Composition of the respiratory tract and gut antibiotic resistome in patients with COVID-19
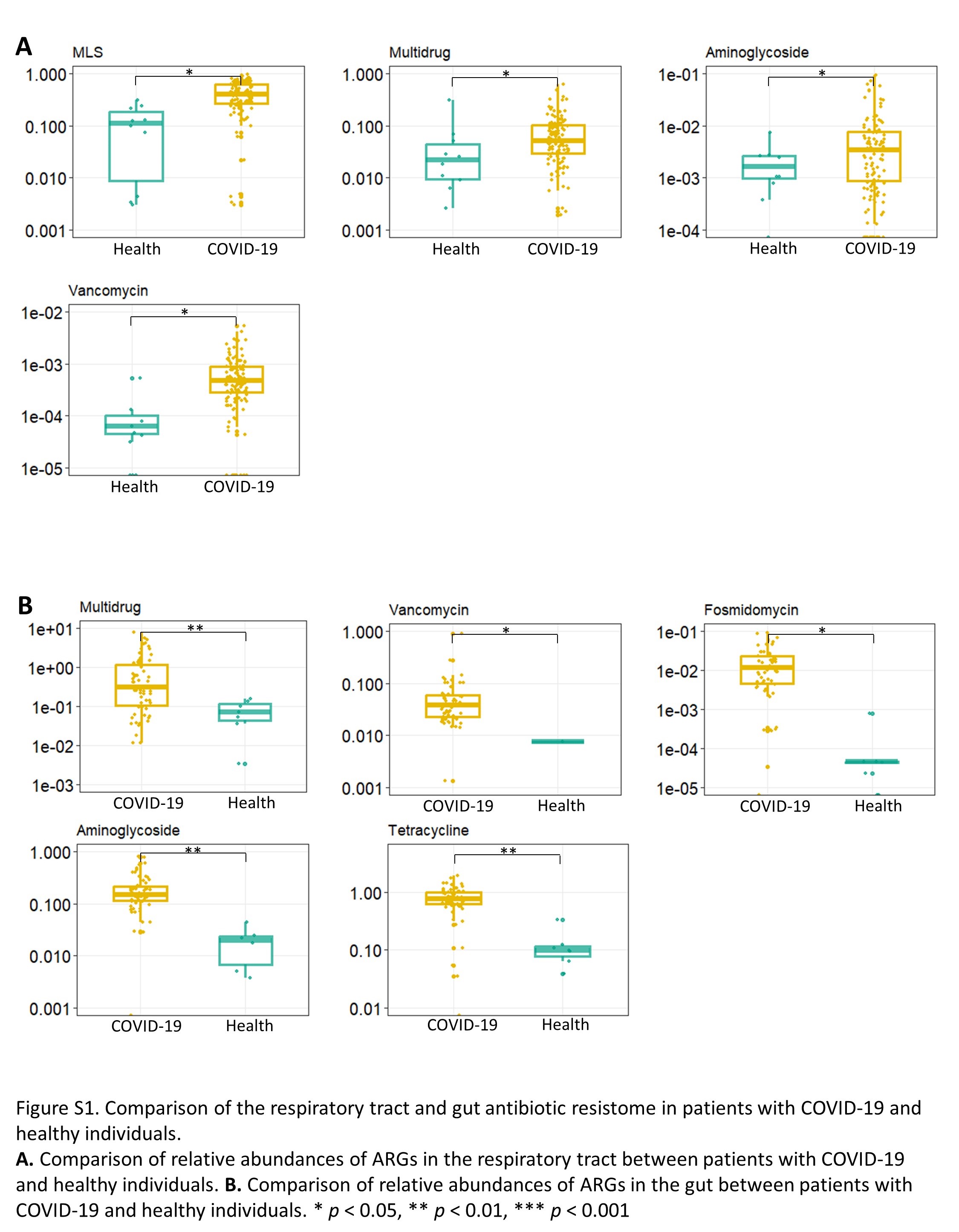
To dissect changes in the ARG composition of COVID-19 patients, we performed metagenome sequencing on 143 sputum and 97 fecal samples in ICU and nICU patients and healthy people. The sputum samples were collected from patients at three disease progression stages (admission, progression, and recovery) whereas the fecal samples were collected at two stages (progression and recovery) for the study (Fig. 1A). We detected a total of 24 ARG types and 1244 ARG subtypes in the total sample population. After excluding unclassified ARG types or subtypes and 10% prevalence filtering, a total of 17 ARG types and 193 ARG subtypes were validated and subsequently analyzed in the current study. The top three most abundant ARG types identified in the respiratory tract are active against Macrolide-lincosamide-streptogramin (MLS), Beta-lactam, and Tetracycline and are present in the both healthy individuals and patients with COVID-19 (Fig. 1B). We found that among the top ten most abundant ARG types in the respiratory tract, the relative abundances of MLS, Vancomycin, Multidrug and Aminoglycoside increased significantly in patients with COVID-19 compared with healthy cohorts (p < 0.05) (Figure S1, Supporting Information). ICU patients had higher relative abundances of Multidrug, Vancomycin and Aminoglycoside ARGs than nICU patients (Fig. 1B). In the gut samples, the top three most abundant ARG types observed are Multidrug, MLS and Tetracycline. We observed that among top ten most abundant ARG types, the relative abundances of Multidrug, Tetracycline, Aminoglycoside, Fosmidomycin and Vancomycin ARGs increased significantly in patients with COVID-19 compared with healthy cohorts (p < 0.05) (Figure S1, Supporting information). ICU patients had higher relative abundances of Multidrug, Vancomycin and Fosmidomycin ARGs than nICU patients (Fig. 1B).
