Patient characteristics
A total of 82 patients were included in the study, which comprised 21 ESCC patients in the discovery cohort and 61 pan-cancer patients in the validation cohort, including colorectal cancer (CRC), gastric cancer (GC), hepatocellular carcinoma (HCC), neuroendocrine carcinoma (NEC), and other cancer types. The clinical and treatment characteristics of all participants are shown in Table S1. All patients had regionally advanced or metastatic diseases. Patients with clinical benefit (PR/SD, also designated as disease control) and no benefit (PD) were examined by using imaging examinations according to the Response Evaluation Criteria in Solid Tumors (RECIST) v1.1.
Identification Of Potential Predictive Biomarkers In Escc
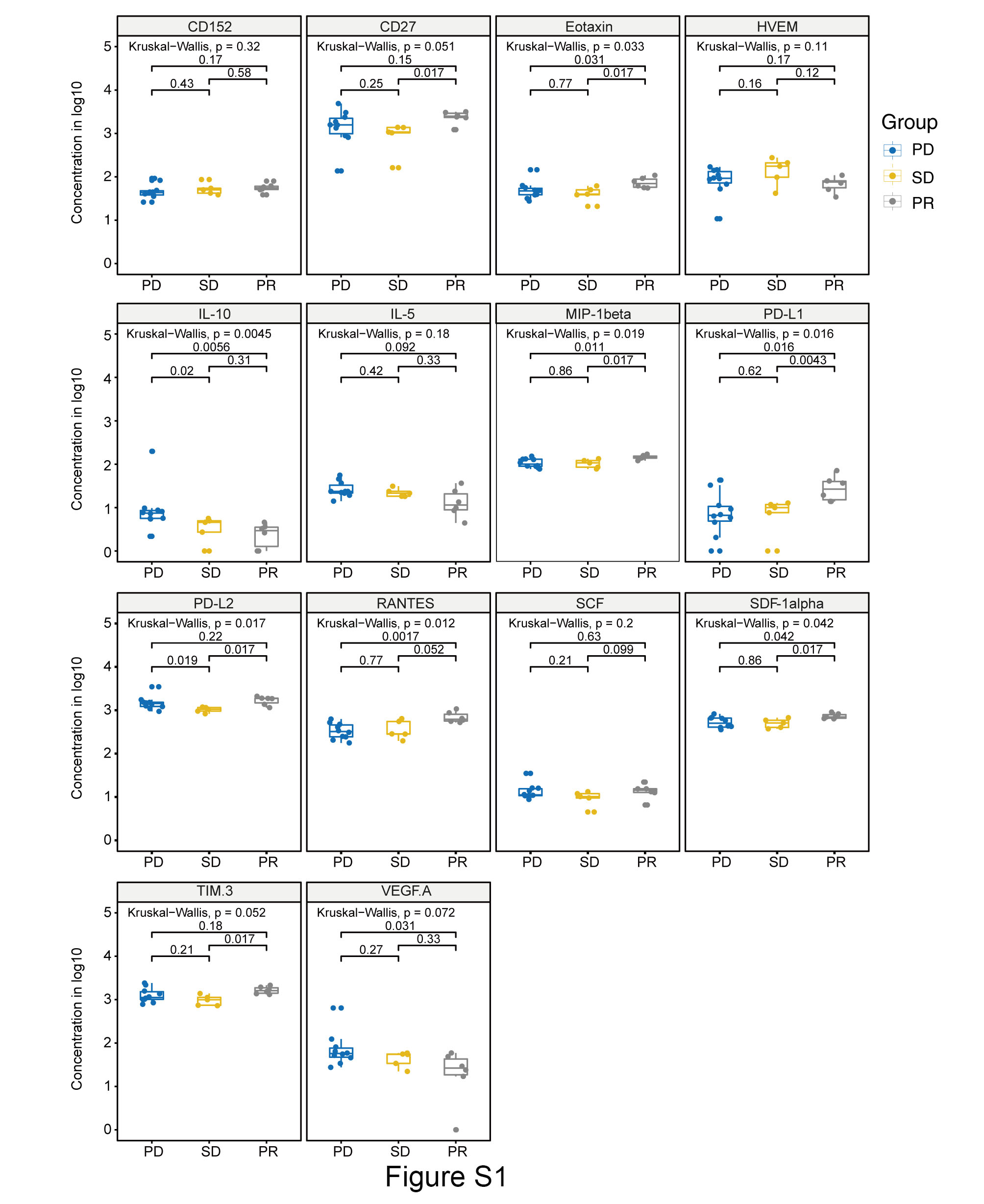
To identify potential systemic biomarkers associated with the immune response, we profiled 59 peripheral immunological factors in a subset of plasma samples from ESCC patients (discovery cohort) by using multiplexed bead immunoassays (Fig. 1A). As Table S2 and Figure S1 reveals, the baseline levels of several cytokines/chemokines/soluble checkpoint molecules were differentially expressed among the PR, SD and PD subgroups (P < 0.05 for a statistical test). Only three immunological factors showed statistical significance by all three tests (Kruskal-Wallis H test for distribution, Jonckheere-Terpstra test for ordered difference, and median test for median differences), indicating the distinct pattern of PD-L1, C-C motif chemokine 5 (CCL5/RANTES), and interleukin 10 (IL-10). Interestingly, in contrast to the decreasing trend of IL10, both PD-L1 and CCL5/RANTES showed a rising trend of therapeutic response across the three groups as PD, SD and PR (Figure S1 and Fig. 1B), indicating a “pro-inflammatory” role of the two factors.
