Drug resistance is a serious cause of therapeutic failures in HCC. In addition to surgical treatment, sorafenib and regorafenib are two critical chemotherapies for patients whose disease progresses toward advanced HCC over a 10-year period or continuously for 3 years[4, 24]. Despite the proven efficacy of sorafenib to significantly increase OS in patients[3], the constantly effective responses for patients are not long appreciated for halting disease progression because advanced HCC often develops resistance to antiproliferative therapies[25]. In the present study, we established two drug-resistant cell lines to further explore the mechanism of sorafenib resistance with the goal of elucidating candidate targets for improving the efficacy of HCC therapy.
The relationship between CSC properties and sorafenib resistance has been predicted and highlighted in recent reports. CSC traits drive tumorigenicity in HCC cells and lead to HCC recurrence and sorafenib resistance[26]. However, SR HCC is causally linked to the maintenance of stem-like properties[27]. Enriched spheres with SR signatures have been related to CSCs, metastasis, and recurrence of HCC[28]. These findings provide us with confidence in defining the correlation between SR cells and CSC traits as well as demonstrate the self-renewal and tumor formation of serially diluted transplanted SR HCC cells.
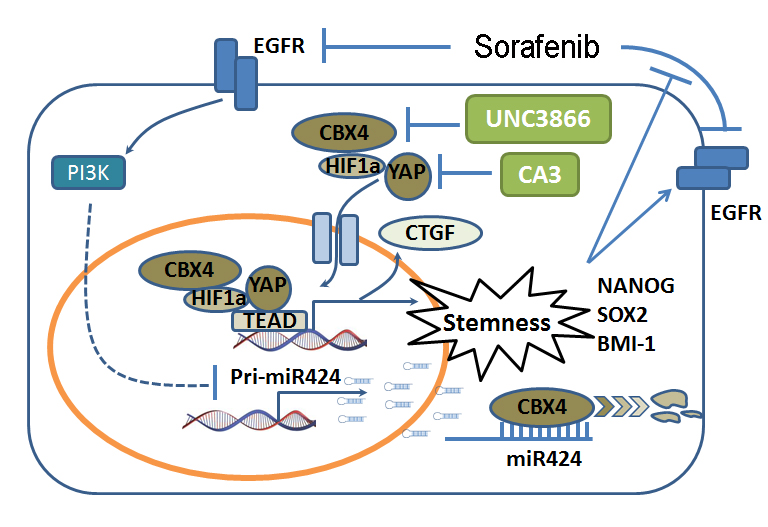
Recent studies have revealed that a series of miRNAs are involved in HCC tumor development. For example, miR367, miR223, miR494, miR221 and miR622 expression levels were increased with sorafenib resistance in HCC cells and associated with different pathways, such as the RAS-ERK pathway, PI3K-AKT pathway, mTOR pathway, etc.[13–15, 29, 30]. However, miR-122 and miR137 expression significantly inhibited SR cells by reducing apoptosis through the AKT/ERK pathway[31] and tumor-initiating cell phenotypes[32]. Although these augmented miRNAs have been characterized to have antiangiogenic, antimetastatic and anti-stem-like functions by targeting many transcription factors in HCC, we definitively identified miR424 as a tumor repressor that targets CBX4 and is associated with poor outcomes in HCC. A previous study revealed that miR424 significantly highlights the stem-cell-like properties of HCC, while the transcription factor PBX3 responds to this activity and modulates tumorigenesis[17]. However, how miR424 is relevant to sorafenib resistance is unknown; thus, in this study, we further explored whether miR424 governs sorafenib resistance by directly targeting CBX4 and activating CBX4-induced tumor formation and self-renewal characteristics. As previously reported, sorafenib could inhibited EGFR activity, and directly affected the downstream PI3K-YAP pathway [33]. Nevertheless, the interaction between PI3K and YAP has not been sufficiently explained. Based on the correlation between PI3K and miR424[34, 35] and this study, we give one explanation of PI3K /YAP interactivity through miR424-CBX4 which was induced by sorafenib resistance. But, the mechanism of how miR424 was regulated by PI3K was needed further understand in the feature.