To investigate diversity of respiratory tract and gut antibiotic resistome among patients with COVID-19, we calculated the Shannon index to measure the alpha diversity for each patient. We found that the Shannon index of gut antibiotic resistome is much higher than that of the respiratory tract antibiotic resistome (p < 0.001) (Fig. 1C). We also found that the beta-diversity was significantly higher in the gut antibiotic resistome than in the respiratory tract (p < 0.001) (Fig. 1D). Furthermore, when we compared the beta-diversity of ICU and nICU patients we found that there were significant differences between the ICU and the nICU patients in both the respiratory tract and gut antibiotic resistome (p < 0.01) (Fig. 1E).
Dynamic changes in respiratory tract antibiotic resistome and its association with disease severity
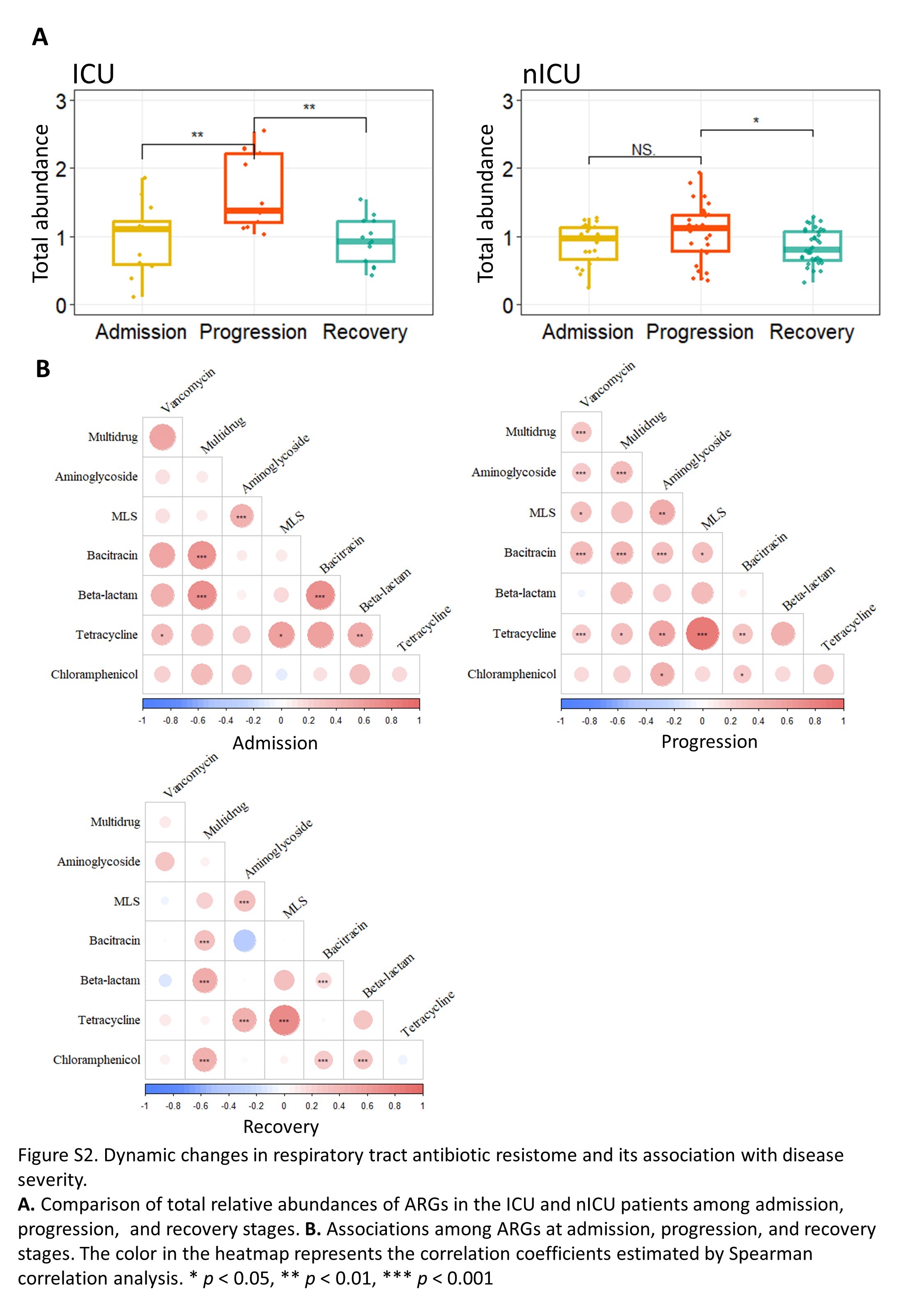
We next examined the relative abundances of ARGs in sputum samples of patients at the admission, progression, and recovery stages to investigate possible dynamic alterations in the respiratory tract antibiotic resistome over the time course of the disease. In the ICU patients, the total relative abundance of ARGs were significantly increased in the progression stage compared to the admission and recovery stages (p < 0.01) (Figure S2, Supporting Information). Moreover, the relative abundances of MLS, Multidrug, Vancomycin and Aminoglycoside ARGs were higher in the progression stage samples compared to samples collected at the admission and recovery stages (Fig. 2A), consistent with our previous findings (Fig. 1B). In nICU patients, the total relative abundance of ARGs were significantly increased in the progression stage compared with the recovery stage (p < 0.05) (Figure S2, Supporting Information). Further comparison of Shannon indices between ICU and nICU patients at different stages indicated that there was a significant difference in antibiotic resistome alpha diversity between ICU and nICU patients at the progression stage (p < 0.05) (Fig. 2B).
