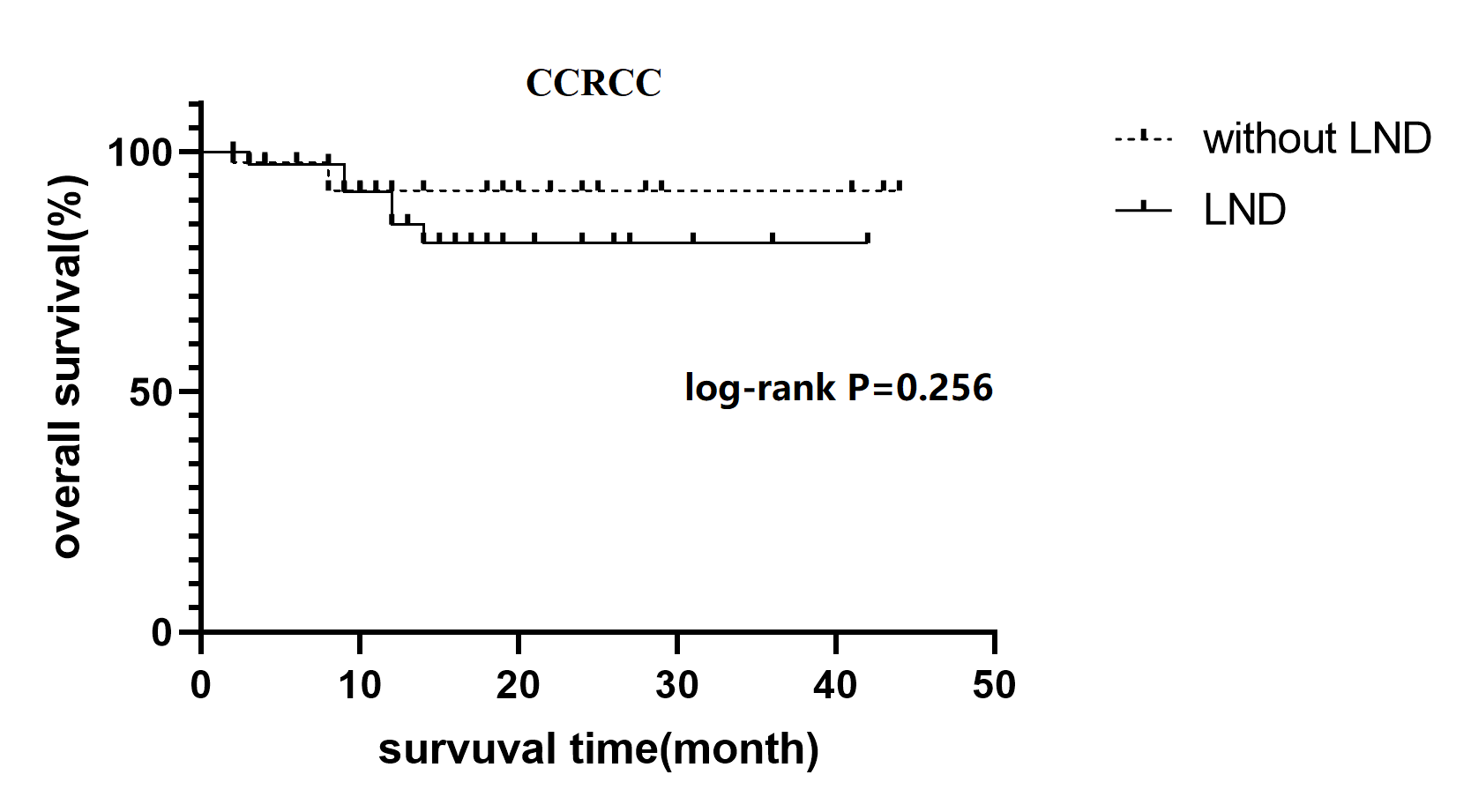
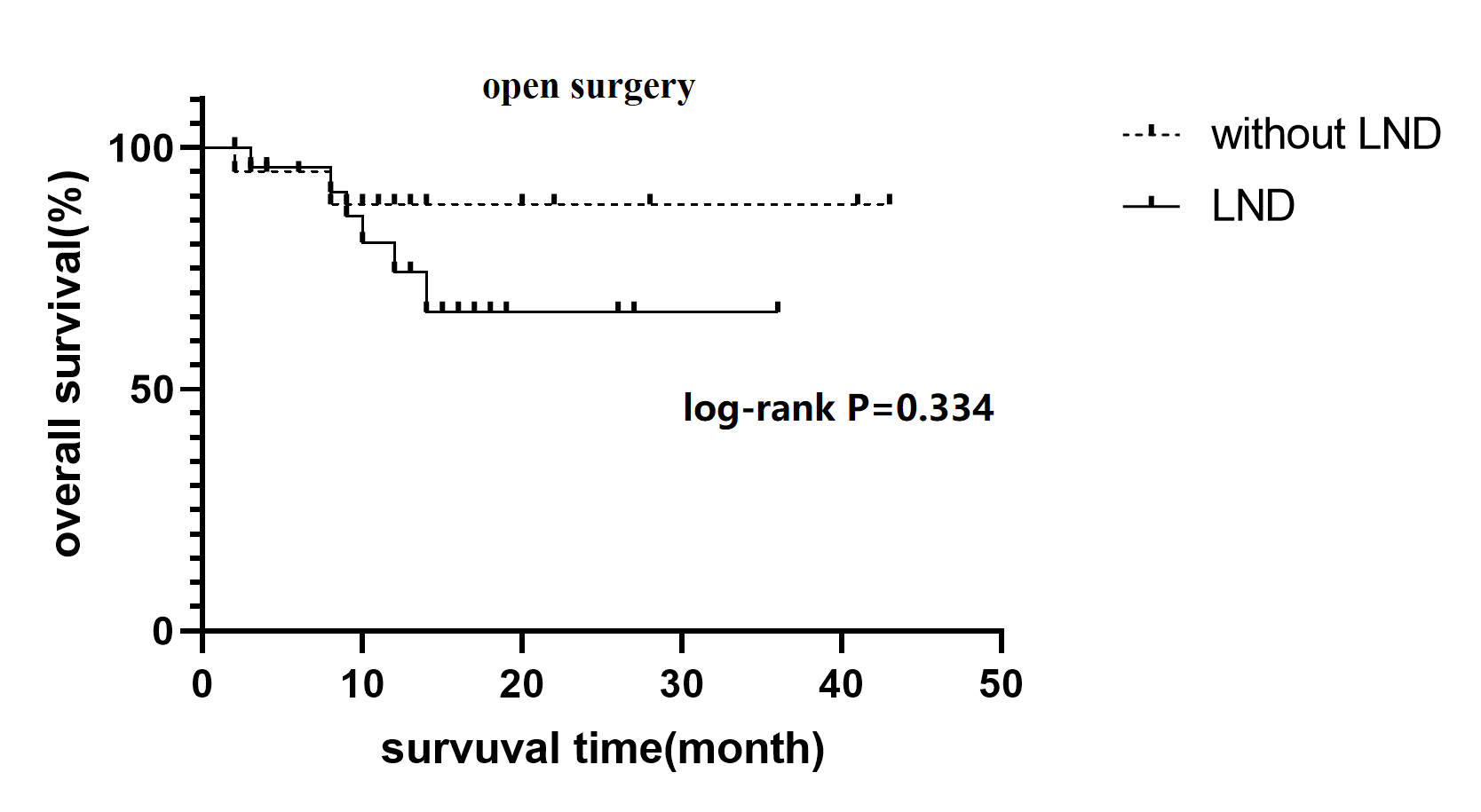
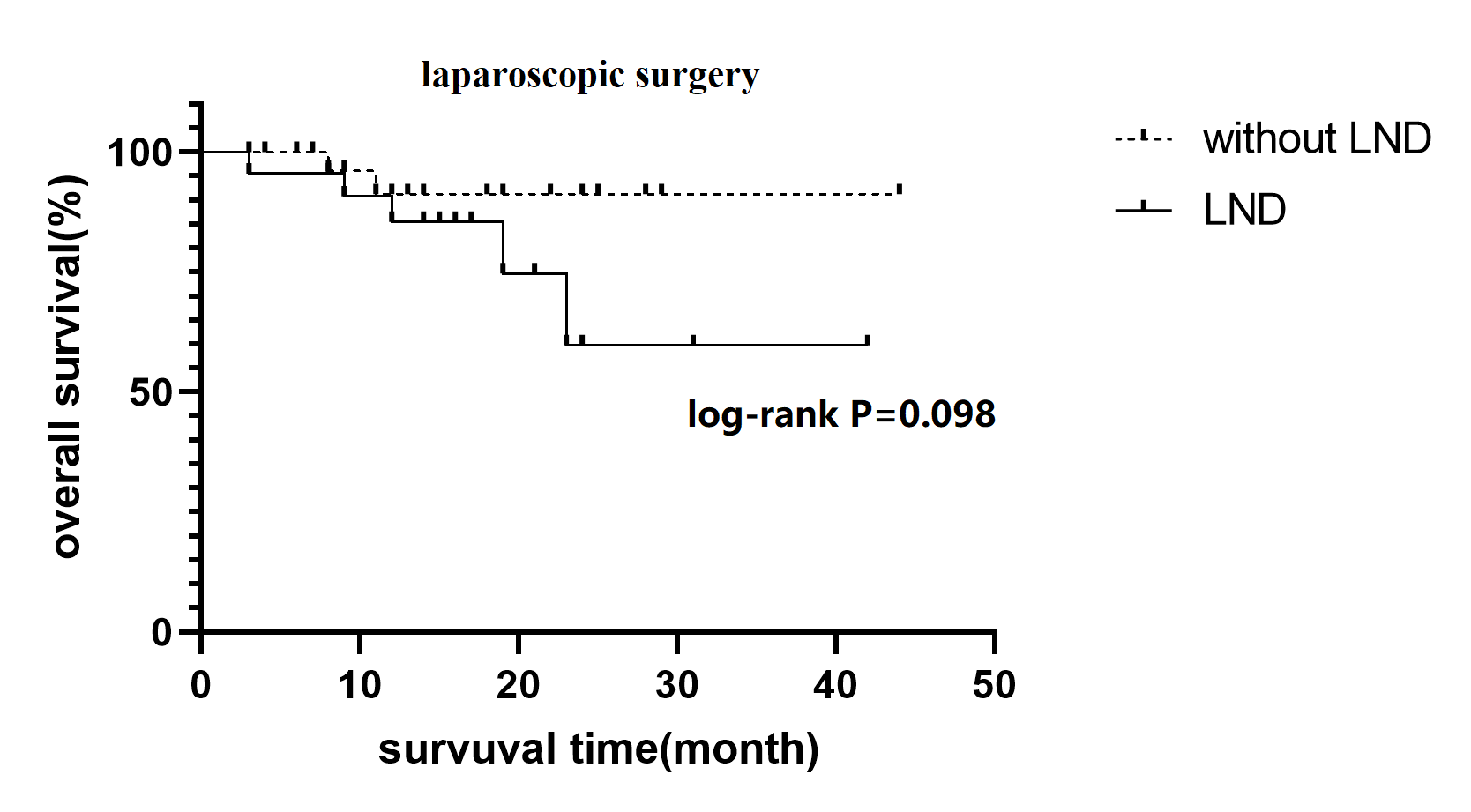
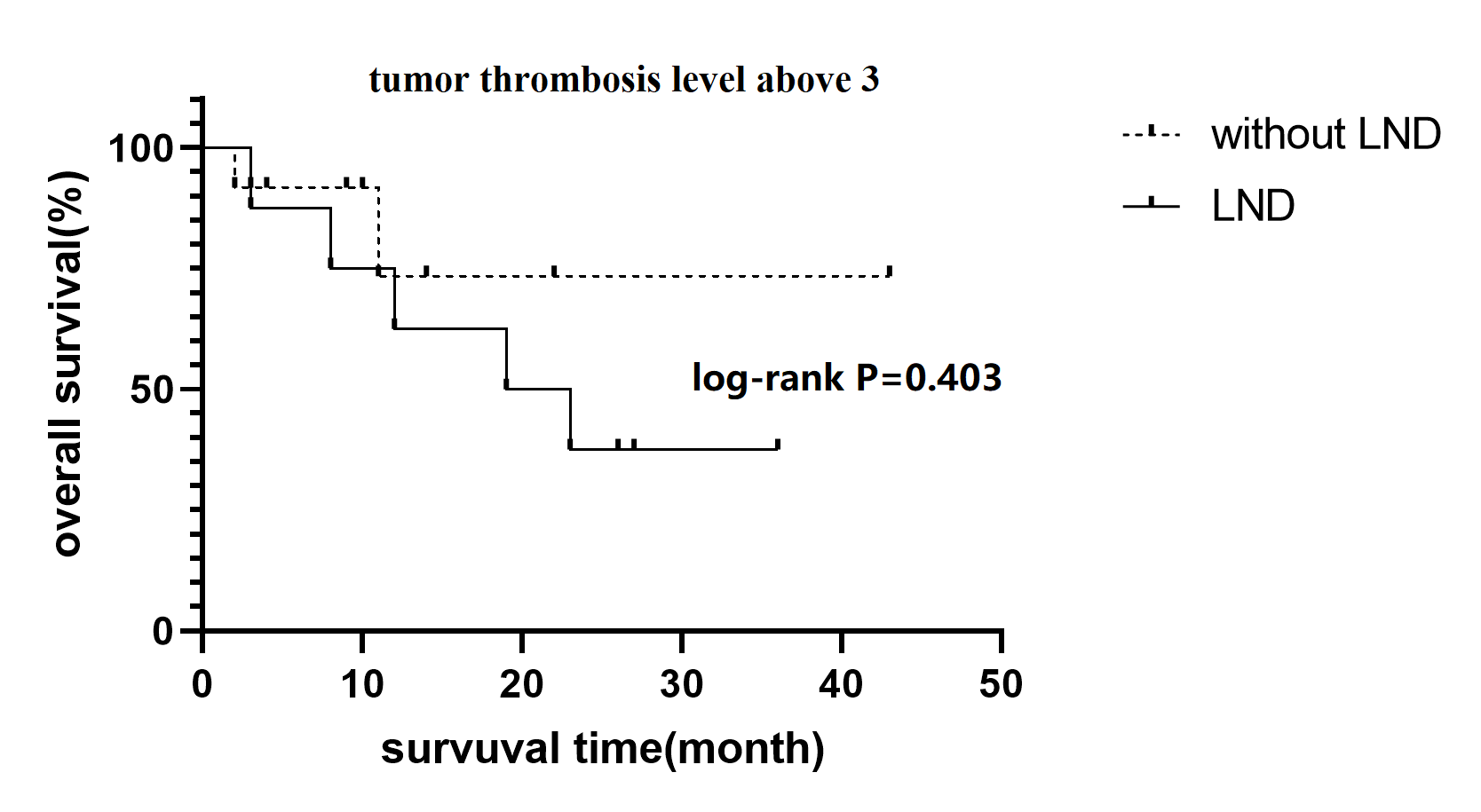
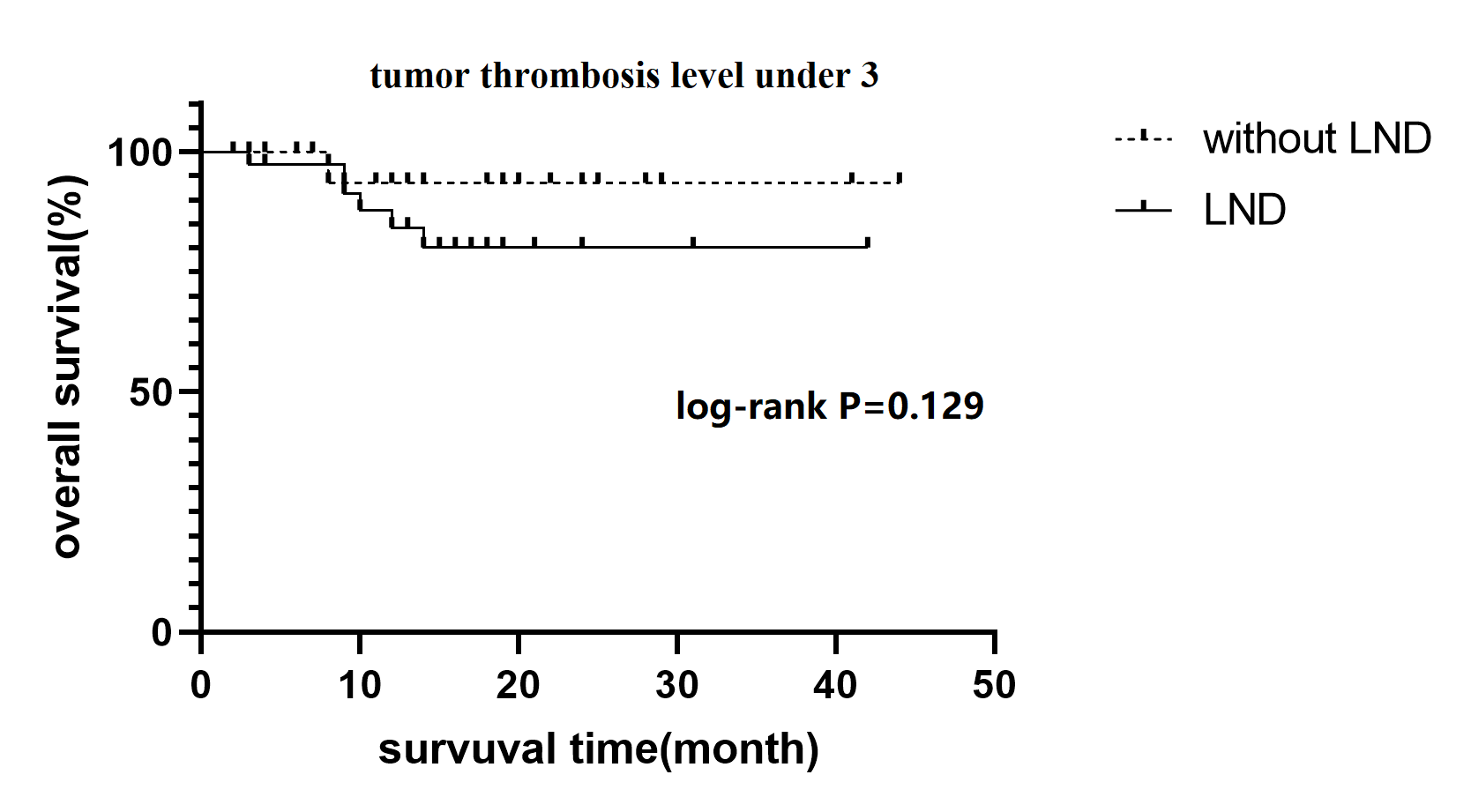
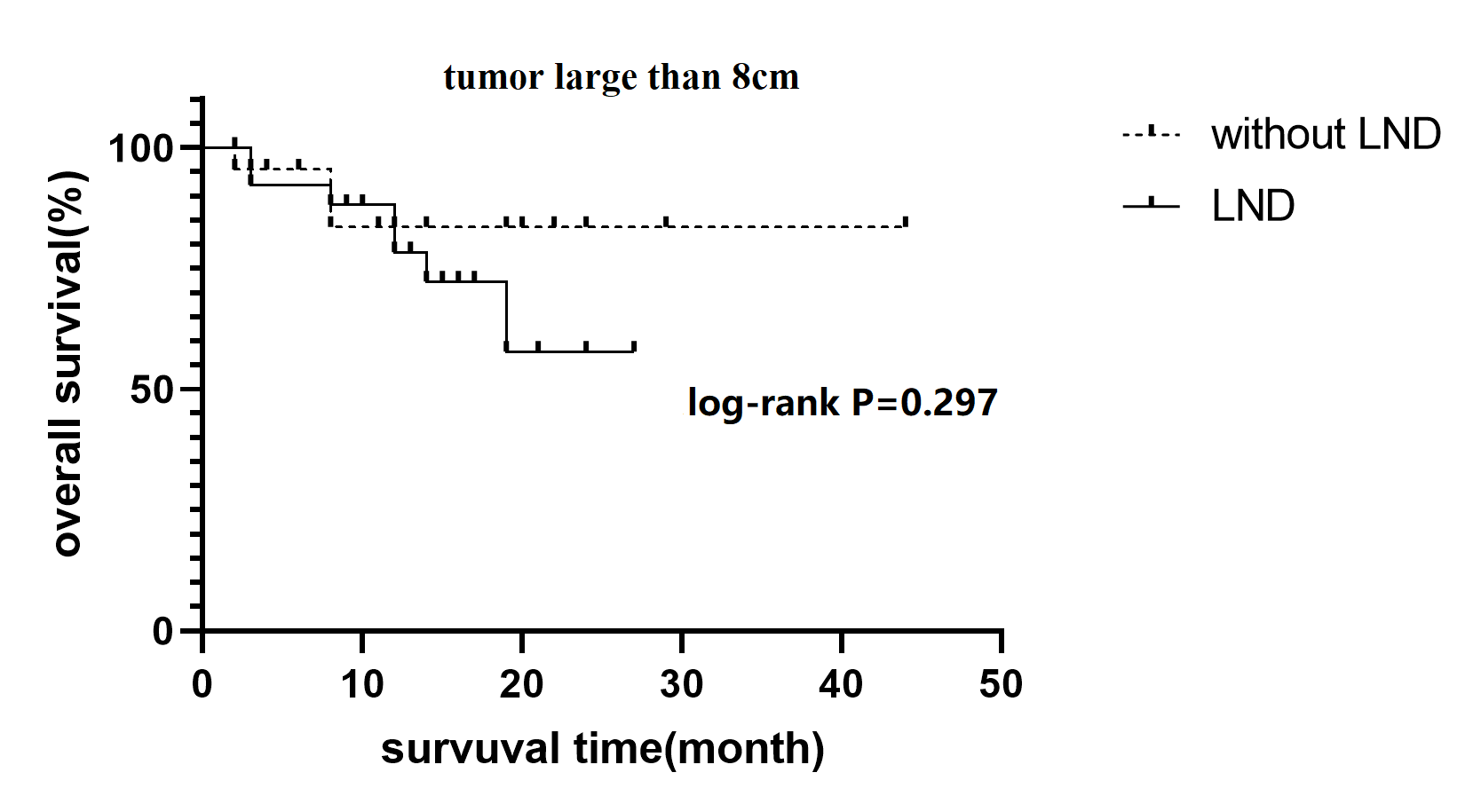
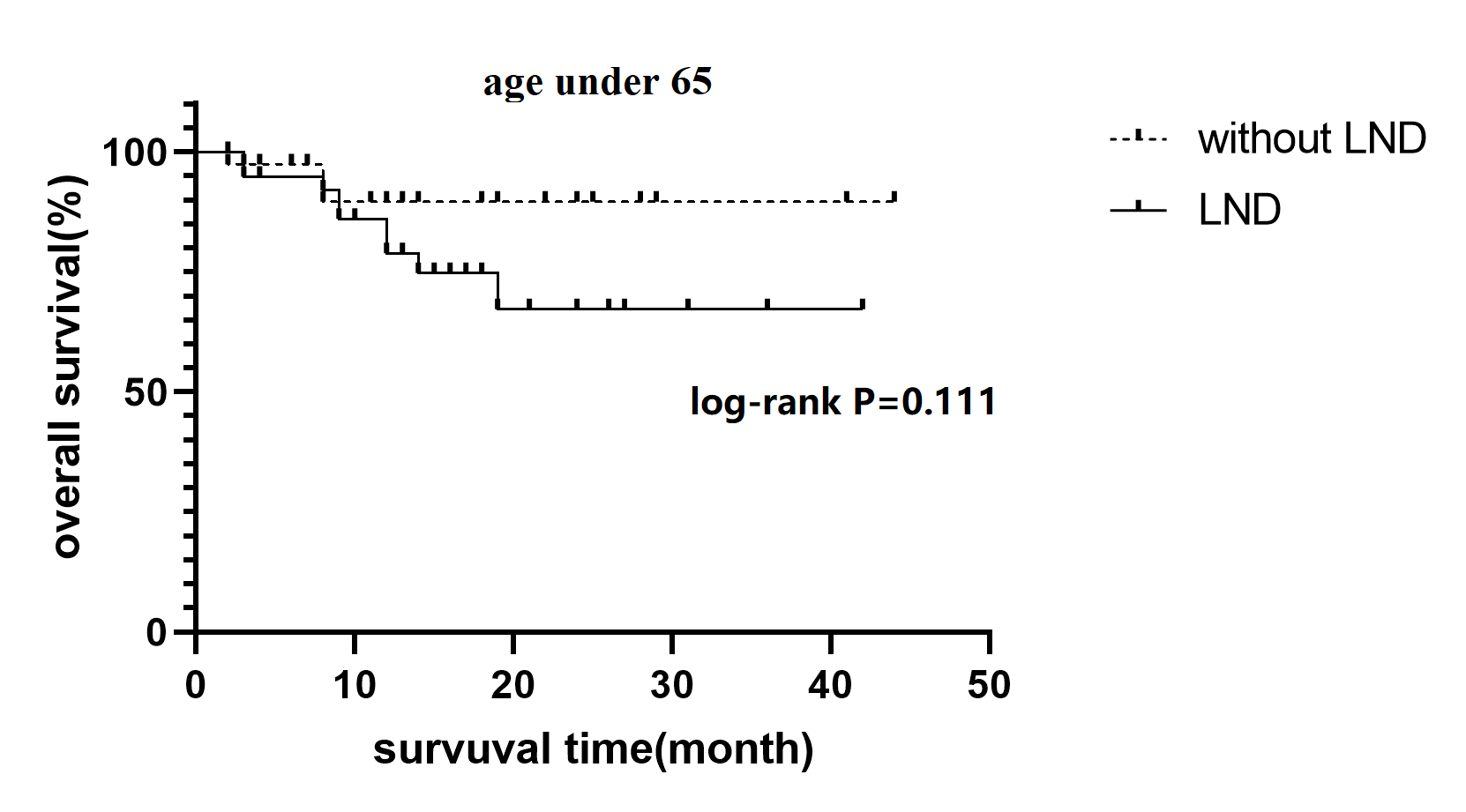
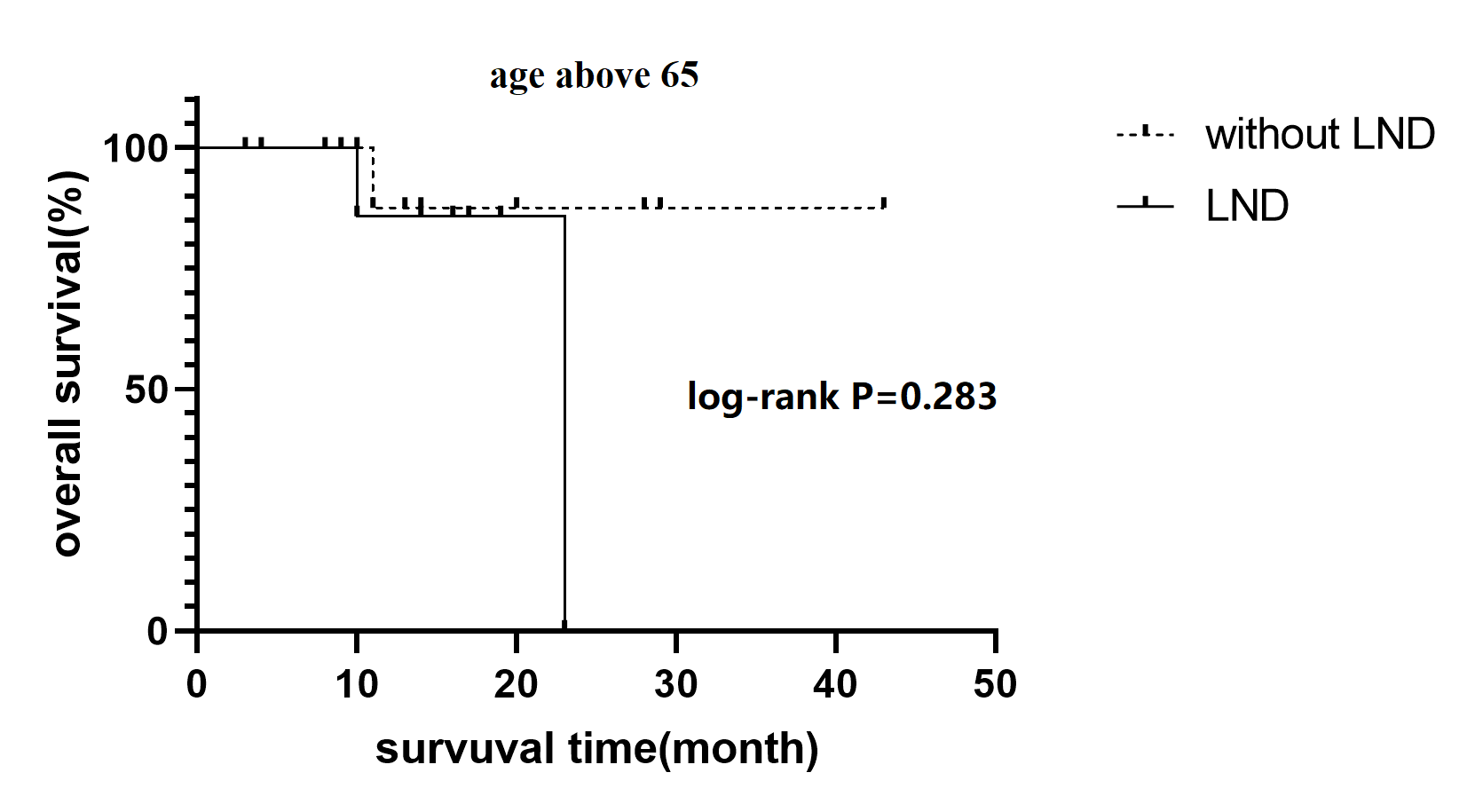
Patients with RCC and TT may represent a special type of high risk feature, but our Kaplan-Meier curve shows that LND had worse OS compared to no LND groups. We suspected the result may attribute to the high proportion of cN1 