This study demonstrated the viability of a shorter, less expensive 3-dose melarsomine protocol in a shelter setting. The incidence of new respiratory signs following melarsomine treatment did not differ between dogs that received M1 early and those that did not. Respiratory complications during melarsomine treatment were uncommon and typically required little intervention. Compared with AHS guidelines, the current THS protocol shortens the duration of treatment by 6 weeks. In addition to the benefits of earlier parasite death, a shorter treatment period decreases shelter length of stay and the duration of exercise restriction, thereby improving animal welfare and increasing life-saving capacity. Further, 10 mg/kg doxycycline SID, rather than BID, was not associated with higher incidence of respiratory signs after melarsomine. There was a lower incidence of GI signs during SID doxycycline treatment, although this difference was not statistically significant.
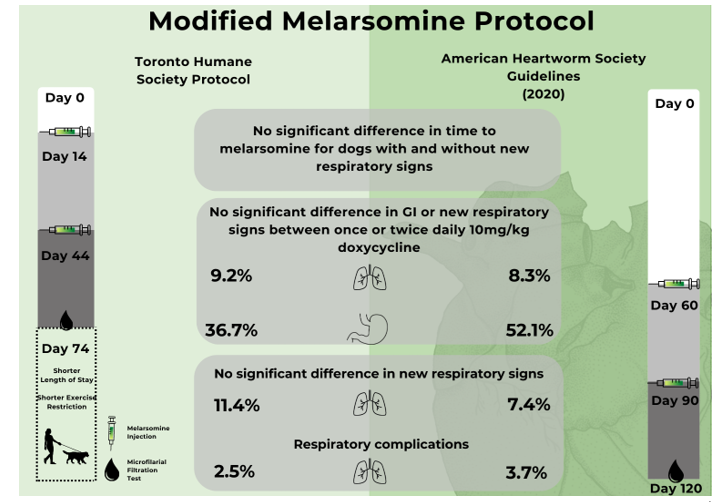
New respiratory signs following melarsomine occurred in 8.9% of all dogs, 11% of Group A and 7.4% of Group C. In early clinical trials of melarsomine (without doxycycline), more than 40% of dogs had “pulmonary reactions”, including coughing, gagging, panting, increased respirations and dyspnea [22]. Coughing or gagging alone occurred in 22.2% of dogs with Class 1–3 HWD, and dyspnea in 2.6% [22]. Another study reported mild signs (primarily cough and lethargy) following doxycycline and melarsomine treatment in 4/15 dogs (26.7%) [23]. These dogs all had high parasite burdens on ultrasound examination. A study that included all classes of severity found a high incidence of respiratory complications in dogs receiving doxycycline and 3-dose melarsomine (48%), but these were mild in all dogs with Class 1 HWD [24]. Nelson et al (2017) reported respiratory signs post-melarsomine in 6.5% of 47 client-owned dogs that also received doxycycline, and 19% of 47 dogs that did not. Finally, a more recent study, that used multiple adjunctive treatments, reported coughing and mild dyspnea in only 1/44 (2%) of dogs [25]. Incidence in our study was influenced by the liberal case definition for respiratory signs, and possibly by heavier parasite burdens in a shelter population. Other than the study that included Class 3 and 4 HWD [24], no deaths attributable to HWD were reported in the recent studies above, as was the case in the current study.
This study was the first to record respiratory signs and complications during different HW treatment periods. A previous clinical study reported, pre-treatment, harsh lung sounds in 17.3%, cough in 16.2%, dyspnea in 1.8%, and PTE in 0.7% prior to treatment [26]. The high pre-melarsomine incidence of signs, particularly cough, in our study, might have been caused by clinical manifestations of HWD, but this would not explain why far fewer dogs had respiratory signs in TP2 and TP3, the periods during which respiratory signs might be expected to occur due to rapid adult worm death. Possible reasons for this are over-reporting before fostering, while dogs were being closely observed by multiple staff members and volunteers; concurrent infectious respiratory disease at admission; reduced respiratory signs after exercise restriction was implemented; and, in rare cases, respiratory reactions to rapid die-off of microfilariae following ML treatment [27, 28].
