There are very limited data about current situation of carbapenem resistant Acinetobacter calcoaceticus-baumannii complex in Nepal [10] and prevalence of genes associated with carbapenem resistance [19, 20]. Our country needs yearly surveillance of genes circulating within CR-ACB complex. So, this study was conducted to detect three (blaNDM−1, blaOXA−23−like and blaOXA−24−like) out of many genes associated with carbapenem resistance in Acinetobacter calcoaceticus-baumannii complex.
ACB complex is one of the most important nosocomial pathogens and a member of ESKAPE pathogens [21] causing wide spread of diseases. Treatment of infections caused by ACB complex are difficult because ACB complex when isolated are usually multi-drug resistant [22]. Without appropriate prescription of antimicrobial agent, these infections can be extremely fatal. Carbapenems were the drug of choice for MDR-ACB complex infections, but recent resistance or reduced susceptibility to carbapenems is becoming serious clinical problems. Resistance to carbapenem is mainly due to genes that codes enzyme inactivating antibiotics, followed by loss of porin protein, presence of efflux pumps and alterations of targets or cellular functions due to mutations [5]. Genes that are most prevalent in causing carbapenem resistance is carbapenem hydrolyzing oxacillinases genes and metallo-β-lactamases genes [17, 23] which are also the focus of this study.
In this study prevalence of ACB complex among total clinical samples were 4.33% which is higher than other studies conducted in Nepal [20, 24] but is lower than some other study of Nepal [25]. This pattern of our study is probably due to the particular exclusion criteria of this study i.e., out-patients.
ACB complex can infect any organ or system of human body, hence it can be isolated from wide range of clinical samples [5]. In this study, ACB complex has been isolated from different samples such as bile, CSF, pus, wound swab, blood, tissue, sputum, tracheal aspirate, urine, bed sore, ET tip and CT tip. Although it was isolated from various samples, but majority of the ACB complex were obtained from respiratory samples (tracheal aspirate, sputum and ET tip) (48.83%) which are in agreement with results previously published from Nepal [19, 20] and other countries [26, 27]. Respiratory infection is the most common form of Acinetobacter infection which occur most frequently in critically ill patients particularly admitted in ICUs with mechanical ventilation [28, 29]. Since, the positive isolates in this study is mainly from ICU and 30.23% of the positive samples (tracheal aspirate and ET tip) were mainly from mechanically ventilated patients, thus it was an obvious finding that ACB complex were predominantly isolated from respiratory samples in this study. However, there are some other studies where ACB complex were isolated predominantly from other clinical samples such as blood [30, 31] and pus [32]. The rate of isolation of bacteria in different clinical specimens can be influenced by the site of the study, sample size, antibiotics used, hospital infection control practices, sources of infection etc. [32, 33].
In this study, higher number of isolates were isolated from males (58.14%) than from females (41.86%) which were similar from other conducted studies [30, 33]. Although, a study conducted in Saudi Arabia shown a higher number of females infected with A. baumannii than male [34].
Regarding antimicrobial susceptibility testing, all isolates of ACB complex were found to be resistant to third generation cephalosporin tested i.e., ceftriaxone and cefotaxime. Similar resistance (100%) to cefotaxime and ceftriaxone was reported by Khanal et al (2017)[35] from Norvic hospital, Nepal. However, unlike that study where resistance to fourth generation cephalosporin (cefepime) was 100%; in this study, resistant to cefepime was found to be 83.72%. Similar resistance (88.6%) was also reported by Joshi et al (2017)[19]. Although majority of cefepime sensitive isolates were obtained from carbapenem sensitive isolates suggesting that cefepime can be still used to treat carbapenem sensitive cases. On the other hand, complete resistance to cefotaxime and ceftriaxone indicates that these cephalosporins are no longer effective to treat Acinetobacter infection. This might be the result of overuse, misuse and most frequent use of these cephalosporins by patients, pharmacy and even by the clinicians. This higher resistance of cephalosporin is also due to hyper production of insertion sequence regulated by AmpC cephalosporinase that are intrinsically present in A. baumanii [36]. This seems most plausible, since cefepime seems to be stable in response to these enzyme [5] which seems relateble in this study. Moreover, other resistance gene may also play a role such as ESBL genes. Shrestha et al (2015) in her studies reported various ESBL genes such as blaPER, blaTEM and blaPSE genes in A. baumannii isolated from Insitute of Medicine, Nepal [10]. Also, production of carbapenemase such as OXA-types and MBL (which was actually detected in this study) also causes reduce susceptibility to oxyiminocephalosporins [9]. Thus, it can be the one of the reasons for third generation cephalosporin resistance. Furthermore, cefperazone and sulbactam combination had even more susceptibility rate (18.6%) than cefepime. Sulbactam is β-lactamase inhibitor and β-lactamase inhibitors such as clavulanate, tazobactam and sulbactam have intrinsic antibacterial activity against Acinetobacter species [37]. Therefore, cefperazone/sulbactam combination shown greater antimicrobial activity than other cephalosporins, even though cefperazone is also a third-generation cephalosporin. Similar results were demonstrated by piperacillin/tazobactam which exhibited higher susceptibility than third generation cephalosporins.
