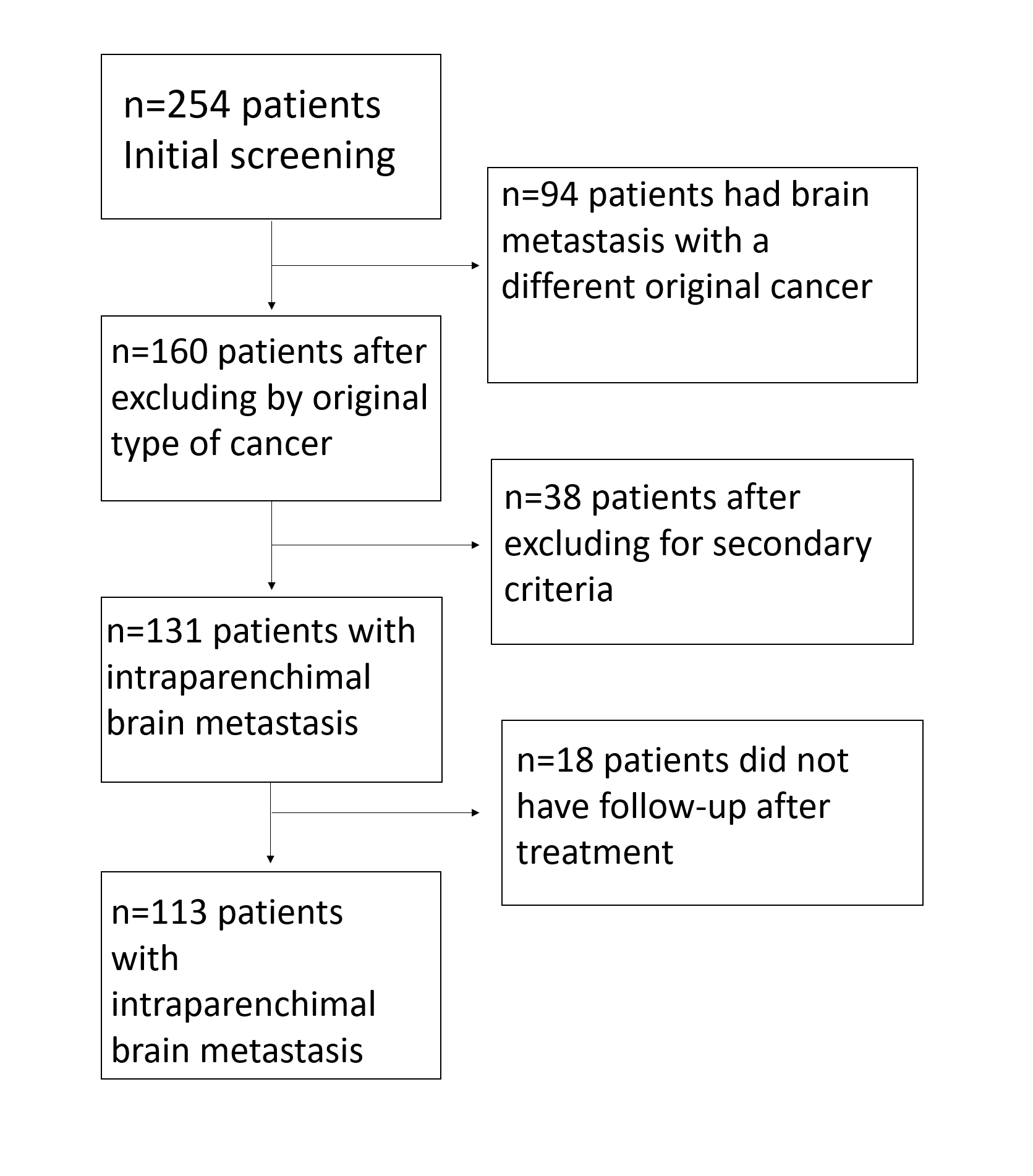
After excluding patients that did not meet our selection criteria, our sample comprised 113 female patients, the mean age of presentation of breast cancer was 53.5 (±11.27). The median interval to brain metastasis in our sample was 4.87 (IQR 2.8-11.2). Sixty-six patients (58.4%) had a breast cancer onset after 50 years. There were seventy-six patients (67.3%) with smoking history, twenty-four patients (21.2%) were African-American, eight patients were Asian (7.1%), and five (4.4%) had other ethnicities (Hispanic and Arab American). The most common type of breast cancer was invasive ductal in eighty-two patients (79.6%), followed by invasive lobular (16.5%), and four patients had other types of histology (3.9%). Most of the tumors in our sample were ER+ (73.2%), while thirty-five cases (31.3%) were HER2 positive. Breast cancer tumors were ER+/HER2- in fifty-eight patients (51.8%), ER-/HER2- in twenty-one (18.8%), ER+/HER2+ in twenty patients (17.9%), and ER-/HER2+ in thirteen patients (11.6%). In the subgroup of patients with ER+ status, forty-one patients received adjuvant endocrine therapy (48.8%), and fourteen received Palbociclib (16.7%).