To further explore the differences in respiratory tract antibiotic resistome between ICU and nICU patients at different stages of disease progression, we performed multiple linear model regression analyses that included clinical information about patient ICU status, gender, antibiotic usage, age and smoking history. At the admission stage, Kasugamycin, Vancomycin and Aminoglycoside ARGs were significantly positively correlated with ICU status. In contrast, Rifamycin ARGs were negatively correlated with ICU status. Besides, at the admission stage, we found that Rifamycin and Aminoglycoside were positively correlated with antibiotic therapy (p < 0.05) (Fig. 2C). At the progression stage, Multidrug, Bacitracin, Quinolone, Aminoglycoside, Chloramphenicol, Fosfomycin, Sulfonamide, Kasugamycin, Fosmidomycin and Vancomycin ARGs were significantly positively correlated with ICU status (p < 0.05) (Fig. 2C), and we observed that Multidrug and Bleomycin ARGs were positively associated with antibiotic therapy (p < 0.05) (Fig. 2C). At the recovery stage, Sulfonamide, Polymyxin, Fosmidomycin and Multidrug ARGs were significantly positively correlated with ICU status. In addition, we found that at the recovery stage, the relative abundances of Multidrug and Chloramphenicol ARGs were positively correlated with antibiotic therapy (p < 0.05) (Fig. 2C). Based on these results, we found that Kasugamycin, Vancomycin and Aminoglycoside ARGs were significantly positively correlated with ICU status in the admission and progression stages. Besides, the relative abundances of Sulfonamide, Fosmidomycin and Multidrug ARGs were significantly positively correlated with ICU status in the progression and recovery stages. In addition, the results showed that patients’ gender, age, and smoking history did not have a significant influence on the abundance of respiratory tract antibiotic resistome (Fig. 2C).