in LND group, which may potential affect OS. So we analyzed OS in subgroup of cN0 and cN1 but failed to find any survival benefit of LND either for cN0 or cN1. After that, We analyze the OS adjusting for some risk factors like age, tumor size, surgical approach, tumor thrombosis level and histologic type, trying to find the certain part of population whom can potential benefit from LND but failed. Some of the existing studies are similar to our results. Michele Marchioni et al.14 carried out a research in SEER database and found that LND have an adverse protective effect on CSM either in the pT2 or pT3 patients. In the pT3 patients, the 5-year CSM-free survival were worse in LND compared with no LND group (65.1% vs 80.9%, P < 0.001). Michael A. Feuerstein et al.15 reviewed data on 258 patients who underwent LND during cytoreductive nephrectomy and found LND had worse OS compared those who did not received LND. Benjamin T. Ristau et al.11 analyzed the high-risk patients without metastasis in the ASSURE trial and showed LND was associated with worse DFS (HR 1.27, p = 0.001). Besides, LND were not associated with OS after in subgroup analysis of treatment arm, grade, stage, gender, age, performance status, symptoms at diagnosis, lactate dehydrogenase level, anemia, histology and surgery type (HR 1.14, p = 0.20). Some of researchers were attribute to the selective bias that patients with high-risk features are more likely to choose LND. Others suspected because lymph node metastasis is rare in renal cell carcinoma, LND can be regard as unnecessary aggressive surgical resection. Patients who underwent unnecessary aggressive surgical