A 59 years old man complaining of hemoptysis and chest pain was admitted to our hospital. Four months ago, Chest computed tomography (CT) revealed a 43×26 mm parenchymal nodule in the posterior right upper lung lobe accompanied by emphysema, while the patient did not pay attention. One month ago, the patient had hemoptysis without obvious inducement, accompanied by progressive shortness of breath, drenching night sweats, diminished appetite and a 5-kg weight loss, chest pain and fever. The chest enhanced CT scan showed that the right lung lesion was significantly larger than previous, and there were multiple nodules in both lungs. The patient has a history of smoking for 30 years (20 cigarettes per day) and drinking for 40 years (200g per day).
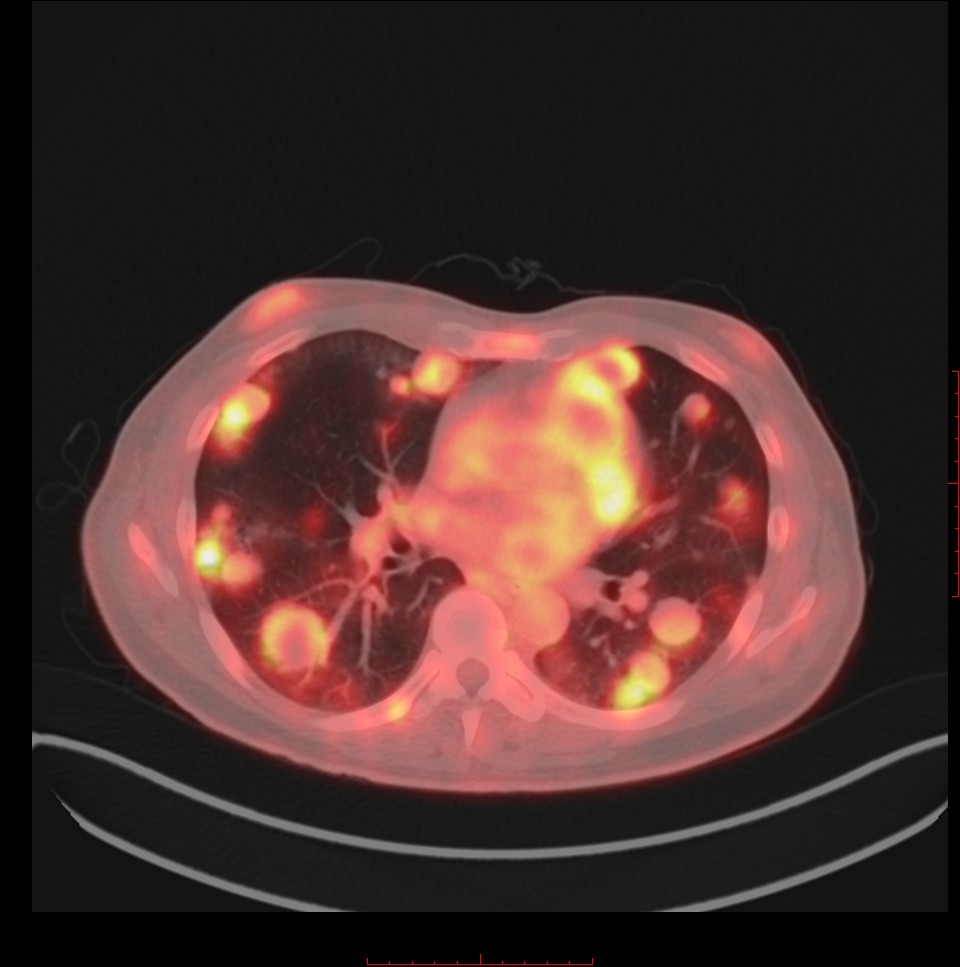
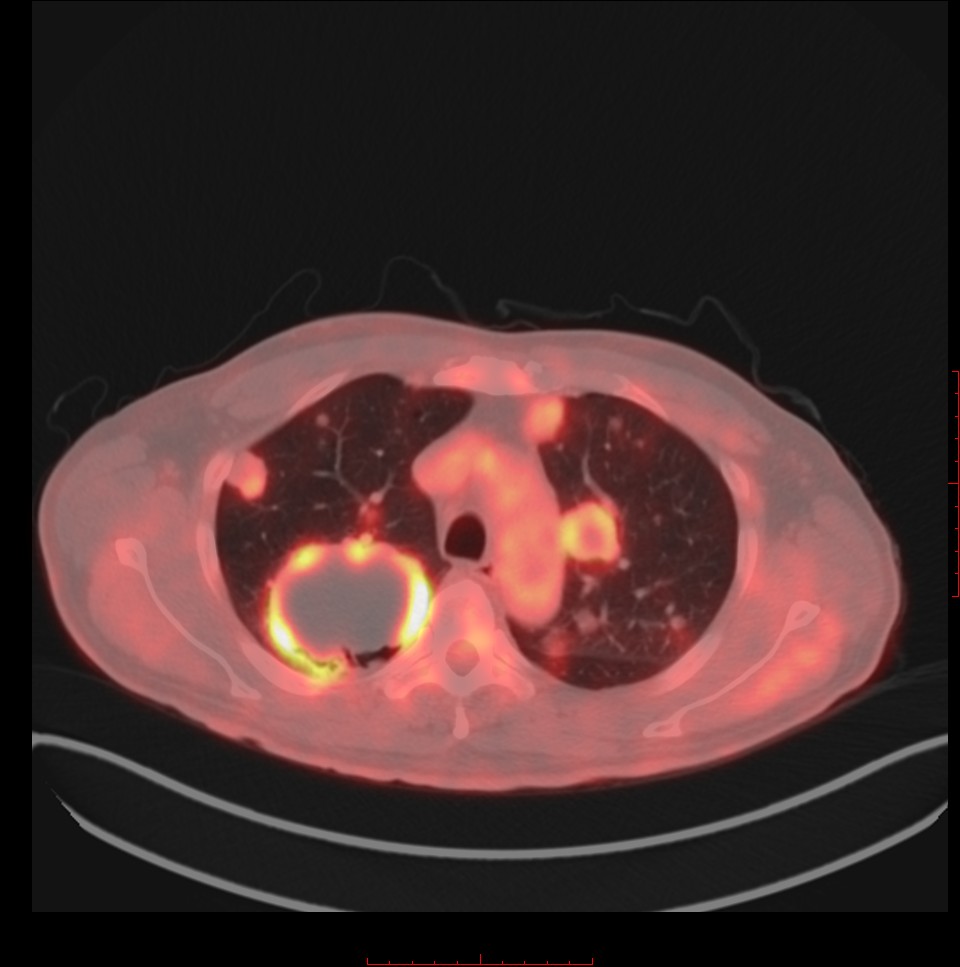
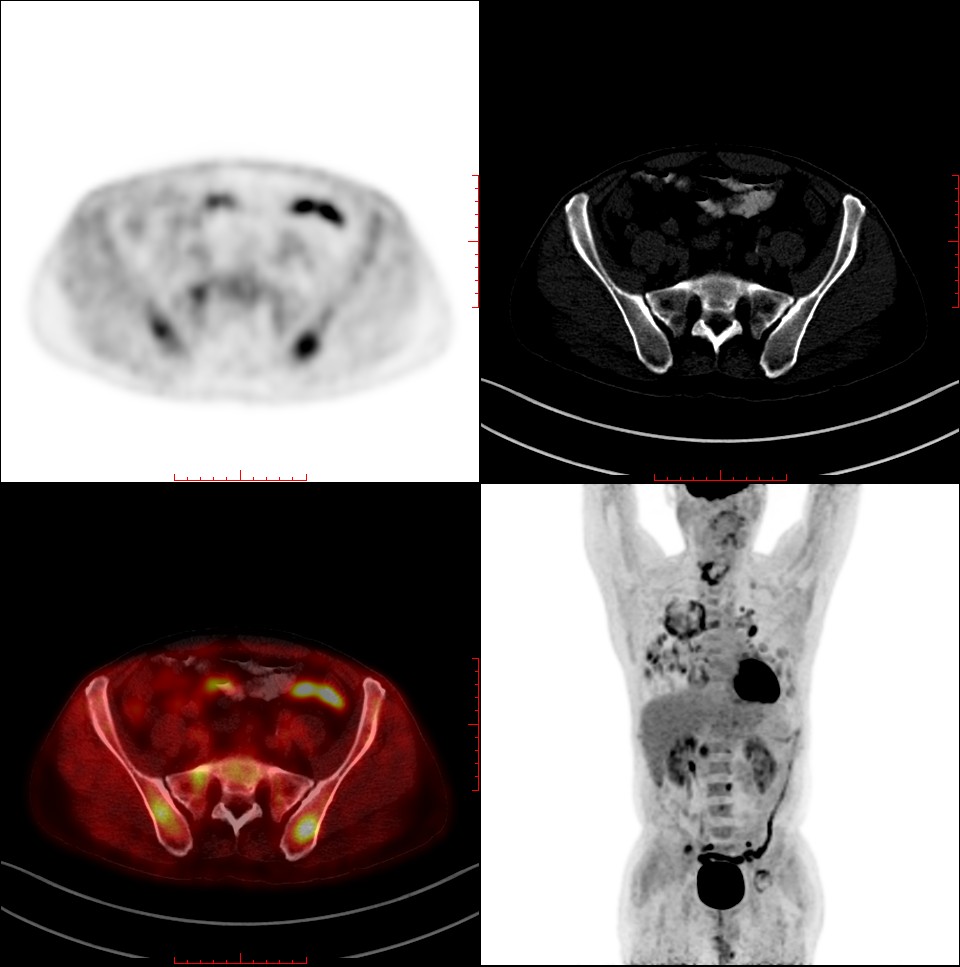
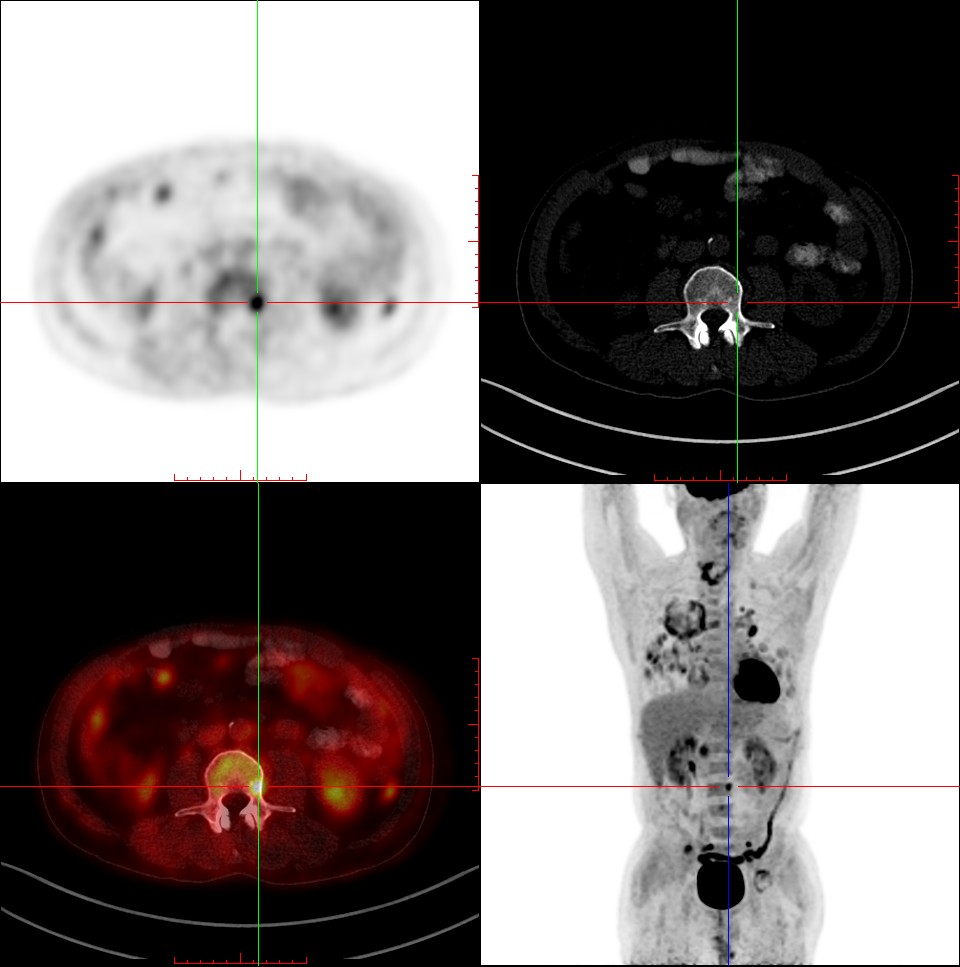
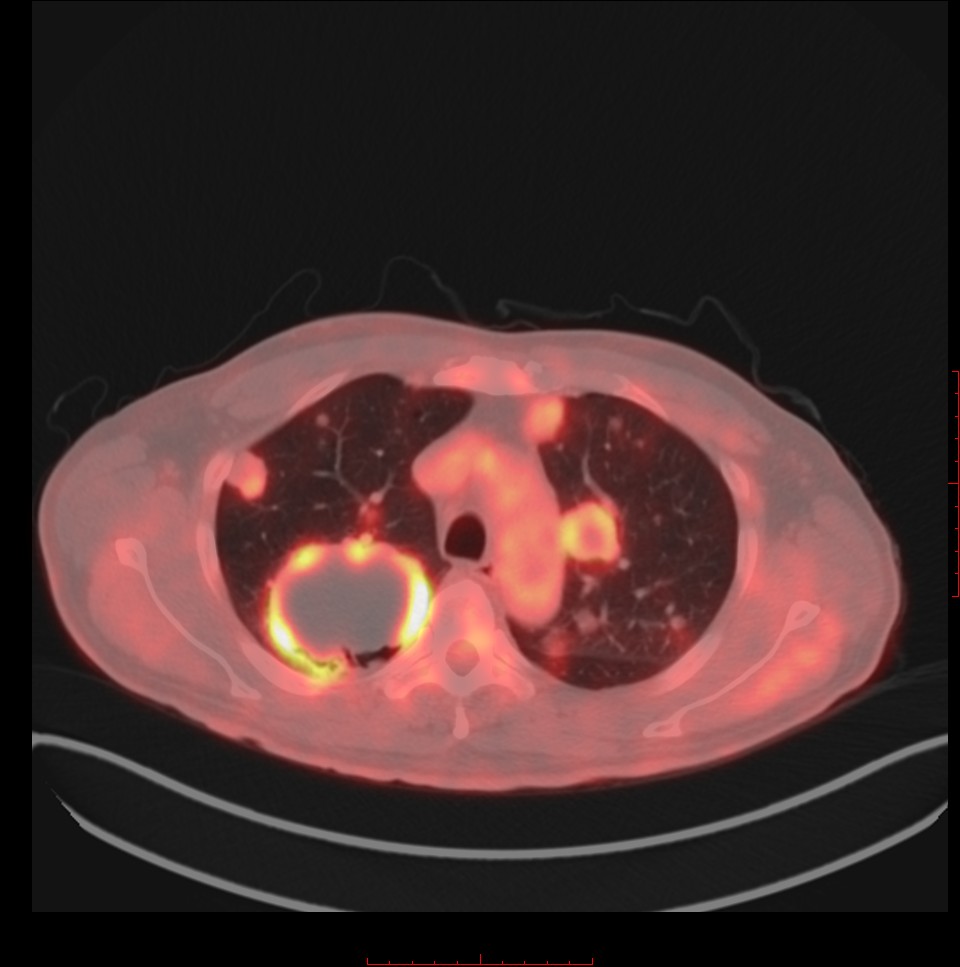
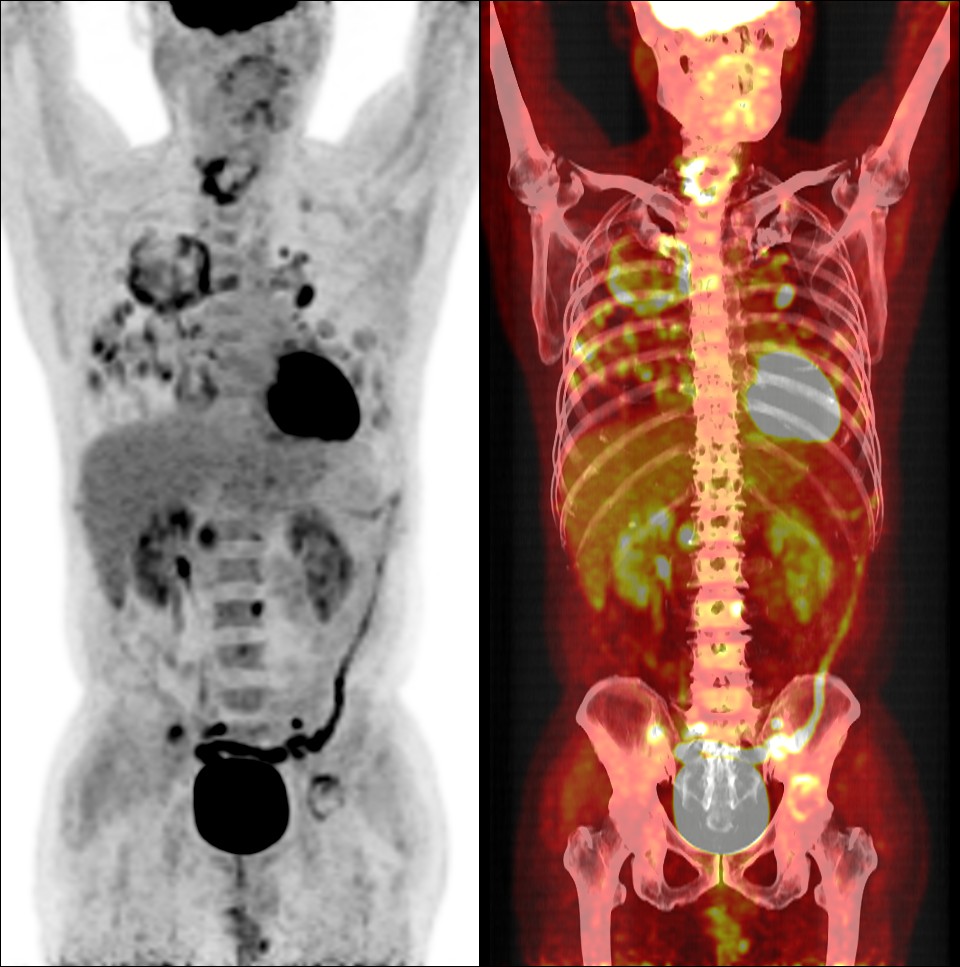
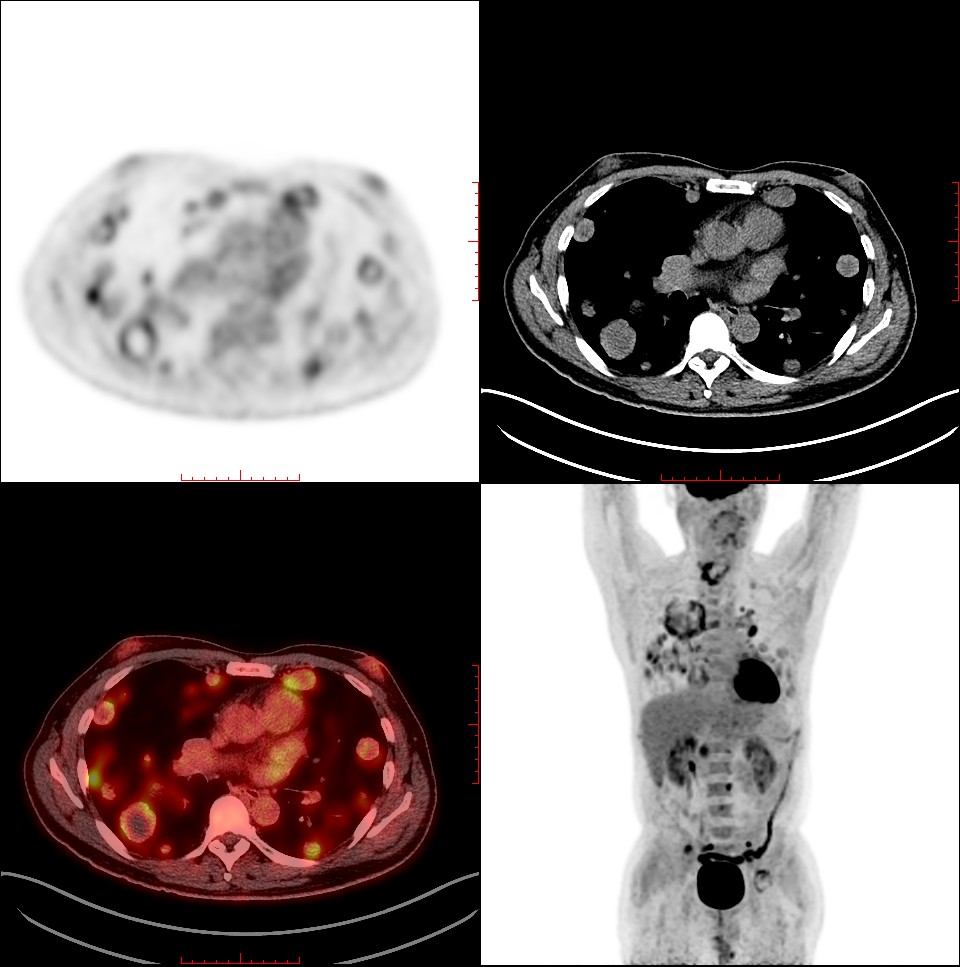
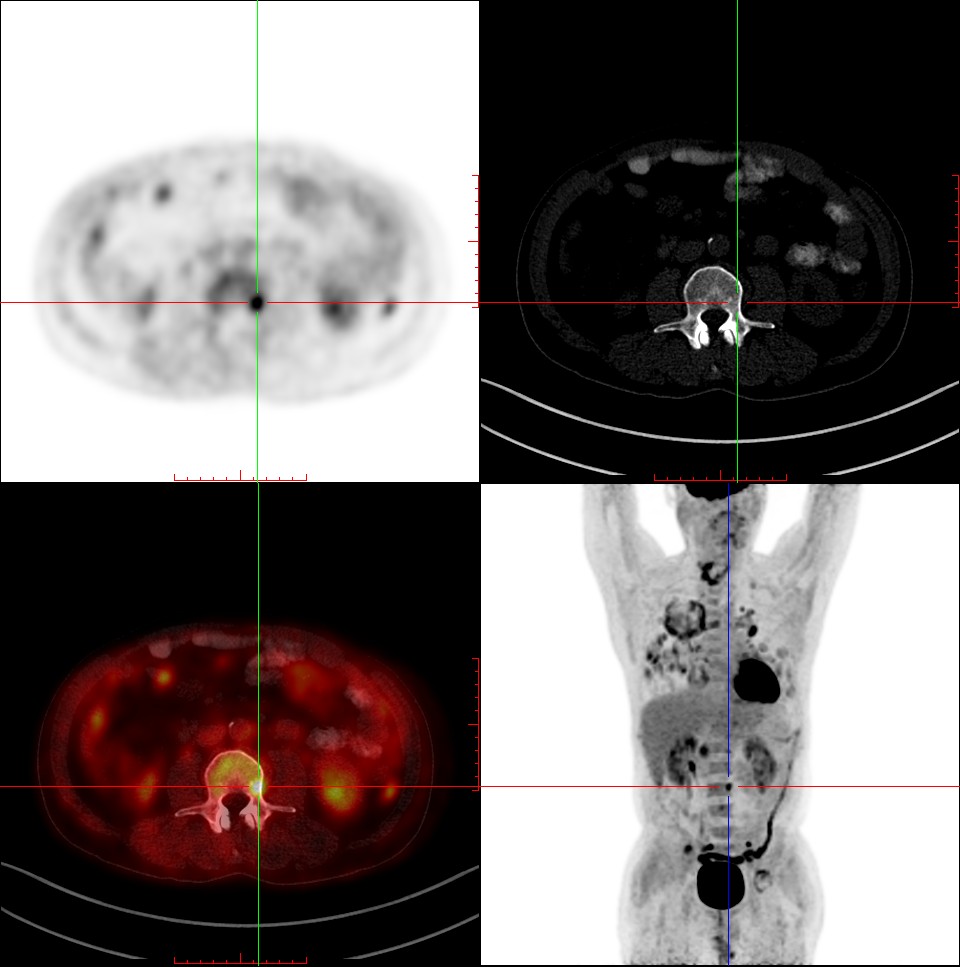