Association between peripheral immune signatures and clinical benefit to ICI treatment in ESCC
Previously, combinatory cytokine signatures have been reported to predict immune-related toxicities [16] and clinical outcomes in cancers [17, 18]. For instance, the expression of a cluster of upregulated cytokines was integrated into a toxicity score, which was associated with the development of immune-related toxicity [16]. Therefore, we tested the predictive and prognostic value of PD-L1, CCL5/RANTES, and their combinatorial signature (mean of log2 transferred value of PD-L1 and CCL5/RANTES) in the discovery cohort. As expected, the increased baseline levels of RANTES, PD-L1 and the “2-cytokine signature”correlated with a higher disease control rate (DCR: PR + SD), with AUC values of 0.818 (95% CI 0.616–1, P = 0.014), 0.750 (95% CI 0.521–0.979, P = 0.053), and 0.755 (95% CI 0.530–0.979, P = 0.049), respectively (Fig. 1C). Accordingly, when using the optimal cutoff value derived from ROC analyses (the Youden index), the peripheral signature-high patients demonstrated a significantly higher DCR than the signature-low subgroup (CCL5/RANTES: 88.9% vs. 16.7%, P < 0.01; PD-L1: 80.0% vs. 18.2%, P < 0.01; 2-cytokine signature: 80.0% vs. 18.2%, P < 0.01; Fig. 1D). Moreover, higher levels of the three signatures were associated with better PFS (CCL5/RANTES: HR, 0.222, log-rank test, P < 0.001; PD-L1: HR, 0.283, log-rank test, P < 0.01; 2-cytokine signature: HR, 0.283, log-rank test, P < 0.01; Fig. 2A). Besides, the associations between signature levels and OS were identical (Fig. 2B) (log-rank test, P < 0.05 for all comparisons).