resection could increase potential morbidity. Similar findings were also found in other malignancies16. Thus due to the controversial result of current study, we need a high-quality randomize trial to further demonstrated the survival benefit of LND in high risk population.
Finally, to identify prognostic factors of RCC with TT whom underwent LND, we examined the associations of some clinicopathologic features. Non-CCRCC and occurrence of major complication were the predictors of worse OS while positive lymph nodes was the only independent prognostic factor presenting worse OS. Derya Tilki et al.17 reviewed 1978 patients with RCC and TT and found the number of positive nodes harvested during LND and LN density was strong prognostic indicators of CSS. The similar results were showed by Juan Chipollini et al.18. They conducted a research on patients with metastatic RCC treated by cytoreductive nephrectomy and LND, and found the number of nodes positive was predictive of survival. Boris Gershman et al.13 followed up 138 patients with isolated pN1M0 RCC underwent partial or radical nephrectomy and LND at the median of 8.5 year. The 5-yr and 10-yr MFS, CSS, and OS rates were 16% and 15%, 26% and 21%, and 25% and 15%, respectively. So patients with lymph node positive may potentially benefit from LND. However, owing to rarity of lymph node metastasis in RCC even in cN1 patients, it is essential for us to develop a tool that can distinguish the lymph node metastasis before surgery.
This retrospective study has several limitations. Firstly, our research is single-institutional retrospective review, which Inevitably include missing data and confounding variable and selection bias that we could not control. Secondly, LND template was not standardized and was based on surgeon discretion, which might inherently influence the study results. Thirdly, because of short follow-up time and high loss of follow up rate, we can only estimate three-year overall survival in these population. Despite these limitations, our study is significant because we are the only single-institution study to assess the role of LND among patients with RCC and TT.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}