In this retrospective observational study, we found that the preoperative level of ATIII was associated with postoperative AKI in over 2,300 patients undergoing LT. In multivariate analysis, a 10% increase in preoperative ATIII was associated with 0.86 times decreased risk of post-LT AKI. This association between the preoperative ATIII level and post-LT AKI remained significant only in the low-MELD (< 20) and LDLT subgroups. Additionally, low ATIII was associated with progression to CKD and EAD.
Most previous studies that explored the relationship between ATIII and AKI were performed in animal models; hence, the data in humans are limited [11, 12, 19, 20]. A previous study by Wang et al. demonstrated the predictive value of ATIII level in the development of AKI [11]. The authors concluded that ATIII appears to ameliorate renal ischemia-reperfusion injury by inhibiting the inflammatory response, oxidative stress, apoptosis, and by improving the renal blood flow. The authors also presented human clinical data, which included only 7 patients with low ATIII levels (< 75%), while the majority of patients had normal ATIII levels. Another recent study by Park et al. demonstrated the relationship between preoperative low ATIII level (< 70%) and AKI following LDLT [21]. The authors suggested that the incidence of AKI was 24.8% (143/577) following LDLT, which was much lower than that in our study (67.3%, 1611/2395). This difference in the incidence of AKI might be due to the difference in the study population. In our study, we included DDLT recipients who were at high risk for the development of post-LT AKI. As the patients’ severity increased, the duration of surgery was about 4 hours longer than that in the previous study [21]. A previous study showed that duration of surgery > 10 hours was an independent risk factor for post-LT AKI, which is in line with the finding of our study [22]. In addition, our results showed that the rate of a high amount of transfusion (> 10 units of pRBC) was 26.7%, which is one of the risk factors of AKI.
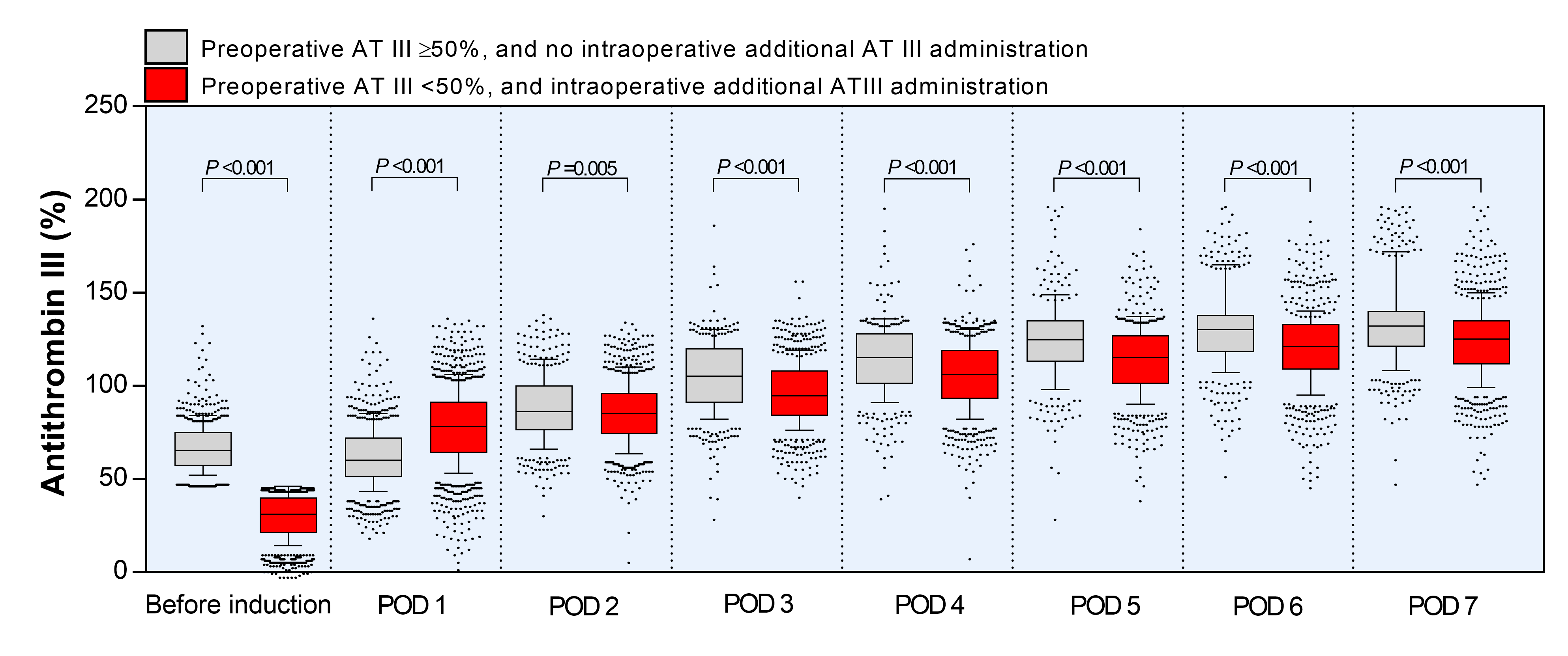
Our center’s protocol of ATIII administration during the perioperative period resulted in a rapid increase of ATIII level. We uniformly administered 2000 units of ATIII daily from POD1 to POD7. Kaneko et al. reported that the ATIII level did not return to normal after LDLT during the first 2 weeks [23]. In a previous study, an initial ATIII level < 50% was reported as the best prognosticator for the prediction of mortality from septic shock [24]. Hence, only patients with preoperative ATIII level < 50% were administered an additional dose of ATIII during the surgery. As a consequence, the average level of ATIII reached the normal level from POD 2 (88.6 ± 18.4% for ATIII ≥ 50% group and 85.9 ± 17.5% for AT III < 50% group). However, on POD7, the ATIII level exceeded the normal (135.1 ± 24.1% in the ATIII ≥ 50% group and 124.2 ± 21.3% for ATIII < 50% group). A protocol with individualized dosage based on the ATIII level might be more cost-effective for maintaining a consistent level of ATIII during the post-LT period.