In this study, 65.11% of the isolates were found to be resistant to amikacin and 69.77% of the isolates were resistant to gentamicin. Similar resistance of amikacin (67.24%) and gentamicin (70.68%) was reported by Bhandari et al. (2015) [38]. However, there were other studies with contrasting results. To elucidate, Joshi et al. (2017) reported lower percentage of resistance to amikacin (43.2%) and gentamicin (52.3%) [19]. Increased resistance to gentamicin and amikacin in this study may be due to presence of aminoglycoside-modifying enzymes or presence of AdeEfflux pumps. In a study conducted by Shrestha et al (2016), 75 (78.12%) out of 96 aminoglycoside resistant A. baumannii isolates had armA gene while study conducted by Joshi et al (2017) reported 40.1% of aphA6 positive A. baumannii isolates [39]. These are probably the most common factors causing aminoglycoside resistance in this region of Nepal.
The resistance to imipenem and meropenem were found to be 81.4% which was quite different from others studies conducted. Joshi et al (2017) in his studies reported 97.7% resistance to carbapenem and Sohail et al (2018) reported 90.85% of carbapenem resistance: both of which obtained higher percentage of resistance than this study [19, 27]. However, there were other studies that published lower percentage of resistance than this study [34][20]. For decades, carbapenem was the drug of choice to treat MDR Acinetobacter infection, however resistance has increased tremendously all around the world. In Nepal, carbapenem resistance percentage has mounted immensely and resistance rate were reported from 17.24% [38] to 97.7% [19] implying that carbapenem resistance is in alarming state. There are various mechanisms responsible for carbapenem resistance which are carbapenemase production, decreased permeability, altered penicillin binding proteins and overexpression of efflux pumps. Although, OXA-type carbapenemase (Class D β-lactamases) and metallo-β-lactamases (Class B β-lactamases) are most common factor responsible for carbapenem resistance [5]. As one of the objectives of this study was to find two (blaOXA−23−like and blaOXA−24−like) out of many oxacillinase coding genes and one (blaNDM−1) out of many metolla-β-lactamse coding genes. In this study, 30 (85.71%) out of 35 carbapenem resistant isolates were found to have either blaOXA−23−like, blaNDM−1 or both genes explaining cause for carbapenem resistance.
Carbapenem resistant isolates left us with no treatment options except for polymixins (colistin and polymixin B), which was previously rejected drugs due to its higher side effects. In this study, colistin and polymixin B were 100% susceptible. This is in accordance with previous studies [19, 39]. On the contrary, there were some studies that reported resistance to colistin in some extent [20, 27]. Polymixins are last resort drugs and increasing resistance to them puts us in a dire situation with no treatment options. However, this study reported 100% susceptibility of polymixins implying polymixins are still effective to treat CR-ACB complex in this region. After polymixins, tigecycline was the most susceptible (60.47%) antibiotics. In Nepal, this kind of susceptibility were also published by Amatya and Aacharya (2015) while Shrestha et al (2015) reported 89% susceptibility [10, 20]. Different percentage of susceptibility were reported ranging from 99.3–25.2% from different parts of the world [27, 33, 40]. Surely to say, susceptibility of tigecycline is in decreasing rate.