Next, to investigate the relationships among the ARG types at each stage, we performed a relative abundance correlation analysis (Fig. 2D). Our results showed that MLS and Tetracycline, MLS and Aminoglycoside, Bacitracin and Multidrug ARGs were significantly correlated with each other at all stages (p < 0.05) (Figure S2, Supporting Information). Tetracycline ARGs were significantly positively correlated with Vancomycin ARGs both at the admission and progression stages (p < 0.05) (Figure S2, Supporting Information). To determine the ARG subtypes involved in the observed changes, we compared the relative abundances of subtypes between ICU and nICU patients at the admission, progression, and recovery stages (Fig. 2E). Among the Chloramphenicol types, the relative abundance of Chloramphenicol_cat increased considerably in ICU patients at the progression stage (p < 0.01). In the MLS types, the relative abundance of MLS_macA increased significantly in ICU patients at the recovery stage (p < 0.05). In the Multidrug types, the relative abundances of Multidrug_mdtB, Multidrug_mdtC and Multidrug_mdtK were significantly increased in ICU patients at the progression stage (p < 0.05). In the Vancomycin types, the relative abundance of Vancomycin_vanS was significantly increased in ICU patients at the admission and progression stages (p < 0.05). Thus, the increased relative abundance of certain ARG types, such as Multidrug ARGs was related to alterations in many subtypes, whereas in Chloramphenicol, MLS, and Vancomycin ARGs only one subtype was responsible for the increase in the relative abundance of the types.
Dynamic changes in gut antibiotic resistome of patients with COVID-19 and its association with respiratory tract antibiotic resistome
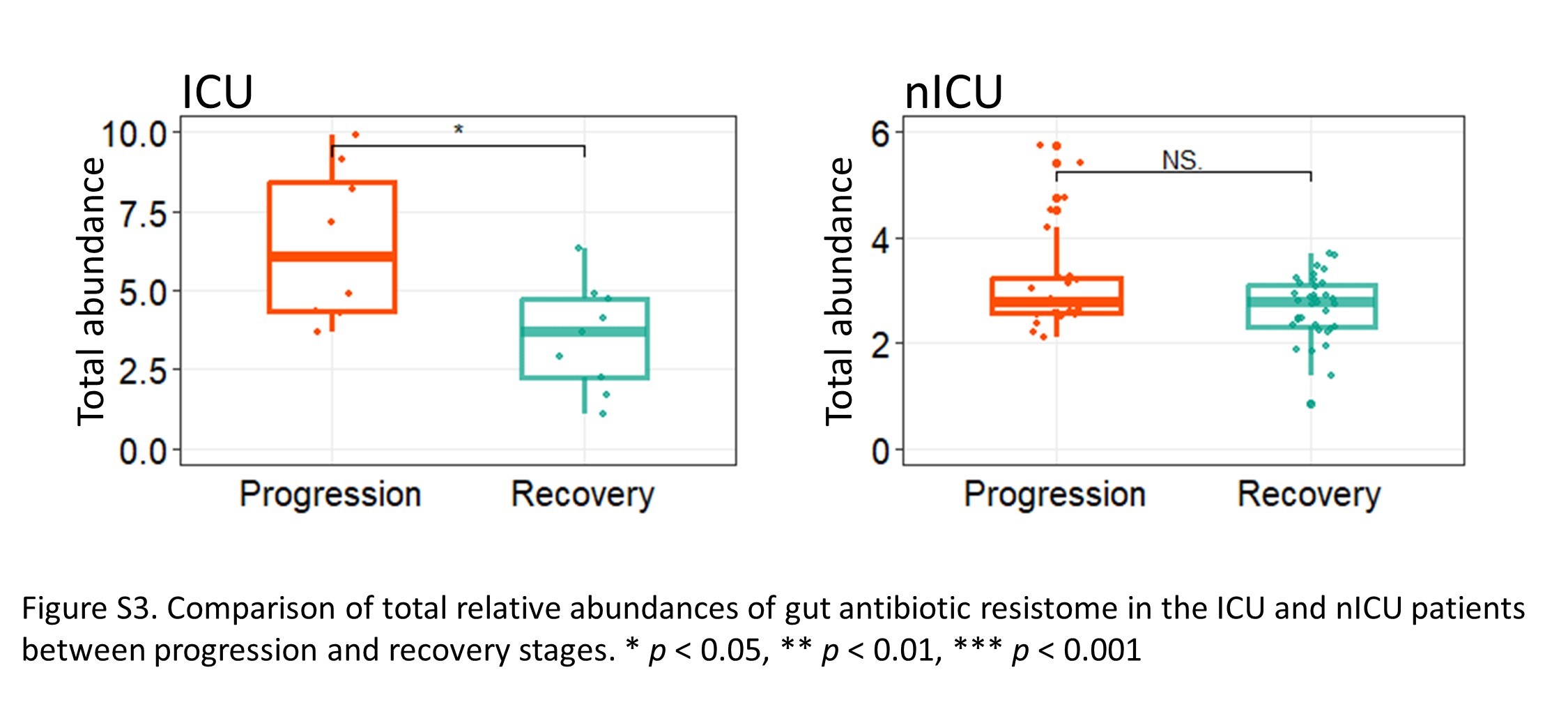
To analyze the dynamic changes in the gut antibiotic resistome, we investigated the relative abundances of the ARG types in the gut during the progression and recovery stages. In ICU patients, the total relative abundance of ARGs was significantly increased in the progression stage compared to the recovery stage (p < 0.05) (Figure S3, Supporting Information). Moreover, the relative abundances of Multidrug and Fosmidomycin ARGs were higher in the progression stage than in the recovery stage (Fig. 3A). In nICU patients, no significant difference in the total relative abundance of ARGs was observed among samples collected at progression and recovery stages (Figure S3, Supporting Information).