In our study, low ATIII level, female sex, high BMI, low serum albumin, DDLT, longer duration of surgery, and higher amount of pRBC transfusion were considered as risk factors for the development of post-LT AKI. Similarly, a previous study also reported that female sex, obesity, low serum albumin, DDLT, longer duration of surgery, and higher amount of blood transfusions were associated the development of post-LT AKI [1, 2, 22, 25]. In our study, the MELD score was not a risk factor for post-LT AKI. Since we excluded patients who were previously diagnosed with end-stage renal disease or CKD, the MELD score did not significantly impact the incidence of post-LT AKI. According to our results, preoperative ATIII level as a prognostic factor for predicting AKI remained significant only in the low-MELD group (< 20) and LDLT subgroups but was not statistically significant in the high-MELD group(≥ 20) and DDLT subgroups. Given that the incidence of AKI in the DDLT group was more than 80% in our study, the DDLT group might have multiple factors that might have led to post-LT AKI. Consistent with our findings, other studies also reported that the DDLT group had a higher incidence of post-LT AKI than the LDLT group [25].
In our study, more than 50% of the patients developed post-LT AKI, and a significant proportion of them progressed to CKD after LT surgery. Although most of them were grade I AKI (89.5%, 1442/1611), over one-third of them progressed to CKD (32.3% at 3 months, 37.1% at 6 months, 35.8% at 1 year after LT). Given that the development of AKI and CKD in LT recipients are considered as the important risk factors for post-LT morbidity and mortality [26], strategies to prevent AKI should be implemented in the peri-LT period. In addition, considering the relatively high rate of postoperative AKI in LT surgery compared to that in other non-cardiac surgeries, there is more room for improvement [27].
There are several limitations to this study. First, we could not explain the mechanism of the preventive role of ATIII on the development of post-LT AKI. However, a previous study reported that ATIII insufficiency exacerbates the renal ischemia-reperfusion injury by inflammation, oxidative stress, and apoptosis [11], which are well-known mechanisms associated with the development of AKI. Second, since this was a retrospective study, the confounding factors could not be eliminated entirely. Third, there is no clear evidence regarding the optimal perioperative dose of ATIII to prevent AKI in LT recipients. Although the ATIII level could be normalized during the first two weeks after LT [23], it is necessary to know the target level of ATIII to mitigate the incidence of post-LT AKI. Therefore, further studies are necessary for the individualization of the ATIII dose based on the preoperative ATIII level.

{kind=link}