This retrospective case series comprised 27 eyes of 27 patients, with uncontrolled open-angle glaucoma (POAG) and cataract, having combined phacoemulsification, ab-interno trabeculectomy with Kahook Dual Blade (KDB) (New World Medical Inc., Rancho Cucamonga, CA, USA) and ECP, at Instituto de ojos Oftalmosalud, Lima, Peru, between April 2017 and May 2017. The ab-interno trabeculectomy was performed 90-120 degrees, and endoscopic cyclophotocoagulation was performed 360 degrees through 2 site corneal incisions. The mean duration of the follow-up period was 9 months.
The ethics committee of the Institutional Review Board of Instituto de Ojos Oftalmosalud in accordance with Declaration of Helsinki approved this retrospective study. All patients in the study were informed of the procedures and legal consent was obtained.
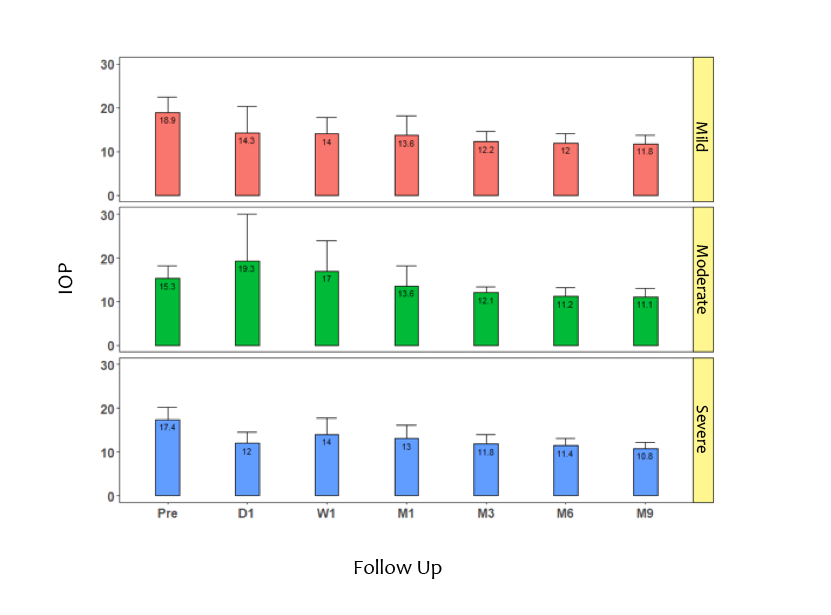
Inclusion Criteria: Glaucoma patients with uncontrolled POAG from mild to advanced, according to Glaucoma Grading Scale (HODAPP), cataract condition, treatment with two or more glaucoma medications; uncontrolled was defined as progression in at least 2 visual fields and/ or retinal nerve fibre layer thinning in spfectral domain optical coherence tomography (sdOCT),
Exclusion Criteria: history of glaucoma surgery, any subsequent glaucoma surgery in the follow-up period, narrow angles or closed angle glaucoma, neovascular, uveitic or other secondary glaucoma, retinal or neurophthalmic diseases.
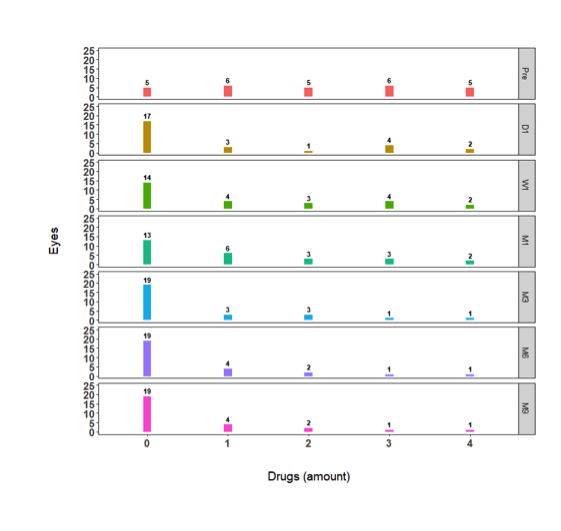
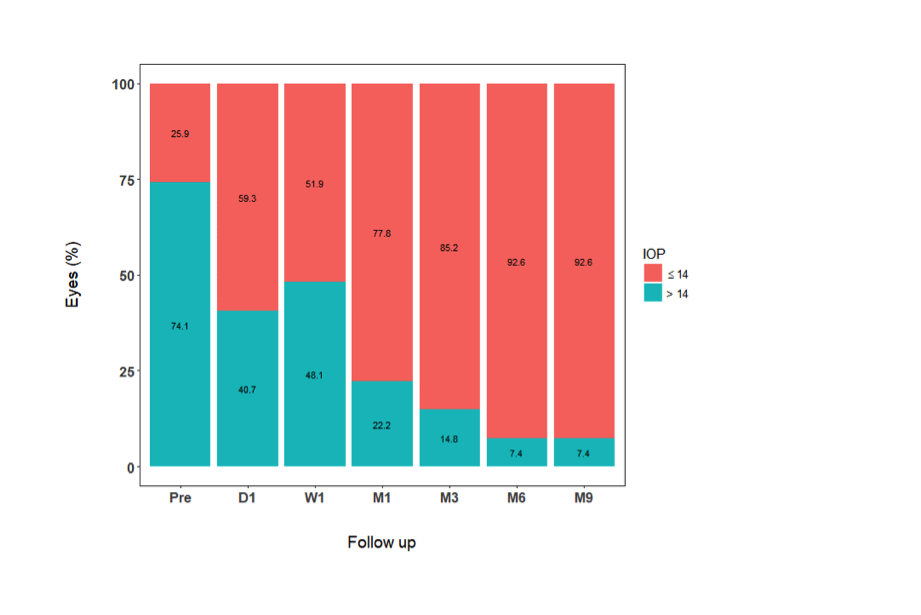
The intraocular pressure (IOP), best corrected visual acuity (BCVA) LogMAR and number of glaucoma medications were recorded prior to treatment, at day 1, week 1, and 1, 3, 6 and 9 months after surgery. At each visit, the IOP was measured with a Goldmann applanation tonometer. The intra and postoperative complications were recorded. Success was defined as IOP <14 mmHg with or without glaucoma medication.
Surgical modified Technique:
All procedures were performed by the same surgeon (JCI). Firstly, phacoemulsification and IOL implantation was performed using 2,2mm keratome and 1.20 mm side-port blade, the anterior chamber was filled with preservative-free lidocaine 1%, and an ophthalmic viscosurgical device (OVD) (Healon GV; Abbott Medical Optics, Santa Ana, CA, USA). Continuous curvilinear capsulorhexis (CCC) was created with a capsulorhexis fórceps and lens segmentation was performed by using a stop and chop technique. Surgery was completed by implantation of an intraocular lens (IOL) in the capsular bag after successful removal of the lens cortex.