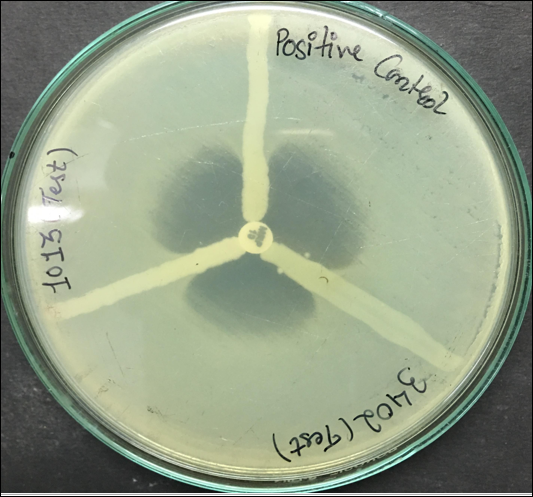
All carbapenem resistant strains were tested for carbapenemase production by Modified Hodge Test (MHT) as described by Lee et al (2001) [41]. 94.28% (33/35) were found to be MHT positive. All 33 isolates gave clover-leaf shaped indentation indicating production of carbapenemase. MHT test is able to detect Class A [42], Class B and Class D carbapenemases [41]. Although, it is supposed to have poor sensitivity for Class B carbapenemases [42], that was not observed in this study.
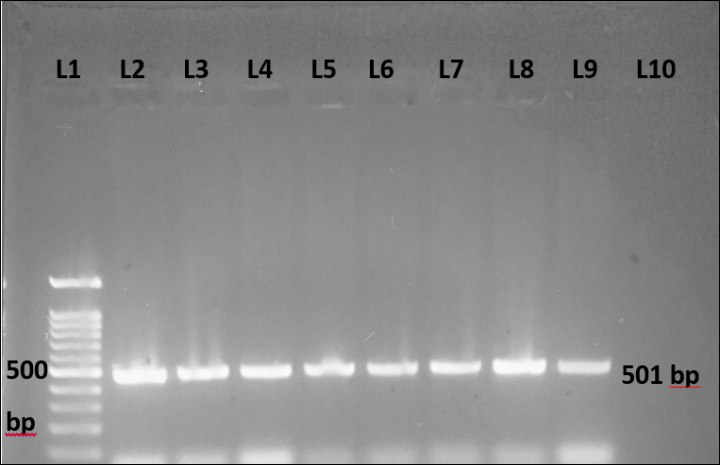
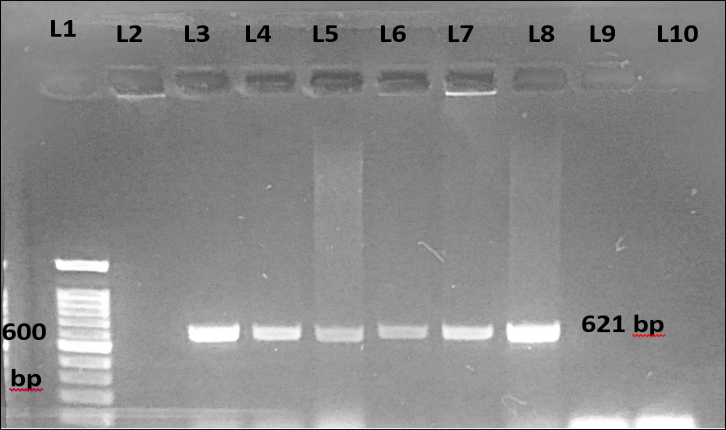
Carbapenem resistance in ACB complex develops predominantly by production of carbapenem hydrolyzing enzymes, OXA-type carbapenemase and MBLs mainly. Widely reported carbapenemases are blaOXA−23−likE, blaOXA−24−like, blaOXA−58−like, blaOXA−51−like, blaNDM−1 and blaIMP, where blaOXA−51−like is intrinsic to A. baumannii and can be used as a species identification marker. Among them, blaOXA−23−like is most frequently detected. But, now-a-days blaNDM−1 is also circulating widely among various bacteria, Acinetobacter and members of family Enterobactericeae being the predominant one. Keeping that in mind, PCR was performed for determination of blaNDM−1, blaOXA−24−like and blaOXA−23−like genes in CR-ACB complex in this study. 82.5% (29/35) of carbapenem resistant isolates were found to have blaOXA−23−like gene and 34.28% (12/35) of isolates were positive for blaNDM−1 gene. 31.42% (11/35) of the isolates were positive for both blaOXA−23−like and blaNDM−1 genes. Only one isolate was found to have only blaNDM−1 gene. However, blaOXA−24−like gene was not present in any of the isolates. 5 of the isolates didn’t have any of the tested genes.