To further understand the differences in gut antibiotic resistome between the ICU and nICU patients at different disease stages, we also performed a multiple linear model regression analysis that included information about patient ICU status, gender, antibiotic usage, age and smoking history. In the progression stage samples, we found that Multidrug, Bacitracin, Fosmidomycin, Polymyxin, Kasugamycin, Aminoglycoside, Vancomycin and Fosfomycin ARGs were significantly positively correlated with ICU status (p < 0.05). At the progression stage, we also observed that Fosmidomycin, Beta-lactam and Quinolone ARGs were positively correlated with antibiotic therapy (p < 0.05) (Fig. 3B). In the recovery stage, Vancomycin, Aminoglycoside and Multidrug ARGs were found to be significantly positive correlated with ICU status (p < 0.05). In addition, at the recovery stage, we observed that Beta-lactam and Chloramphenicol ARGs were positively correlated with antibiotic therapy (p < 0.05) (Fig. 3B). Based on these findings, we concluded that Vancomycin, Multidrug and Aminoglycoside ARGs were positively correlated with ICU status in both the progression and recovery stages, and Beta-lactam ARGs were positively correlated with antibiotic therapy in both the progression and recovery stages.
Next, we compared the relative abundance of ARG subtypes between ICU and nICU patients at the progression and recovery stages to determine which ARG subtype contributed the most to the alterations in the gut antibiotic resistome (Fig. 3C). In the Multidrug type ARGs, the relative abundance of Multidrug_mdtN and Multidrug_mexE subtypes were significantly increased in ICU patients at the progression stage (p < 0.05). In the Aminoglycoside type the relative abundance of Aminoglycoside_aph-3I was significantly increased in ICU patients at the progression stage (p < 0.05). In the Vancomycin type the relative abundance of Vancomycin_vanY was significantly increased in ICU patients at the progression stage (p < 0.01). In the Fosmidomycin type the relative abundance of Fosmidomycin_rosB and Fosmidomycin_rosA subtypes were significantly increased in ICU patients at the progression stage (p < 0.05). Based on these results, we suggested that the increased relative abundance of the Multidrug and Fosmidomycin ARGs could be attributed to multiple subtypes, whereas in ARG types such as Vancomycin and Aminoglycoside, only one subtype was responsible for the increased relative abundance.
To investigate the relationship between the antibiotic resistome of the respiratory tract and the gut, we conducted a correlation analysis based on the relative abundances of each ARG type. A significant positive correlation was revealed between the relative abundances of Aminoglycoside, Kasugamycin and Tetracycline ARGs in the respiratory tract and the gut (Fig. 3D). In addition, we found that the Multidrug type was significantly increased in the ICU patients in both the gut and respiratory tract (Fig. 6A). The relative abundance of Multidrug ARGs in the respiratory tract was significantly lower than that in the gut (Fig. 1B). Based on samples in which Multidrug ARGs were detected, a significant (p < 0.01) correlation was found between Multidrug ARGs in the respiratory tract and gut (Fig. 3E).