Initial stage characteristics are outlined in table 1. Forty-four patients had visceral metastasis (38.9%), thirty-three had a distant lymph node metastasis (29.2%), twenty-eight had bone metastasis (24.8%), and twenty-five had vertebral metastasis (22.1%) before having intracranial disease. Sixty-eight patients (63.6%) had a low KPS (<70) during the initial BM diagnosis. Thirty-one patients underwent surgical resection as first-line treatment (27.4%), twenty-nine (25.7%) stereotactic radiosurgery (SRS), and fifty-three (46.9%) WBRT. Median time to last follow-up was 12.6 months (IQR 4.4-30.6).
Onset time to brain metastasis
Median time to brain metastasis was 53.8 months (IQR 32.2-96-1). In univariate analysis post-menopausal state at initial breast cancer diagnosis (HR=1.49; CI 1.02-2.21, P=0.04), HER2+ status (HR=2.19; CI 1.26-3.82, P=0.01), the subtypes ER-/HER2+ (Figure 1.A; HR=2.21; CI 1.22-4.01, P=0.01), and ER+/HER2+ (Figure 1.A, HR=2.14; CI 1.25-3.65, P=0.01), Hispanics and other ethnicities (Figure 1.B; HR=2.40; CI 1.02-5.63, P=0.04) had a shorter interval to brain metastasis from initial diagnosis. In multivariate analysis, post-menopausal state (HR=1.69; CI 1.13-2.53, P=0.01), Asian ethnicity (HR=2.30; CI 1.03-5.16, P=0.043), and the subtype ER+/HER2+ (HR=2.06; CI 1.14-3.71, P=0.016) had a shorter interval time. Factors associated with onset time to BM are summarized in table 2.
Subgroup analysis of the patients with ER+ status showed that patients with an initial Stage IV at diagnosis (HR=1.83; CI 1.1-3.18, P=0.03) and HER2+ tumors (HR=1.81; CI 1.09-2.96, P=0.02) had shorter intervals to brain metastasis. Patients that underwent adjuvant endocrine therapy (Figure 1.C; HR=0.61; CI 0.39-0.95, P=0.03) and palbociclib therapy (Figure 1.D; HR=0.51; CI 0.28-0.96, P=0.04) had longer onset time to brain metastasis. In multivariate analysis, high initial stage (HR=2.09; CI 1.16-3.76, P=0.014), Hispanic and other ethnicities (HR=3.63; CI 1.34-9.81, P=0.011) remained associated with a shorter time to onset. This subgroup analysis can be found in supplementary table.
Survival analysis
In the univariable Cox proportional hazard analysis, we found significantly worse OS in patients with initial lymph node positive status (HR=2.1; CI 1.01-4.3, P=0.041), vertebral metastasis (Figure 2A; HR=2.01; CI 1.01-4.28, P=0.046) and WBRT as initial treatment (Figure 2B; HR=2.7; CI 1.11-6.5, P=0.03). Patients with an early diagnosis (<2 years) of BM had improved survival (Figure 2C; HR=0.24; CI 0.074-0.83, P=0.025). In the multivariable analysis patients with an early diagnosis of BM<2 years remained statistically significant for improved survival (HR=0.22; CI 0.049-0.98, P=0.048). These results are displayed in Table 3.
{kind=link}