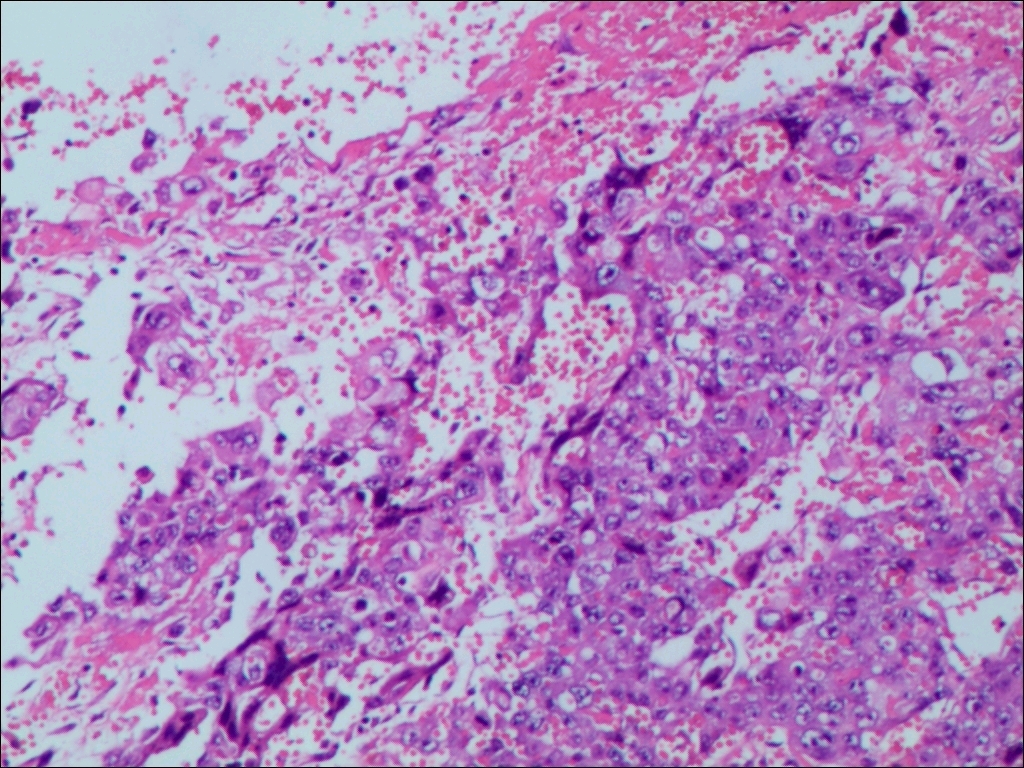
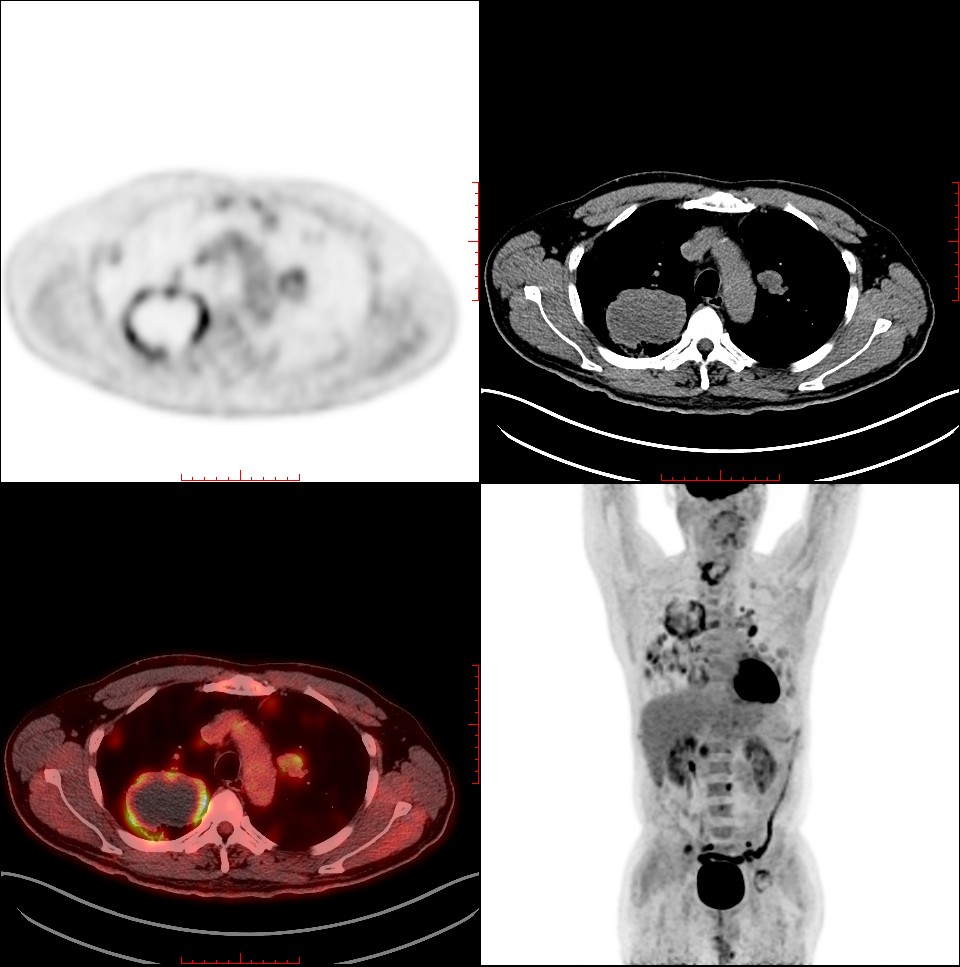
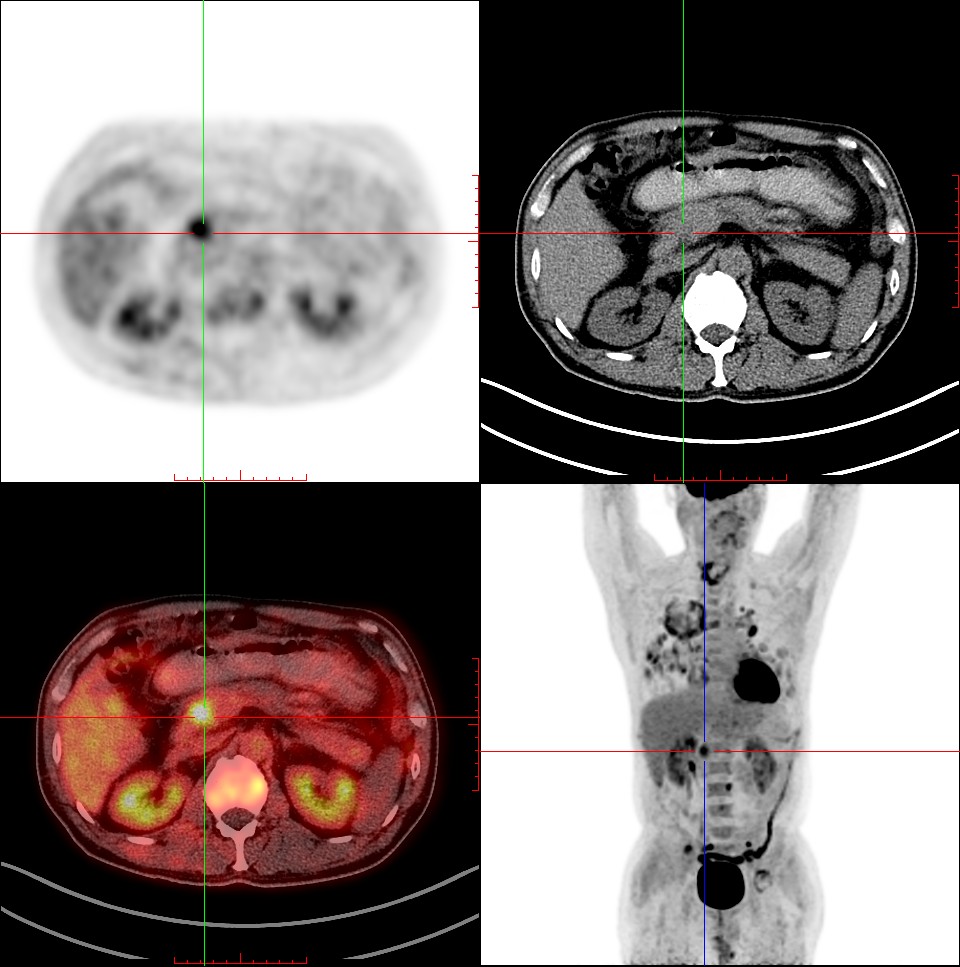
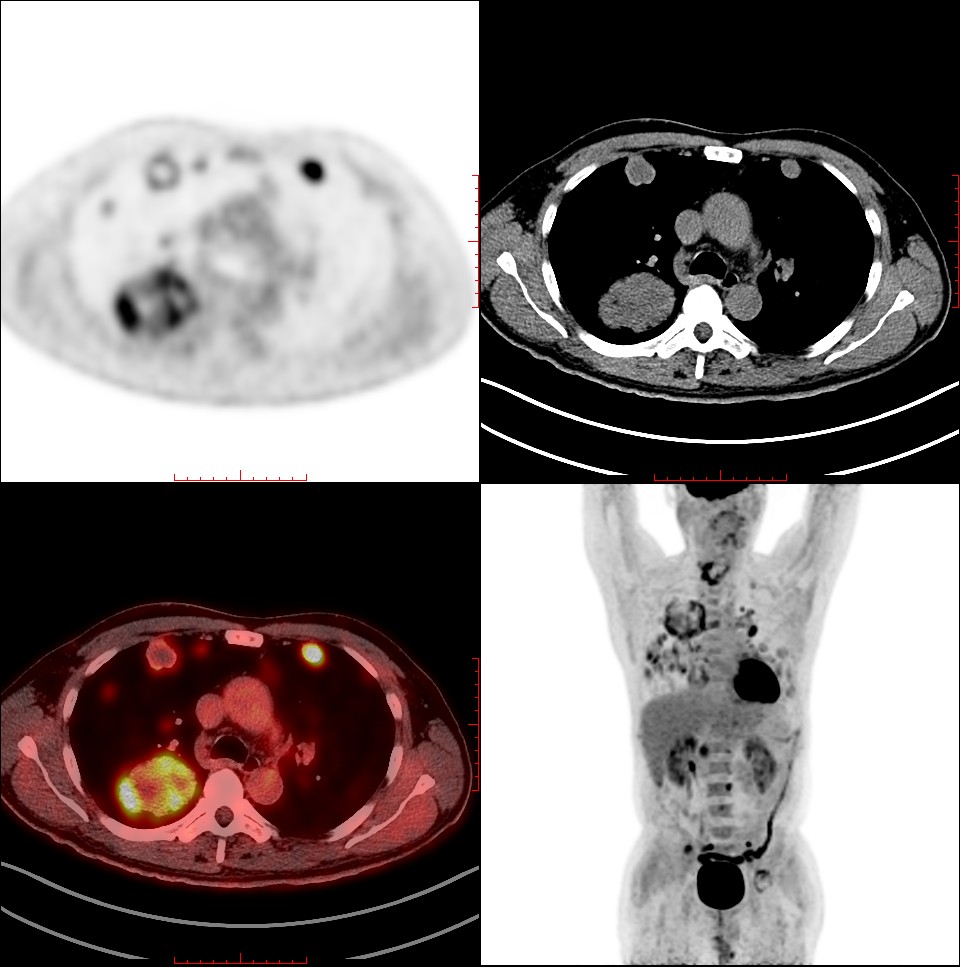
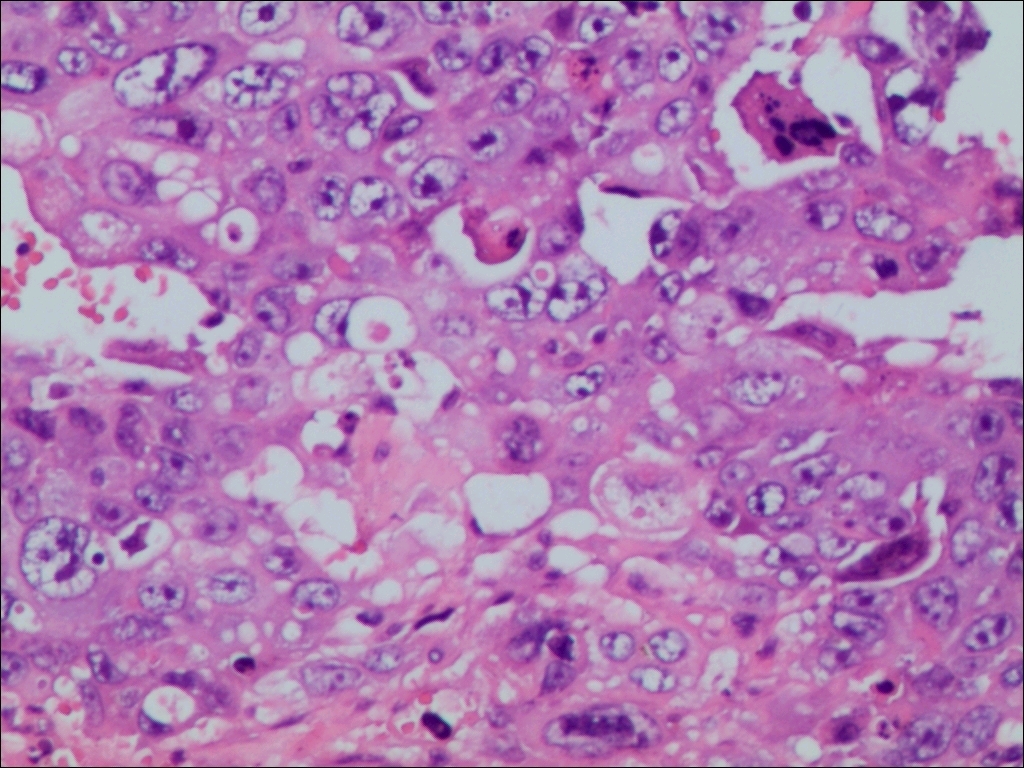
After admission, genital exam did not reveal any scrotal mass. The remainder of the physical examination was unremarkable. Chest x-ray was significant for bilateral pulmonary nodules. Doppler ultrasound of the testes and mammography of breasts were negative for malignancy. To determine whether the tumor occurred