Relationship between respiratory tract, gut antibiotic resistome composition and clinical indexes
We compared clinical indices in the ICU and nICU patients and found that the number of WBC was significant higher in the ICU patients than the nICU patients (p < 0.05). In contrast, HCT levels were significantly higher in the nICU patients (p < 0.05) (Fig. 4A). Both of these observations are consistent with results from previous studies 25–27. We further conducted Spearman correlation analysis between clinical indices and the relative abundances of ARG subtypes, to explore the relationships between the clinical indices and respiratory tract, gut antibiotic resistome of patients with COVID-19 (Fig. 4B, C). In the respiratory tract, we found that IL-6 was positively correlated with the subtypes of Multidrug ARGs (p < 0.05), and PCT level, WBC and Neutrophil numbers were significantly positively correlated with the relative abundance of ARG subtype MLS_macA (p < 0.01), which was increased in the ICU patients at the recovery stage (Fig. 2E). However, the Hb and HCT levels were significantly negatively correlated with the abundance of Chloramphenicol_cat and subtypes of Multidrug ARGs (p < 0.05), whereas the abundance of Tetracycline_tetO was positively correlated with the Hb and HCT levels (p < 0.05). The IFN-γlevel was positively correlated with the abundance of Bacitracin_bcrA and Tetracycline_tetO subtypes (p < 0.05) (Fig. 4B). In the gut, PCT level was significantly positively correlated with the abundance of ARG subtypes Multidrug_mexE and Vancomycin_vanY (p < 0.001), both of which are higher in ICU patients at the progression stage (Fig. 3C). IL-6 level was positively correlated with the abundance of many subtypes of Multidrug ARGs (p < 0.05). Moreover, WBC and Neutrophil numbers were positively correlated with the abundance of Vancomycin_vanY (p < 0.001), whereas the Hb and HCT level were negatively correlated with the abundance of ARG subtypes Aminoglycoside_aph3I and Vancomycin_vanY (p < 0.05).
Co-occurrence patterns among disease severity related ARGs and microbial species in respiratory tract and gut
To investigate if there was a co-occurrence pattern between the disease severity related ARGs and microbiota in the respiratory tract and gut, we conducted a correlation analysis based on the relative abundance of ARG subtypes and microbiota composition at the genus and species level. In the respiratory tract, at genus level, we found that the relative abundance of Multidrug_mdtB ARGs was positively associated with Lautropia (Fig. 5A). Genera associated with pathogenicity, like Lautropia, in conditions of immune exhaustion were predominant in patients with severe infection 28. At the species level, we found that Multidrug_mdtB ARGs were positively associated with Klebsiella pneumoniae, which accounts for a higher proportion of hospital-acquired pneumonia (Fig. 5C). Moreover, we found that subtypes of Multidrug ARGs were positively associated with Pseudomonas aeruginosa, which can cause infections in the blood or other parts of the body after surgery (Fig. 5C). A prior study showed that patients with severe COVID-19 requiring ECMO had a very high rate of late-onset ventilator-associated pneumonia frequently caused by P. aeruginosa29. This observationis consistent with our findings that the relative abundance of Multidrug ARGs is associated with disease severity (Fig. 2A). We also observed that subtypes of Aminoglycoside and Chloramphenicol_cat ARGs were positively correlated with Candida albicans, a main cause of invasive fungal infections in critical care settings (Fig. 5C). A prior study suggested a high prevalence of systemic candidiasis in severe COVID-19-associated pneumonia patients 30, which is consistent with our findings that the relative abundance of Aminoglycoside and Chloramphenicol_cat ARGs was higher in ICU patients and at the samples collected at the progression stage (Fig. 2A, E).