In previous molecular studies conducted in Nepal, blaOXA−23−like gene were present in higher number than in this study. For instance, Shrestha et al (2015) reported 95.08% of the test isolates contained blaOXA−23−like gene. Likewise, Joshi et al (2017) found 100% blaOXA−23−like gene positive isolates in his study. Their data were slightly different than this study, probably due to the fact that their test isolates were only A. baumannii while this study included A. nosocomialis and A. pittii along with A. baumannii (thus, ACB complex). In a study conducted in Taiwan [3] where test isolates were also ACB complex yielded almost similar result (80.36%) as this study. On the other hand, blaNDM−1 positive percentage were higher than the other studies conducted in Nepal meaning this gene is increasing and circulating widely in this country and speculated reason for this can be ability of A. baumannii to transfer this gene via conjugation to the recipients, where Tn125 act as a main vehicle for dissemination [43].
MBLs (such as blaNDM−1, blaIMP, blaSIM) confers high resistance to carbapenem, almost 100–1000 fold than OXA-type carbapenemase [5]. Moreover, blaNDM−1 confers resistance to not only to carbapenem but also to penicillins and cephalosporins [44]. Similarly, blaOXA−23−like renders resistance to carbapenem, oxyiminocephalosporins, piperacillin, aminopenicillins, oxacillin and aztreonam [5, 45]. This explains the pattern of antibiotic resistance in carbapenem resistant and carbapenem susceptible ACB complex (Table 4) in some extent. Cefperzone/sulbactam, piperacillin/tazobactam and cefepime were almost 100% susceptible in carbapenem sensitive isolates while almost 100% resistant in carbapenem resistant isolates.
This study was not able to detect any blaOXA−24−like gene. Majority of the isolates contained either blaOXA−23−like, blaNDM−1 or both genes. Although one of the recent studies [46] does published result showing co-occurrence of blaOXA−23−like and blaOXA−24−like genes in one isolate but in most of the studies that does not happen to be the case [47, 48]. In this study, as blaOXA−23−like and blaNDM−1 genes were already present in those isolates causing blaOXA−24−like gene to be negative in them. One of the recent study detected blaOXA−24−like gene in inpatients of Patan Hospital, Nepal [49] and the studies by neighboring countries such as India and China have repeatedly reported it [12, 13], thus it might be circulating in Nepal but due to some of the sample bias or sample size, it might have come negative in this study.
Out of 35 carbapenem resistant isolates, 30 isolates harbored tested carbapenem resistance genes but 5 were negative for any of the tested genes. Those 5 isolates may harbor other carbapenem resistance genes that this study did not test such as blaOXA−58−like, blaIMP, blaSIM, blaVIM, blaKPC, blaSME etc. or it may be resistant to carbapenem by other non-enzymatic methods such as efflux pumps, loss of porin proteins and altered penicillin binding proteins.
Lastly, this study highlighted the increasing problem of carbapenem resistant ACB complex in clinical setting. CR-ACB complex which when isolated was resistant to wide groups of antibiotics that marks the major problem. Accurate microbial techniques for diagnosis of this organism are necessary for appropriate treatments. Infection by this organism can be managed and reduced properly by regular fumigation of ICU and wards in hospital, regular monitoring of organisms in those areas and finally, restricted use of antibiotics.
{kind=link}
{kind=link}
{kind=link}