In November 2020, the World Health Organization (WHO) launched a strategy to reduce the current worldwide incidence from 13.3 per 100,000 (age-adjusted) to 4 per 100,000 women by 2030 as the first step towards elimination of cervical cancer [15]. Recently, National Health Commission of China published cervical cancer screening program regarding introduction of primary HPV testing and cytology test, the focus of which is on rural women and urban subsistence allowance women. By the end of 2025, more than half of women with appropriate age will be screened for cervical cancer. This program will promote early diagnosis and treatment of cervical cancer. In China, the prevalence of the disease is still relatively severe due to inadequate women vaccination and HPV screening coverage, especially in rural areas. In addition, the prevalence and genotype distribution of HPV differ by geographic areas. There are few reports on HPV prevalence in Fujian Province, especially in Xiamen. As an inflowing city, the population composition of Xiamen is progressively complex due to numerous migrant populations. Thus, it is of great significance to comprehend the overall HPV prevalence and genotypes distribution to formulate prevention and strategies about elimination of cervical cancer.
Among the participants in this study, the overall HPV positive rate including HR-HPV and LR-HPV was 15.13%, which was consistent with the study demonstrated the overall prevalence of HPV infection in China (15.54%) [16].Some results from other cities of China also reported the similar HPV prevalence [17,18,19,20,21]. However, the HPV prevalence reported was higher than Shannan (8.16%) [22] and Xinjiang (9.34%) [23] but was lower than Zhejiang Province (22.3%) [24], Beijing (22.7%) [25], Jiangxi Province (22.49%) [26] and Heilongjiang Province (27.1%) [27]. The variability of HPV prevalence may be accounted to diverse geographical condition and economy developmental level. Compared with the 2 studies reported about Fujian Province, we found that our result was significantly lower than Fuzhou (38.3%) [28] and Quanzhou (22.5%) [29]. This result suggested that the prevalence of HPV in Fujian province decreased significantly from 2009 to 2021. Considering the same laboratory method (flow-through hybridization technique) used in these reports, the differences might be attributed to differences in study period and progressive clinical use of HPV vaccination.
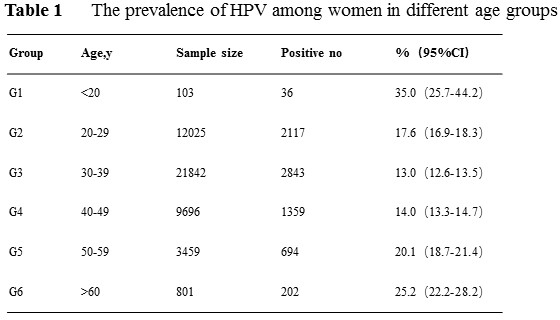
Results regarding age-specific HPV infection is pivotal for next stage of cervical cancer prevention. Numerous reports showed that HPV infection rate was significantly age specific. In the present study, we discovered that women under 20 years old had the highest HPV infection rate. Women in the > 60 years old group had a smaller peak of HPV infection rate. HPV infection in women aged 20–49 years old gradually decreased, reached the lowest in the age group 30–39 years old, and then showed a progressively upward trend. In conclusion, age-specific HPV distribution in our study was shown as a bimodal “U” curve, in line with most of the other reports [30,31]. There are possible reasons explained for this phenomenon: On the one hand, young women were sensitive to HPV due to relatively frequent sexual activity without protective measures and their non-sensitized immune system[32]. However, it was reported that majority of young women infected with HPV was transient, the immune system would protect them from persistent HPV infection [33]. Hence the HPV infection rate gradually decline with age. On the other hand, for women aged over 60 years, continue infected with the virus or latent HPV reactivation due to physiological disorder like hormonal level changes may result in immune disorder, presenting as a risk factor for cervical cancer development [34].
Furthermore, we observed that women aged under 20 years old and aged over 60 years old were more sensitive to HPV, whether for single, double, or multiple infection. Host susceptibility and virus characteristics may account for this phenomenon [35]. Therefore, it is pivotal for adolescents to be vaccinated to reduce HPV primary infection. In addition, it is recommended that aged women should involve in cervical cancer screening regularly.