There is compelling evidence for the benefits of doxycycline in treatment of HWI [1, 5–11]. At least some delay prior to M1 is advisable, in order to allow time for doxycycline to take effect. At issue is the precise amount of time that is optimal. Safe and effective administration of melarsomine 30 days after initiation of doxycycline was demonstrated in 76 naturally infected dogs [13]. Most dogs (61%) in that study had clinical HWD, and 17% had a high parasite burden on ultrasound examination. Our results support initiation of melarsomine after two weeks of doxycycline. A full 28-day course of doxycycline was completed in all dogs and remains advisable, based on current knowledge.
The use of doxycycline at 10 mg/kg PO SID, rather than BID, in the current THS protocol was based on lack of consensus between expert guidelines, absence of studies demonstrating superiority of BID dosing, cost advantages of less frequent dosing, and concerns about GI adverse effects [19]. In one study, doxycycline 10 mg/kg BID was superior to SID dosing, as measured by residual microfilarial Wolbachia DNA [14], but negative PCR or antibody tests may not be a necessary end-point for effective clinical reduction of the pro-inflammatory effects of Wolbachia. Our study showed no statistically significant differences between SID and BID doxycycline, for either new respiratory signs or for GI signs. However, a higher percentage of dogs treated BID had GI signs. This was consistent with an experimental study in which 4/8 dogs administered 10mg/kg doxycycline BID had GI side effects compared with 2/8 dogs receiving 5mg/kg BID [14]. Another study reported GI effects in 6% of dogs treated with doxycycline 10 mg/kg BID [25]. These resolved after reducing the dose to 5 mg/kg BID. Similarly, GI signs necessitated reducing doxycycline to 5 mg/kg BID in 12/50 dogs in an earlier study [24]. As with respiratory signs, the case definitions for GI signs in our study were liberal, with signs being mild and self-limiting in many cases. This most likely contributed to the reported high incidence. Many confounding factors, including stress, diet change and infectious disease, can cause GI signs in a shelter environment, and microfilarial die-off can also be associated with vomiting or diarrhea [27].
Non-respiratory complications of melarsomine treatment occurred in three dogs in our study. The most commonly reported adverse effects are injection site reactions, coughing/gagging, lethargy and inappetance, but a wide range of rare complications may occur [24, 29, 30].[1] Interestingly, injection site reactions were rare in our study (data not shown), possibly due to the fact that sedation and mu-agonist opioid analgesia are administered prior to injection as part of the shelter treatment protocol.
The exceptional efficacy of 3-dose melarsomine [1, 31] provides substantial confidence that this treatment will be successful. All tests performed > 3 months after M2/3 were negative in our study. This included 14 dogs tested four to eight months after M3. This is in agreement with a previous study, in which all antigen tests were negative six months after a shortened melarsomine protocol [13]. These findings support the absence of a “susceptibility gap” when using MLs, doxycycline and melarsomine, as previously outlined [12]; however, tests may remain positive beyond six months in some successfully treated dogs [1, 24]. Repeat antigen test results were only available for 44 dogs, a surprisingly low proportion and consistent with low retesting rates reported elsewhere [24], and few adopters tested at the recommended interval after treatment.
The study had several limitations, including its retrospective nature; the potential for non-HW-related causes of respiratory and GI signs in a shelter environment; and potential over-reporting of these signs. Clinical signs were reported if they were mentioned even once in the electronic medical record, rather than, as would be more typical in clinic records, if they were enough of a concern to require a consultation or intervention. Case definitions have not been proposed in previous studies that reported respiratory signs during HW treatment [7, 13, 24, 32–34]. These would be helpful for future comparisons between protocols.
[1] https://www.drugs.com/vet/immiticide.html, https://www.drugs.com/vet/diroban.html - accessed 5 October, 2022
{kind=link}