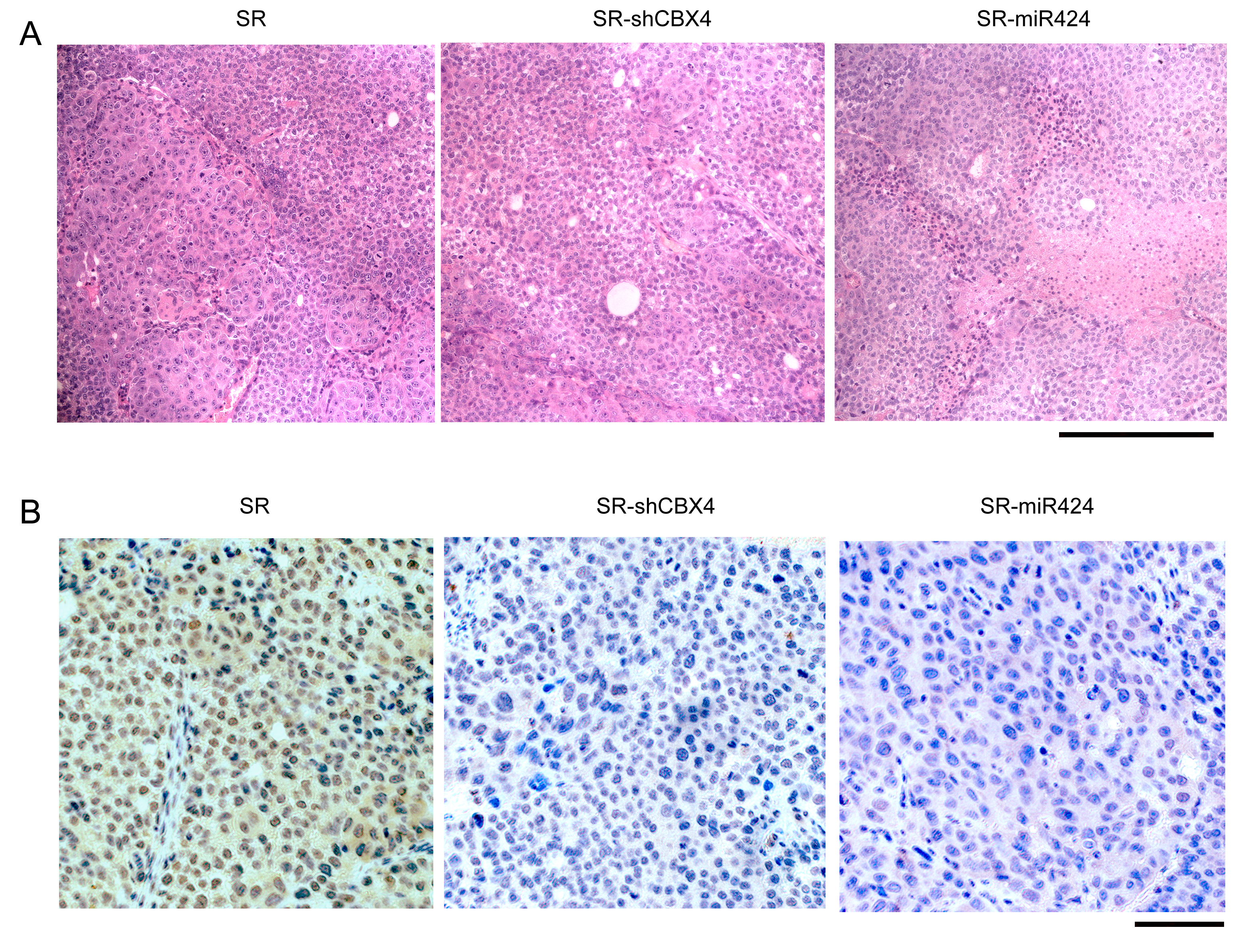
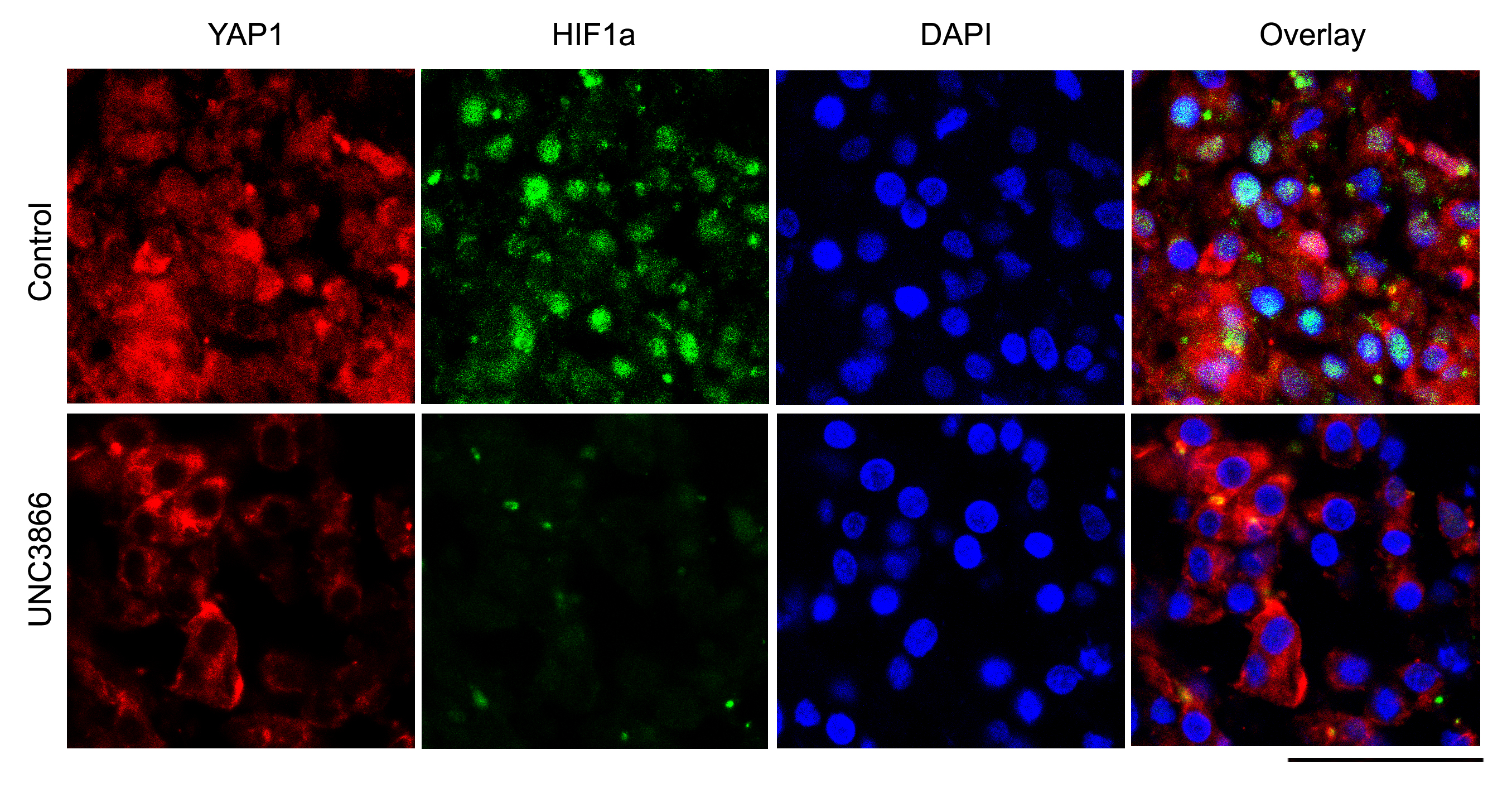
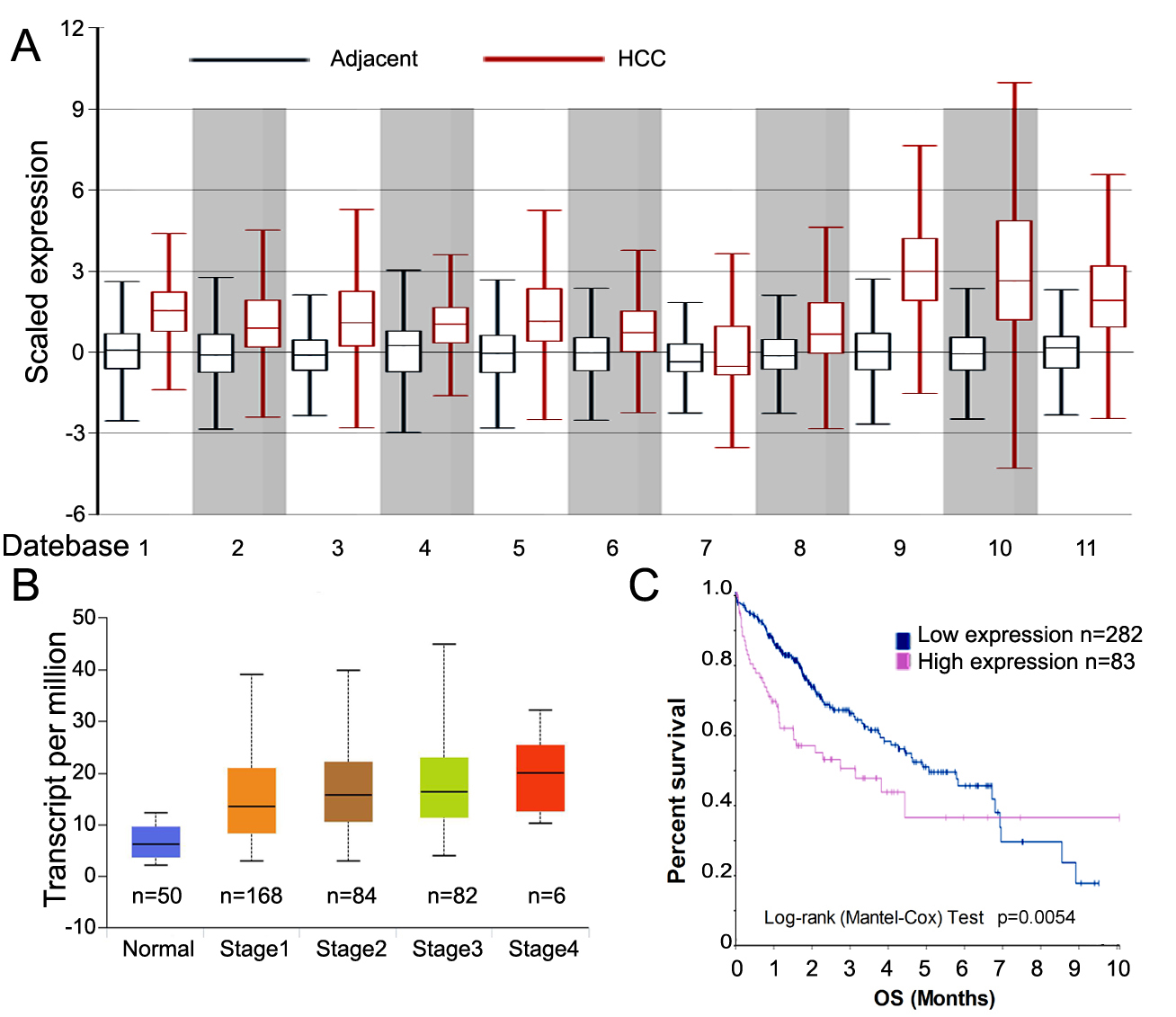
Because we reported that cytoplasmic CBX4 protein levels indicated poor survival for HCC patients who undergo surgical resection[10], CBX4 was followed by analysis of a TCGA dataset and GTEx bioinformatics with 11 public HCC expression datasets that covered approximately 3401 clinical samples (Fig S2 and Table S7)[36]. We clearly confirmed that a high CBX4 level contributes not only to tumorigenesis but also to a more advanced stage of HCC. As a factor of poor prognosis, CBX4 increases the transcriptional activity of HIF-1a and hypoxia-induced VEGF expression in HCC[9]. In addition, CBX4 results in BMI1 recruitment via its E3 sumo ligase activity[37] and has been shown to suspend proliferation and promote terminal differentiation[8]. This differential activity might be influenced by individual characteristics of different organs, as we found that CBX4 drives opposing behaviors in colorectal carcinoma metastasis[38]. In our present study, as a tumor progenitor, CBX4 was shown to induce stem-cell-like properties and promote YAP nuclear translocation in a HIF1a-dependent manner. This outcome is based on the discovery