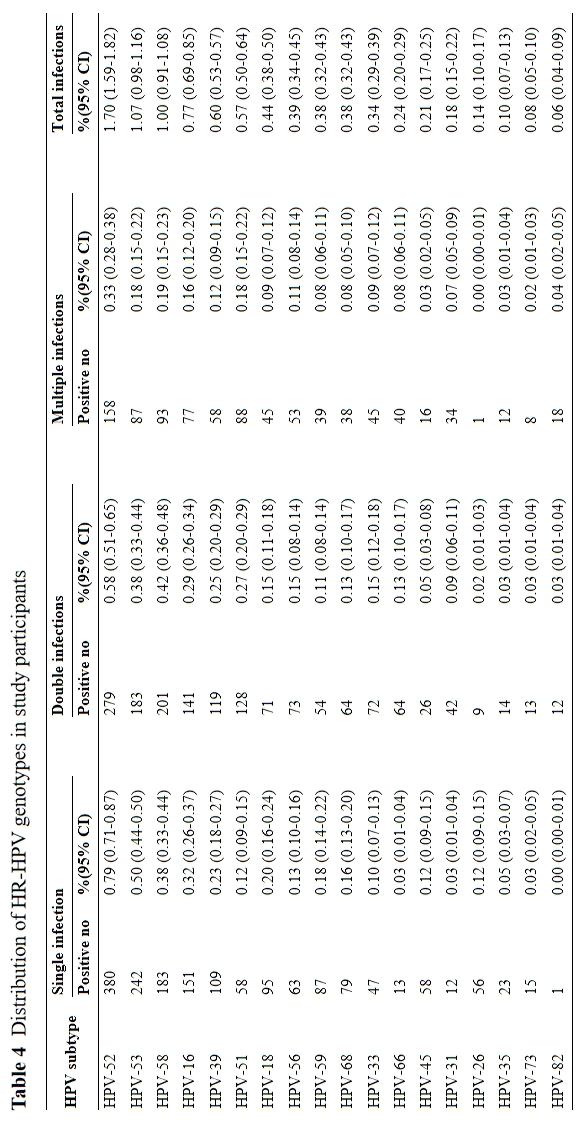
In the present study, we analyzed the age-specific distribution of single, double, and multiple HPV prevalence. Whether multiple infection increase the risk of cervical cancer has yet to be concluded. Some studies demonstrated that multiple infections displayed longer duration of HPV infection compared to single infection, which may result in cervical cancer occurrence [36].On the contrary, some studies found that single HPV infection had more risk of developing cervical cancer than multiple infections, the possible pathogenic mechanism of which could be competition or counterbalance between various HPV subtypes [37,38].Specific mechanism of whether single or multiple HPV infections have greater risk of developing cervical cancer deserves further investigation.
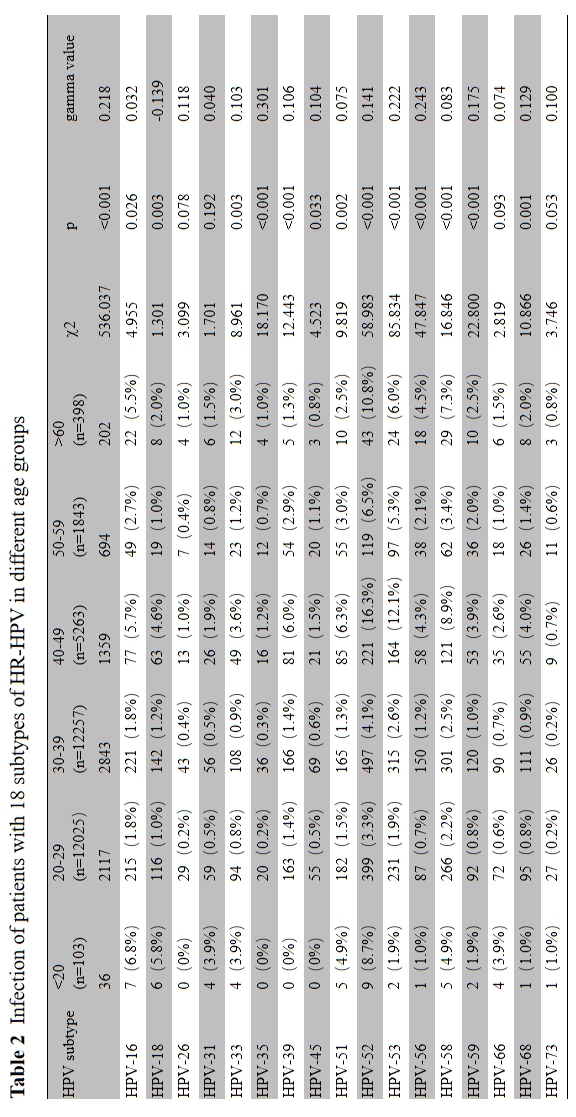
The most prevalent genotypes of HPV among women varies greatly in different regions. Therefore, specific HPV prevalence data is closely conducive to future vaccine development. According to a HPV epidemiological report carried out in mainland China, the five most common HPV subtypes were HPV16, 52, 58, 53 and 18 [39]. Other studies have reported the high HPV infection rate of HPV16, HPV52, HPV58 in northern Henan [40]. However, similar to the study concerning Jilin [41], we found a HPV genotype distribution that HPV52 was the most prevalent in this area, followed by HPV53, 58, 16 and 51. 70% of the HR-HPV DNA detected in cervical cancer patients were HPV16 and 18. HPV16 ranked fourth in our study. To be noted, HPV18 only ranked seventh in HR-HPV to be detected, which was consistent with the recent studies reported in other regions [40,42,43]. This phenomenon could be due to the bivalent vaccine against HPV16 and 18 applied to clinical practice. Besides HPV16 and 18, both