We received 90 responses, among responders Gynecological oncologists were 61 (67.78%); followed by Gynecologists 11 (12.22%); then Surgical Oncologists 10 (11.11%); and finally Medical Oncologists and Radiation Oncologists 4 responders each (4.44%). Half of the responders 45(50%) were from the academic hospital; followed by the cancer centre 28 (31.11%); then private hospitals with 14(15.56%) and 3(3.33%) from local or regional hospitals. 44 (48.89%) of responders were consultants with experience of ten years or more; while 21 (23.33%) were consultants with below ten years of experience; and 17 (18.89%) were residents and 8 (8.89%) were fellows.
The majority of responders 45 (75%) told to have institutional or national guidelines, rest 15 (25%) were told to follow international guidelines. 60% responder expressed about the lack of scientific evidence among guidelines. Responders were equally distributed when asked about the general management of gynecological cancer patients requiring surgery, as follows: Cancellation of most oncologic surgeries; Starting or prolonging the neo-adjuvant therapy; Surgical treatment in COVID-free centers and Surgical treatment delayed but already scheduled within next 3 months for all patients.
58% of responders’ institute has managed to install ‘tele-consultation’ services, while 16% told to have facility under process for the same. 44% of responders were told to have new cases based on institutional guidelines, 35% were seeing new cases but deferring assessment till lockdown is in effect and 21% were told to not have any new patients. 65% of responders were comfortable postponing definitive management of CIN-3 by 3 months, another 30% are still able to provide standard management.
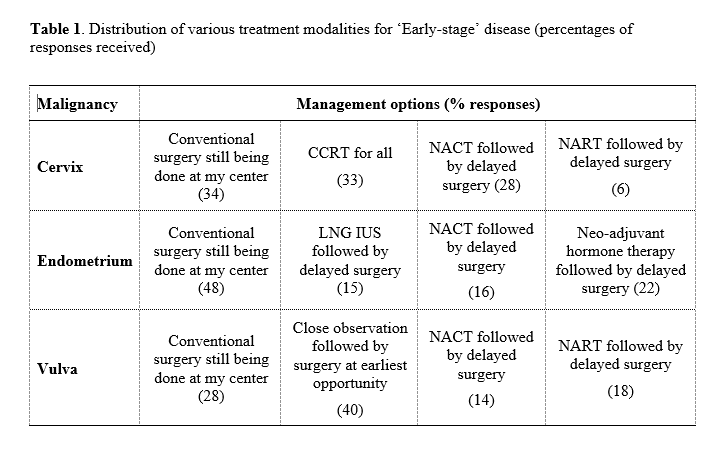
Early-stage cervical cancer: 34% of responders were able to continue with standard surgical management, 33% were offering chemo-radiation for all cases, rest were following less common options like neoadjuvant chemotherapy or radiotherapy. (Table 1)
Early-stage endometrial cancer: Almost half of the responders (48%) were continuing standard surgery, rest were offering neoadjuvant hormonal therapy (37% overall) or neoadjuvant chemotherapy followed by delayed surgery. (Table 1)
Early-stage vulvar cancer: 40% were observing these patients closely, 28% were continuing to offer standard surgery and rest (32%) were offering neoadjuvant options with chemo or radiotherapy. (Table 1)
The majority of responders (83-92%) were continuing treating advanced stage gynecological cancers, though most of them have ‘modified’ standard management as per institutional protocols. (Figure 1)
80% of responders felt strongly about ‘cessation of elective benign surgeries’ and 70% for ‘cessation of elective cancer surgeries’. 68% of responders were not in favor of postponing delaying diagnostic services for ‘new’ patients. 82% strongly supported delaying or modifying standard ‘follow-up protocols’ of gynecological cancer patients.
71% responders felt that elective benign surgeries should be postponed ‘as long as necessary’ to shift resources for COVID care. However, only 37% felt a delay of 2 weeks is acceptable for elective cancer surgeries and another 36% felt these surgeries could be delayed for 6 weeks. 52% felt the diagnosis of new patients could be delayed up to 2 weeks and 27% felt a delay of 6 weeks was acceptable.
Most responders have modified ‘follow up’ protocols, mostly with a ‘less frequent’ follow up approach. Patients with more than 5 years of disease-free survival were not being seen presently by 54% of responders. (Figure 2)
75% of responders feel that full personal protection equipment (PPE) should be used only by those health care workers (HCW) who are managing suspected or confirmed COVID-19 patients. Another 22% feel that PPE should be used by all HCW in the current scenario. 92% responders believe that a combination of social distancing, face mask (any type) and hand hygiene are effective means to contain the pandemic.
83% of responders felt that it will take 3-6 months for socio-cultural life to get back to normal. 37% felt about get back to standard cancer care in 6 weeks. Whereas 43% felt about required duration of 3 months to do so. 30% believed to resume surgical practice will start in 6 weeks, whereas 47% believed 3 months for the same. 68% believe that it will take 6 months or longer for surgical or scientific meetings to restart.
95% responders felt strongly that ‘cancellation of large scientific meets and sports events’ are effective means to contain the viral spread. 95% felt the same for ‘closing of borders and prohibition of travel’. 93% strongly support the ‘lockdown of social and economic life’. Another 96% strongly support ‘active contact tracing of possible infected persons’ as a containment measure. 91% feel that there should be some penal action against those who dissent/desert above containment measures. 86% were comfortable with the cancellation of large public events ‘as long as necessary’. 91% were comfortable with the prohibition on traveling and closure of borders for 3 months to ‘as long as necessary’. 88% of responders were comfortable with the closure of schools and universities for 3 months or longer. 52% feel that social and economic lockdown should continue as long as needed, another 24% were comfortable with the lockdown extending for 3 months. 84% felt that contact tracing of likely infected people should continue for 3 months or as long as needed.
Only 3% of responders told to have operated confirmed COVID case yet, while another 4% were awaiting results of the test by the time of survey. 22% of responders had taken Hydoxy-chloroquine (HCQ) prophylaxis at the time of answering the survey. 50% wish to take it but were waiting for stronger evidence to emerge for its efficacy, another 12 % wish to take it but were concerned about cardiac toxicity and 16% don’t want to take it at all.
Various alternative learning methods were suggested by responders as depicted in Figure 3. 54% of responders felt that it would be the alternative learning methods were not good enough as there is ‘less opportunity for professional interaction’. 42% were concerned about different geographic time zones during online events. 48% were concerned about acquiring new digital/social media skills to be part of e-learning. And lastly 26% felt that there will less opportunity for networking in e-learning events
{kind=link}