In the gut, at the genus level, we found that the relative abundance of Fosmidomycin_rosA, Vancomycin_vanT and Multidrug_mexE ARGs were positively correlated with Escherichia, Citrobacter and Pseudomonas (Fig. 5B). At the species level, we note that the relative abundance of Fosmidomycin_rosA and Vancomycin_vanT ARGs was positively correlated with Pseudomonas putida, whereas the relative abundance of Multidrug_mexE ARGs was positively correlated with Pseudomonas aeruginosa. We also observed that the relative abundance of Fosmidomycin_rosA, Multidrug_mdtN and Multidrug_mexE ARGs were positively associated with Escherichia coli (Fig. 5D). Prior studies showed that E. coli was positively correlated with COVID-19 disease severity 31. This observation is consistent with our finding that the relative abundances of Fosmidomycin_rosA, Multidrug_mdtN and Multidrug_mexE ARGs were significantly increased in ICU patients at the progression stage in the gut (Fig. 3C). Moreover, we found that at the species level, the relative abundance of Multidrug_mdtB ARGs was positively correlated with K. pneumoniae in the both the respiratory tract and gut (Fig. 5C, D).
Respiratory tract and gut antibiotic resistome features are associated with immune response in PBMC
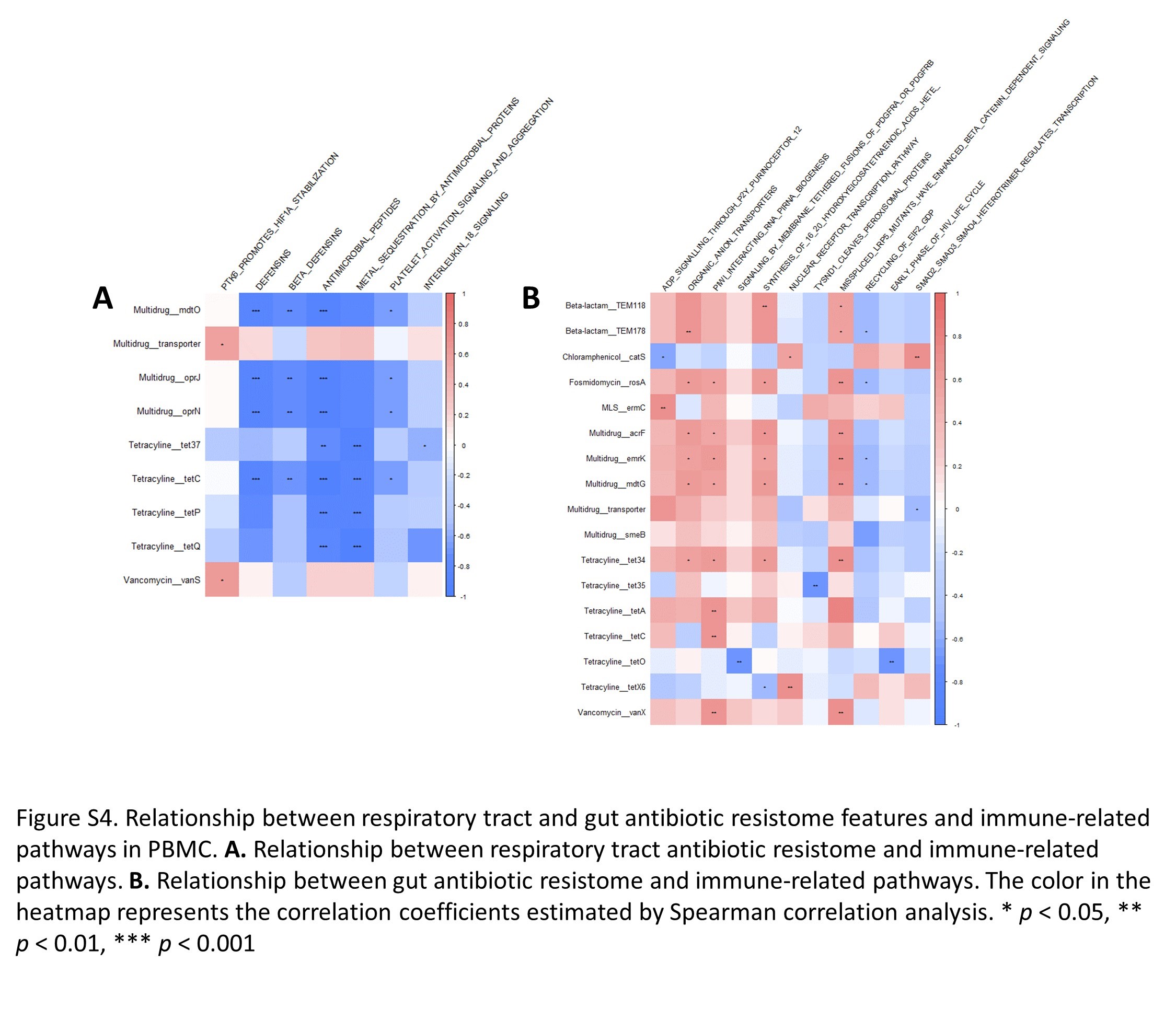
RNA sequencing was performed on PBMC samples of blood from ICU and nICU patients with COVID-19 at the progression stage, and from 18 healthy individuals to explore the relationships between respiratory tract ARGs, gut ARGs, and immune response-related gene expression. To explore this relationship, we carried out a Spearman correlation analysis between the gene set enrichment analysis (GSEA) score of each pathway and relative abundance of ARGs. In the respiratory tract ARGs, we found that the relative abundances of Vancomycin_vanS and Multidrug_transporter types were positively correlated with “PTK6 promotes HIF1A stabilization” (Figure S4, Supporting Information). Moreover, the defensin-related pathways, such as “Defensins”, “Beta defensins” and “Antimicrobial peptides”, were found to be significantly correlated with the relative abundance of subtypes of Multidrug and Tetracycline ARGs. In the gut ARGs, the results showed that the relative abundance of Fosmidomycin_rosA subtype, which was found significantly increased in ICU patients (Fig. 3C), was positively correlated with “Synthesis of (16–20)-hydroxyeicosatetraenoic acids (HETE)” (Figure S4, Supporting Information). This is consistent with the observation that infection with SARS-CoV-2 causes the imbalance of metabolites of arachidonic acid (AA) such as 20-HETE 32.
Respiratory tract and gut antibiotic resistome could accurately classify the disease severity of patients with COVID-19