HPV52 and 58 has been reported to be potent oncogenic factors inducing intraepithelial neoplasia [37,44]. To be noted, HPV53 ranked second in the present study, which was similar to the report in Xi’an [18]. However, the pathogenicity of single HPV53 infection was low [45]. Besides HR-HPV, the present study also investigated the prevalence distribution of LR-HPV. We found that HPV54, 61 and 81 were the most common LR-HPV, none of which are targeted by present vaccines. Unlike HR-HPV, LR-HPV have few associations with cervical cancer but result in proliferative lesions.2 HPV vaccination is not only conductive to women’s health but also can save a lot of medical expenses. The present study supports the recommendation of the 9-valent vaccine for HPV vaccination in Xiamen. Meanwhile, Vaccines targeting HPV53 and 51 are the next research direction to efficiently protect HR-HPV infection.
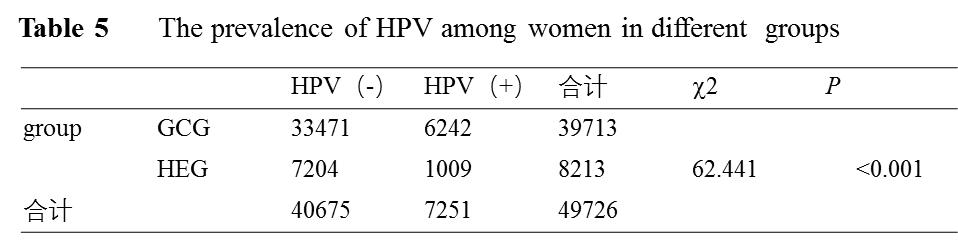
Since the participants in this study included outpatients and health examination subjects, we analyzed total HPV positive rate and distribution of HPV subtype infection rate in the two different groups. As imagined, we found that HPV infection rate was higher in outpatients than health examination subjects. Both groups showed similar HPV subtype distribution, which means that there was no obvious HPV subtype characteristic when one considered whether to attend gynecology clinics.
Although this study reported a large-scale information on HPV prevalence and genotype distribution in Xiamen, there are some limitations should be addressed. First, our results were not combined with cytology results. Second, the design of our study was cross-sectional, temporal trend of HPV prevalence is recommended to provide better conditions for deeper research.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}