Secondly, ECP (Endo Optiks® E2 Ophthalmic Laser Endoscopy System, Beaver-Visitec International, Inc. USA) containing an endoscope, an illumination source, the diode LASER (810 nm) and a helium-neon aiming beam, was inserted into the anterior chamber via the main corneal incision. Once the intraocular lens (IOL) was positioned in the bag, viscoelastic was injected to expand the sulcus behind the iris, and the diode laser ablation of the ciliary processes was performed under direct visualization via a 20G endoscope. In order to reach 360 degrees of the ciliary processes, a second incision 180 degrees away from the initial incision was made. The physical goals of treatment were to whiten the ciliary processes and cause visible shrinkage of the tissue, avoiding rupture. The 2-site corneal incisions 360 degrees were treated successfully with 0.2W energy on continues mode (Figure 1).
Finally, a 2.2 mm wide iris planar clear corneal incision is fashioned approximately 2 mm anterior to the surgical limbus and viscoelastic was used in the anterior chamber. The patient’s head was rotated 40 degrees away from the surgeon and the microscope was tilted in the opposite direction for gonioscopic visualization, with the goniolens (AVG; Surgical Gonio Lens, Volk Alcon, Mentor, OH, USA). Trypan blue was use to stain the TM. The Kahook dual-blade (KDB; New World Medical, Rancho Cucamonga, CA, USA) was engaged in the TM just anterior to the scleral spur for a more pointed entry into the meshwork and was advanced 90 degrees parallel toward the wall of the canal. Intracameral dexamethasone 0.8 mg/0.2 ml was administered to all patients in addition to standard cataract antibiotic prophylaxis (intracameral cefuroxime 1.0 mg/0.1 ml). The corneal incisions were then closed with 10-0 nylon (Figure 2).
Postoperative care routinely included tobramycin 3mg/ml and dexamethasone 1mg/ml (Trazidex, Sophia, México) 6 times daily tapered over 1 week, and pilocarpine 1% (Pil, Sophia, México) 3 to 4 times daily tapered over 4 weeks. In all cases, the glaucoma medication was discontinued at the time of surgery and restarted in selected cases according to IOP.
Statistical Analysis:
To compare the changes in IOP according to the observation period, the non-parametric Friedman test was used, followed by a post-hoc Nemenyi multiple comparison test. For change in the number of glaucoma medications, the signed test for paired samples was used. Statistical tests we considered significant if p value was less than 0.05. The analysis was done with statistical software R, versión 3.4.3 (https://www.r-project.org/).
{kind=link}
{kind=link}
{kind=link}