Validation of the peripheral immune signatures in a pan-cancer cohort
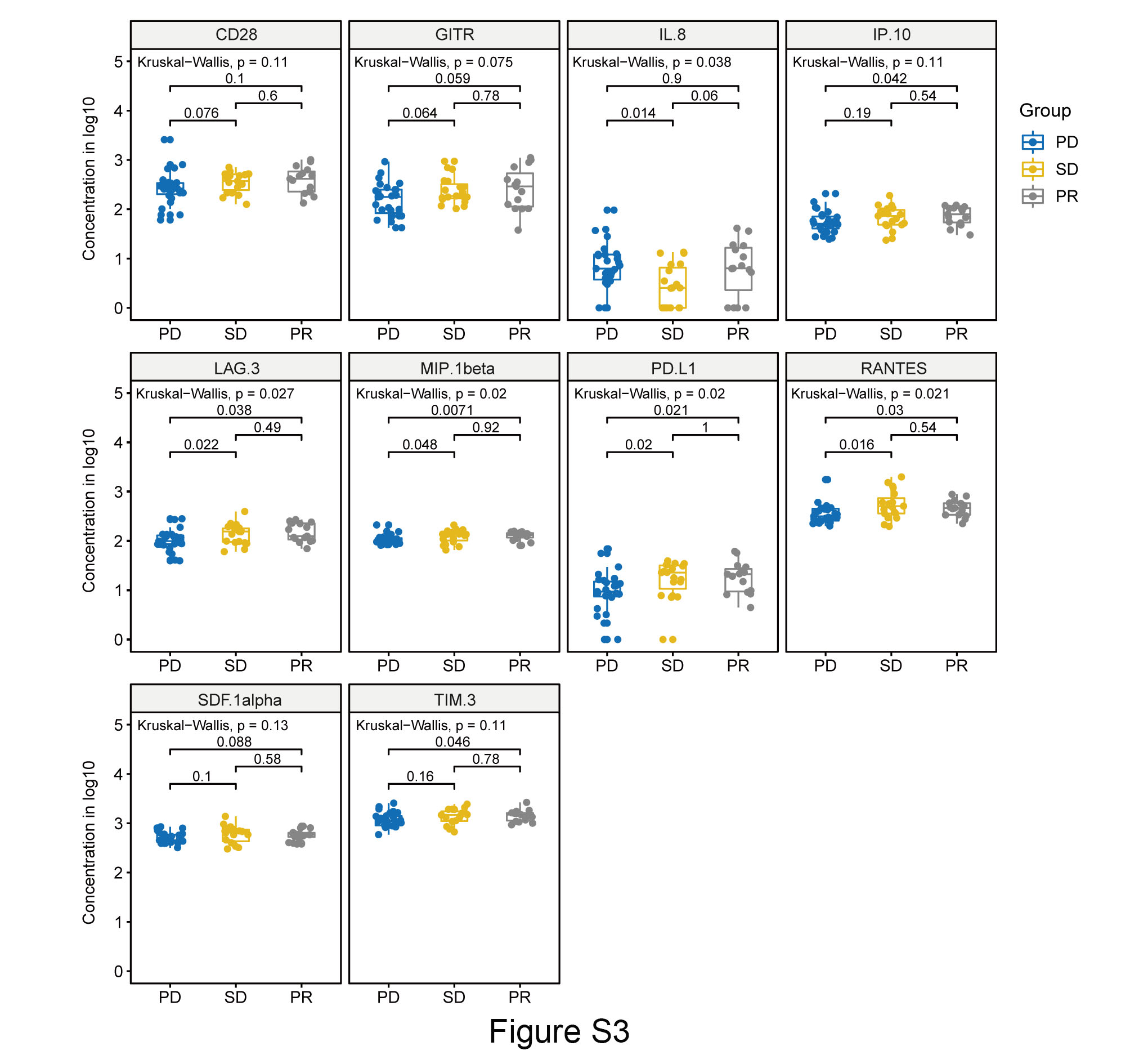
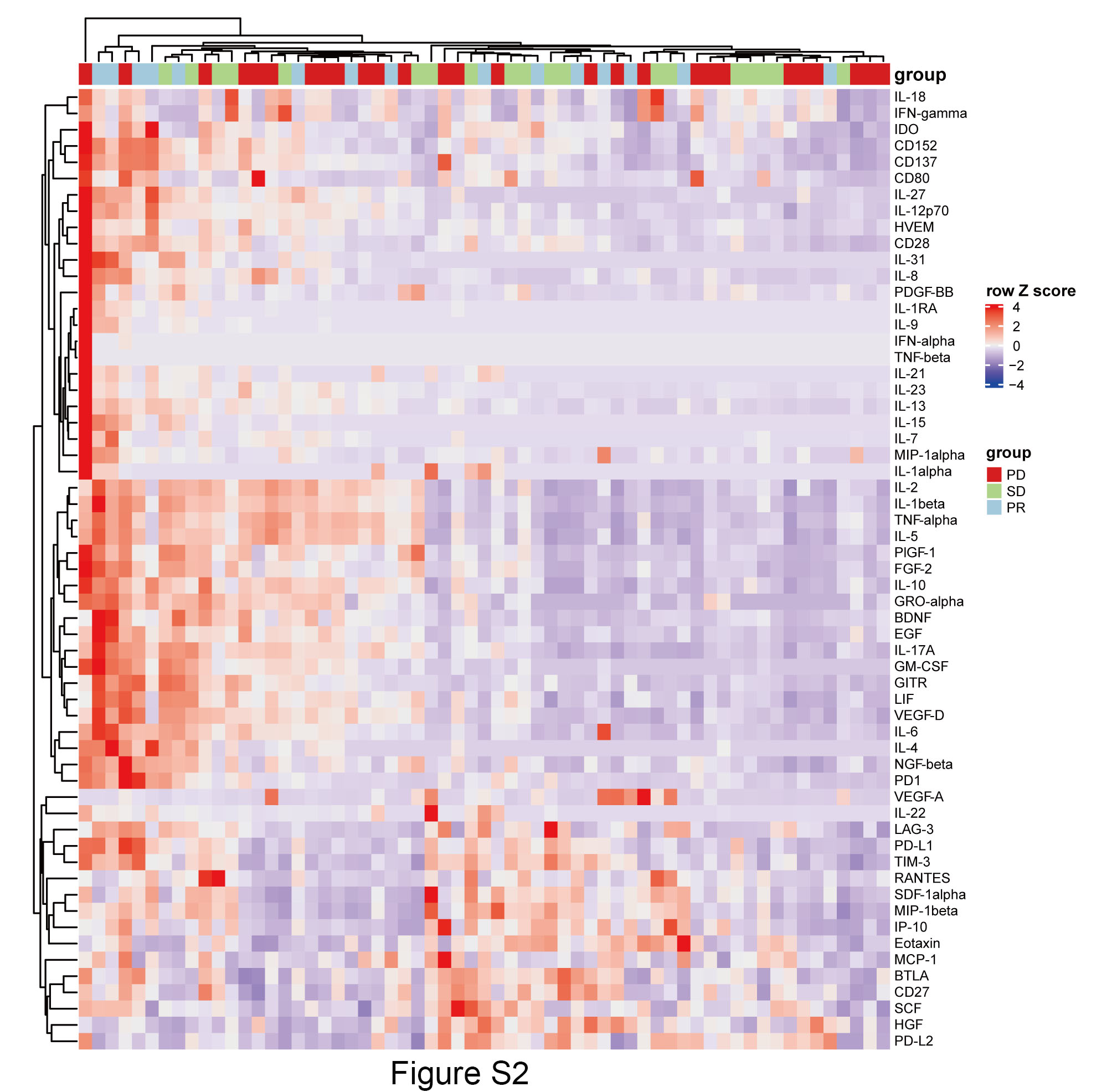
To confirm the predictive and prognostic value of the candidate biomarkers in the peripheral blood samples, we further profiled the expression levels of 59 immunological factors in an independent validation cohort (Table S3 and Figure S2-S3). Not surprisingly, plasma samples in the clinic benefit subgroup displayed higher levels of CCL5/RANTES, PD-L1 and the 2-cytokine signature than those from the no benefit subgroup (P < 0.05) (Fig. 3A). The AUC curves for the three immune signatures were 0.707 (95% CI 0.575–0.839, P = 0.008), 0.710 (95% CI 0.578–0.845, P = 0.005) and 0.722 (95% CI 0.587–0.857, P = 0.003) (Fig. 3B). By using the same stratification cutoff value as in the discovery cohort, higher levels of CCL5/RANTES, PD-L1, and 2-cytokine signature were associated with a higher DCR (P < 0.05 for all comparisons, Fig. 3C). As expected, improved PFS was observed in patients with higher baseline levels of two signatures (CCL5/RANTES: HR, 0.505, log-rank test, P < 0.05; 2-cytokine signature: HR, 0.424, log-rank test, P < 0.01; Fig. 4A). However, only the stratification power of the 2-cytokine signature attained statistical significance for OS (HR, 0.431, log-rank test, P < 0.05; Fig. 4B).