primarily within the lung systemic screenings were performed by positron emission tomography-computed tomography (PET-CT). The results showed that multiple high metabolic nodules throughout the body (Fig 1), multiple bilateral pulmonary nodules (Fig 2), especially large mass in the upper lobe of the right lung (Fig 3), a 22 mm metastatic lesion in the pancreas (Fig 4), and multiple bone metastases (Fig 5). The patient underwent single-port thoracoscopic wedge resection of the right lung upper lobe. Extensive metastases in the right lung were observed during the operation, with tumor diameters ranging from 2-6cm. Histopathologic workup of excised tumour showed poorly differentiated carcinoma and hemorrhage, with the few viable islands demonstrating syncytiotrophoblastic and cytotrophoblastic like cells (Fig 6). Immunohistochemical phenotype of pathological sections was that CK7(+),TTF-1(-),CK(+),CD34(-),CD117(-),OCT3/4(-),SALL4(+),HCGα(+),Ki67(+90%),Vimentin(-). Thus, we performed the serum β-HCG levels examination and the result was >10000.00(mlU/ml). The final pathological diagnosis was choriocarcinoma that met the diagnostic criteria for PPC.
Three days after the operation, the patient suddenly appeared consciousness disorder, sweating profusely and pinpoint pupils. Heart rate of the patient increases and the blood oxygen saturation continues to decrease. The patient was admitted to the ICU with tracheal intubation for respiratory support. A large amount of bloody fluid was sucked out of the bilateral main bronchus using bronchoscopy. The chest radiograph showed that multiple cluster and nodular shadows scattered in both lungs. Laboratory data was significant for white blood cell 13.85 900/mm which prompt the pneumonia. Subsequently, the patient developed cardiac dysfunction, manifested by increased myocardial markers. Cardiac color doppler ultrasound revealed that ventricular wall motion is not coordinated; left ventricular diastolic function decreased; ejection fraction was 60%. Simultaneously, the patient suffered acute renal failure, the endogenous creatinine clearance rate continued to decrease, to a minimum of 10.01 (ml/min/1.73m2), and urea and creatinine continued to rise. Despite supportive treatment, the patient’s condition continued to deteriorate. Due to multiple organ failure, the patient has no indications for chemotherapy and eventually died. Diagnosis of death: 1. Pulmonary choriocarcinoma with metastasis to the lung, brain, bone, pancreas, and lymph nodes 2. Severe pneumonia and respiratory failure 3. Acute renal failure; 4. Acute coronary syndrome.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}