from the KEGG analysis of the sequencing data between CBX4-overexpressing cells and control cells. Thus, exciting results indicate several interesting pathways downstream of CBX4 signaling. For example, Wnt signaling has always enhanced CSC properties[39], Toll-like receptor signaling facilitates stem cell marker expression in HCC[40], and the PI3K-AKT pathway is a canonical signaling pathway downstream of EGFR to reduce tumor-initiating cell frequency[41]. The Hippo-YAP pathway showed the greatest upregulation in response to CBX4 in our results. Although HIF1a and YAP have been widely reported and contribute to CSCs in HCC[42, 43], we actually found that CBX4 regulates YAP signaling through YAP translocation rather than its production in SR HCC, and this mechanism implicates that the CBX4-YAP interaction is an important event for sorafenib resistance and even contributes to HCC therapy as shown in Figure S4.
The mounting evidence suggests that CSCs are particularly resistant to chemotherapy[44], and cells with sorafenib resistance maintain their CSC properties[27]. Our previous findings indicated that YAP1 plays a critical role in CSC self-renewal and tumor formation and that suppressing YAP1 could be an effective way to prevent the maintenance of CSCs[21]. In this study, we propose that targeting the CBX4-YAP1 axis could viable in treating CSCs and might be a novel strategy for SR HCC. Therefore, defining CBX4-YAP mediators of resistance to therapy is critical to better understand the relationship between CSC and sorafenib resistance.
We also investigated the effect of the combination of CBX4 and YAP inhibitors (UNC3866 and CA3) as a therapy for SR cells. Notably, the use of three targeted medicines for treating tumors is not available in the clinic. However, in our study, we provide effective candidates for patients who experience chemotherapy failure but can still benefit from a long-term treatment, even if they develop sorafenib resistance. In our opinion, we suggest three ways to maintain an available strategy for sorafenib resistance: transducing cells with miRNA424, inhibiting CBX4 expression and arresting the Hippo-YAP pathway. We also propose a rational, biomarker-based clinical trial (using CBX4 and YAP1 overexpression to enrich the HCC patient cohort). We would also like to provide empirical therapeutic strategies for reducing sorafenib resistance by conducting in-depth molecular analyses of HCC.
{kind=link}
{kind=link}
{kind=link}
{kind=link}