Correlation Between Peripheral Immune Signatures And Tumor Infiltrating Lymphocytes
The above data indicated that CCL5/RANTES and PD-L1 are peripherally correlated with the clinical benefit and prognosis of patients with various cancer types receiving ICI treatment. Cytokines are a broad category of small proteins that allow components of the immune system to communicate with one another to induce a coordinated response [10]. We therefore asked whether different peripheral expression patterns were associated with local immune features in the tumor microenvironment (TME).
In the combined cohort, we obtained only 39 FFPE tissue samples for the mIHC assay (discovery cohort: 13 samples; validation cohort: 26 samples). To determine the correlation between the peripheral and local immune systems, we measured the expression of PD-1/PD-L1 and immune cell infiltration, which includes CD8 + T-cells, CD68 + macrophages (M1), CD68 + CD163 + macrophages (M2) and CD57 + NK cells(Fig. 5A). Intriguingly, in the 2-cytokine signature-high group, we observed enrichment of CD57+, CD57+/PD-L1+, and CD68+/CD163+/PD-L1 + subpopulations in the stromal region and total area when compared to the signature-low group (Fig. 5B). However, no difference was found in CD8 + T-cells between the high- and low- 2-cytokine signature subgroups (data not shown). In addition, we observed no significant difference in infiltrating immune cells and PD-1/PD-L1 expression between the high-RANTES versus low-RANTES or high-PD-L1 versus low-PD-L1 subgroups (data not shown).