To identify the antibiotic resistance characteristics associated with COVID-19 disease severity in the respiratory tract and gut, unsupervised random forest classification analysis using a leave-one-out cross validation method was performed at the types and subtypes levels. We identified antibiotic resistance classifiers distinguishing ICU patients from nICU patients based on the respiratory tract ARGs, gut ARGs, and combined respiratory tract-gut ARGs in patients with COVID-19. At the ARG types level, the random forest classifiers based on the respiratory tract, gut, and combined respiratory tract–gut ARGs achieved area under the receiver operating characteristic curve (AUC) values of 0.918, 0.956 and 0.969, respectively (Fig. 6B). The random forest classifier also identified the top ARG types characteristics of ICU and nICU patients. For the respiratory tract classifier, Multidrug, Aminoglycoside and MLS types were the top three characteristic ARGs, which was in line with our finding that relative abundances of Multidrug, Aminoglycoside ARGs in the respiratory tract were higher in the ICU patients (Fig. 1B). For the gut classifier, Vancomycin, Aminoglycoside and Multidrug types were the top three characteristic ARGs, which was in line with our finding that relative abundances of Multidrug and Vancomycin ARGs in the gut were higher in the ICU patients (Fig. 1B). For the combined respiratory tract-gut classifier, Aminoglycoside and Vancomycin ARGs in the gut and Multidrug ARGs in the respiratory tract were the top three characteristic ARGs between ICU and nICU patients (Fig. 6D).
At the ARG subtypes level, the random forest classifiers based on the respiratory tract, gut, and combined respiratory tract–gut ARGs achieved area under the receiver operating characteristic curve (AUC) values of 0.922, 0.958 and 0.965, respectively (Fig. 6C). The random forest classifier identified the top characteristic ARG subtypes between the ICU and nICU patients. In the respiratory tract, Multidrug_mdtC, MLS_macB and Multidrug_mdtG were the top three characteristic ARG subtypes, which was consistent with the finding that the relative abundance of Multidrug_mdtC subtype in the respiratory tract was significantly higher in the ICU patients at the progression stage (Fig. 2E). In the gut, Multidrug_adeC, MLS_msrC and Multidrug_mexF were the top three characteristic subtypes. In the combined respiratory tract–gut classifier, Multidrug_adeC and Multidrug_transporter in the gut and MLS_mefA in the respiratory tract were the top three characteristic subtypes between ICU and nICU patients (Fig. 6E).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}