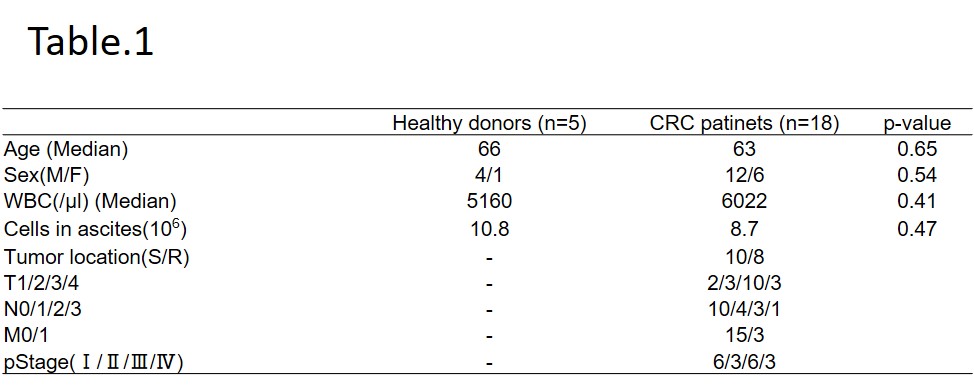
Patients with clinically confirmed CRC or inguinal hernia, diagnosed at our hospital between January 2017 and July 2019, were eligible before inclusion in this study was performed in accordance with the ethical standards of the Committee on Human Experimentation of our institution (Institutional Review Board No.18-257), and we excluded all cases of emergency surgery or multiple cancers. The following factors were compared between the CRC group and the non-CRC group (healthy donors), namely, age, gender, white blood cell counts, cancer stage, and inflammatory cell population in ascites. Ascites was aspirated during laparoscopic surgery using the Opti4 system (Medtronic Inc., Minneapolis, MN, USA). In the absence of ascites in the peritoneal cavity, ascites was diluted with saline.
Flow cytometry
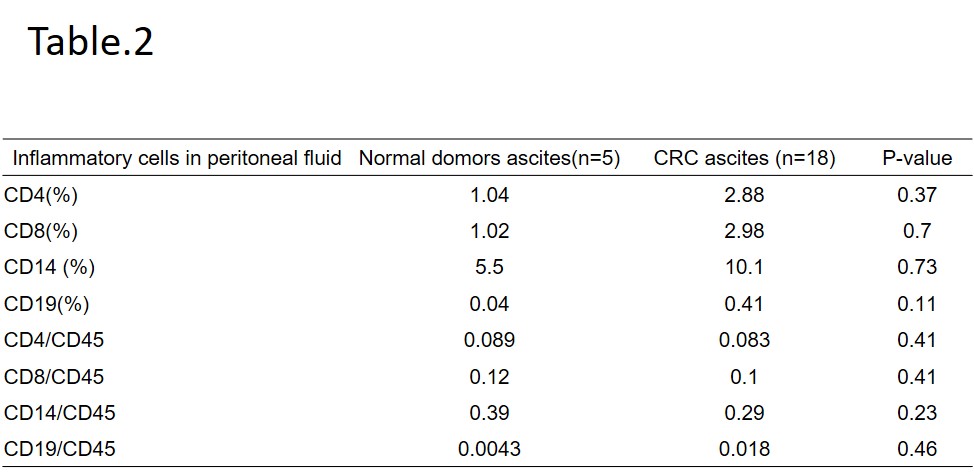
For staining of surface antigens, inflammatory cells were stained with CD4-PE, CD8-FITC, CD14-PE, CD19-APC, and CD45-PerCP (all from TONBO). Viability was determined via DAPI staining (Vector Laboratories). Flow cytometric analyses were performed on a Fluorescence activated cell sorting (FACS) Verse (BD, Immunocytometry Systems, San Jose, CA). For data analysis, we used CellQuestPro (BD/Pharmingen), and FlowJo (Tree Star, Ashland, OR). CD45 positive and CD14 positive cells were sorted by a FACS Aria III (BD Biosciences).
After surgical resection of the CRC, all specimens were histopathologically reviewed, and the pathological classification and stage determined according to the TNM staging system.
Quantification of Cytokine mRNA Expression in CD14 cells by Reverse- Transcription Polymerase Chain Reaction.
Quantitative Real-Time PCR was performed using SYBR Green PCR Master Mix (Toyobo, Osaka, Japan) on a 7500 Fast Real-Time PCR System (Thermo Fisher Scientific, Waltham, MA, USA). Relative mRNA expression was calculated using the 2―ΔΔCT method. The primers used were as follows: ACTB: 5'-AGAGCTACGAGCTGCCTGAC-3'and 5'-AGCACTGTGTTGGCGTACAG-3'; TGFB1: 5'-GGCCTTTCCTGCTTCTCATGG-3'and 5'-CCTTGCTGTACTGCGTGTCC-3'; IL-10: 5'-GCCTAACATGCTTCGAGATC-3'and 5'-TGATGTCTGGGTCTTGGTTC-3'; ARG1: 5'-GGCAAGGTGATGGAAGAAAC-3'and 5'-AGTCCGAAACAAGCCAAGGT-3'; TNF-α: 5'-CAGAGGGAAGAGTTCCCCAG-3' and 5'-CCTTGGTCTGGTAGGAGACG-3';
CCR2: 5'-GACCAGGAAAGAATGTGAAAGTGA-3'and 5'-GCTCTGCCAATTGACTTTCCTT-3'; iNOS: 5'-GTTCTCAAGGCACAGGTCTC-3'and 5'-GCAGGTCACTTATGTCACTTATC-3'
Transwell co-cultures
Co-cultures using 0.4μ cell culture inserts (Nunc, Thermo Fisher Scientific, Waltham, MA, USA) were performed in RPMI-1640 (Wako Pure Chemicals, Tokyo, Japan) supplemented with 10% Fatal Bovine Serum (Biosera, Chile) and 1% Penicillin-Streptomycin Solution (Wako Pure Chemicals, Tokyo, Japan) . CD14+ macrophages and HCT 116 cells were co-cultured as follows. HCT 116 cells were seeded at a density of 104 cells in the bottom of the plate while CD 14+ cells from PB of healthy donors or CRC patients with or without TNF-α antibody treatment (1.5ng/ml; R&D Systems, Minneapolis, MN) were added to the culture inserts. The cells were cultured for 48 hours, after which cell numbers were enumerated by imaging on a BZ-X700 microscope (KEYENCE, Osaka, Japan).
Immunohistochemistry
Colon cancer tissues were snap-frozen in liquid nitrogen, cut into 5-μm sections, and labeled with anti-CD14-PE primary antibody (TONBO). Nuclei were stained using DAPI (Vector Laboratories).
Statistical analyses
Categorical variables were compared using the chi-square test or Fisher's exact test, as appropriate. Continuous variables are presented as median values and were compared using the Mann-Whitney U-test. Data were analyzed using JMP 10 software (SAS, Cary, NC, USA).
{kind=link}
{kind=link}