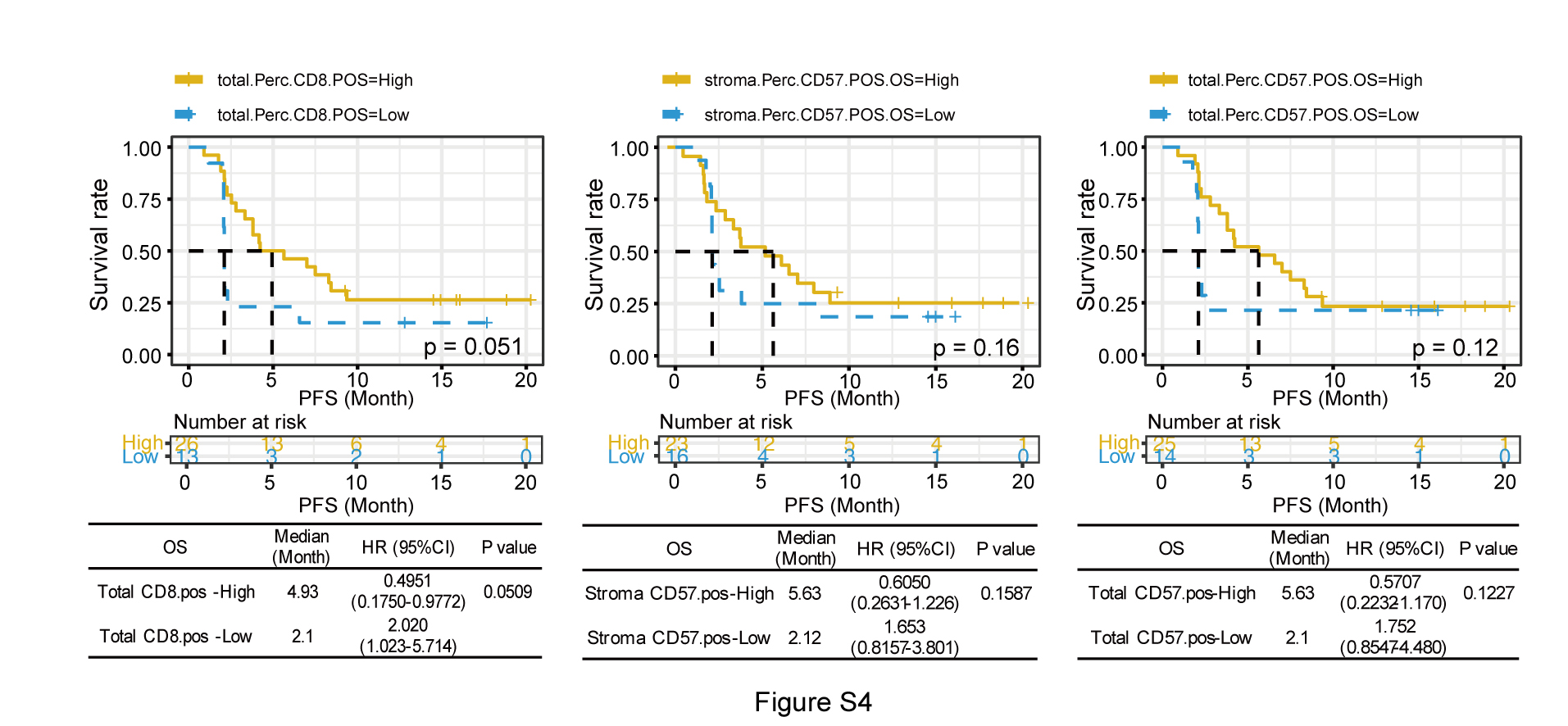
In view of the correlation identified between peripheral and local immune features, we next asked whether the infiltrating immune cells correlated with clinical benefit to immunotherapy. As expected, abundant infiltration of CD8 + T-cells and CD57 + NK cells were local immunological correlates of the DCR (Fig. 6). Specifically, higher percentages of CD8 + T-cells and CD57 + NK cells were observed in the DCR subgroup (Fig. 6A and B). More importantly, the enrichment of these immune cells can stratify patients with longer OS (Fig. 6C). Although improvement of PFS was observed in high-TILs subgroups when compared with low-TILs, statistical significance was not attained (Figure S4). Collectively, our data suggest that higher levels of the predictive peripheral 2-cytokine signature are associated with abundant NK cell infiltration in the TME, which may, in turn, contribute to the better prognosis of patients receiving ICI treatment.
{kind=link}
{kind=link}
{kind=link}
{kind=link}