With an increase in the number of patients with COVID-19, the place of COVID-19 care has moved from the wards to the outpatient setting. Clinics and medical hospitals, particularly those providing primary health care have an increasing role in the appropriate and efficient triage of patients with COVID-19. Such facilities select patients with a current or future requirement for oxygen administration and make decisions about referring patients to a hospital where they can be admitted. Given those situations, risk score to triage COVID-19 patients in an outpatient setting has become required. However, the majority of risk scores proposed up to the present are assumed a serious illness of inpatients. Moreover, those risk scores are consisted of too many components to put to practical use in an outpatient setting. In addition, most risk scores do not target patients with SARS-CoV-2 omicron strains which are prevalent in Japan as of January, 2023. In this study, we aim to overcome these problems.
In the target group before adjustment for background factors (562 vs. 22), age > 65 years, confirmation of pneumonia on CT, chronic kidney disease, body temperature, number of risk factors for COVID-19 progression, respiratory rate, SpO2, number of times vaccinated, age and duration of symptoms were associated with oxygen administration required within 7 days. However, the potential confounding of background factors of age and sex was a concern. In the group adjusted for age, background factors of age and sex with propensity score matching (38 vs. 19), severity classification, diabetes, confirmation of pneumonia on CT, body temperature, respiratory rate, SpO2, hospitalization, and duration of symptoms were significantly associated with oxygen administration required within 7 days. As the severity classification in Japan includes the requirement for oxygen administration as one of the criteria [Table 5], it is not surprising that the severity classification was significantly associated with oxygen administration required within 7 days. Abnormal vital signs, such as high temperature, increased respiratory rate, and low SpO2, were more likely to be associated with oxygen administration required within 7 days. To our knowledge, no reports have examined the association between these vital signs and oxygen administration in patients with COVID-19, especially Omicron strains. On the other hand, for example, high body temperature (BT > 38°C or BT < 36°C) and increased respiratory rate (RR > 20) are included in the criteria for systemic inflammatory response syndrome (SIRS). The primary cause of respiratory failure in COVID-19 is considered to be an exaggerated host immune response. Given these facts, the results relating hyperthermia and increased respiratory rate to oxygen administration required within 7 days seem reasonable.
It is also reasonable that patients with pneumonia on chest CT required oxygen administration within 7 days. The duration of symptoms was significantly shorter in the group requiring oxygen administration within 7 days, possibly due to earlier hospital presentation in more severe cases requiring oxygen within 7 days. The rate of oxygen administration within 7 days was significantly higher in the non-diabetic group than in the diabetic group; 43.2% (19/44) vs. 0.0% (0/13), a result that is inconsistent with clinical findings. The exact cause is unknown, but the target population may have been biased due to inadequate sample size, requiring further study with sufficient sample size.
BMI, administration of immunosuppressive drugs, history of bronchial asthma and smoking, hypertension, dyslipidemia, heart failure, chronic kidney disease, COPD, and the number of times vaccinated were not significantly associated with oxygen administration within 7 days. Concerning these results, the number of patients included in the study was insufficient to detect significant associations. Whether these factors are associated with COVID-19 severity remains controversial and may differ between SARS-CoV-2 strains, requiring further investigation with an increased sample size for each strain.
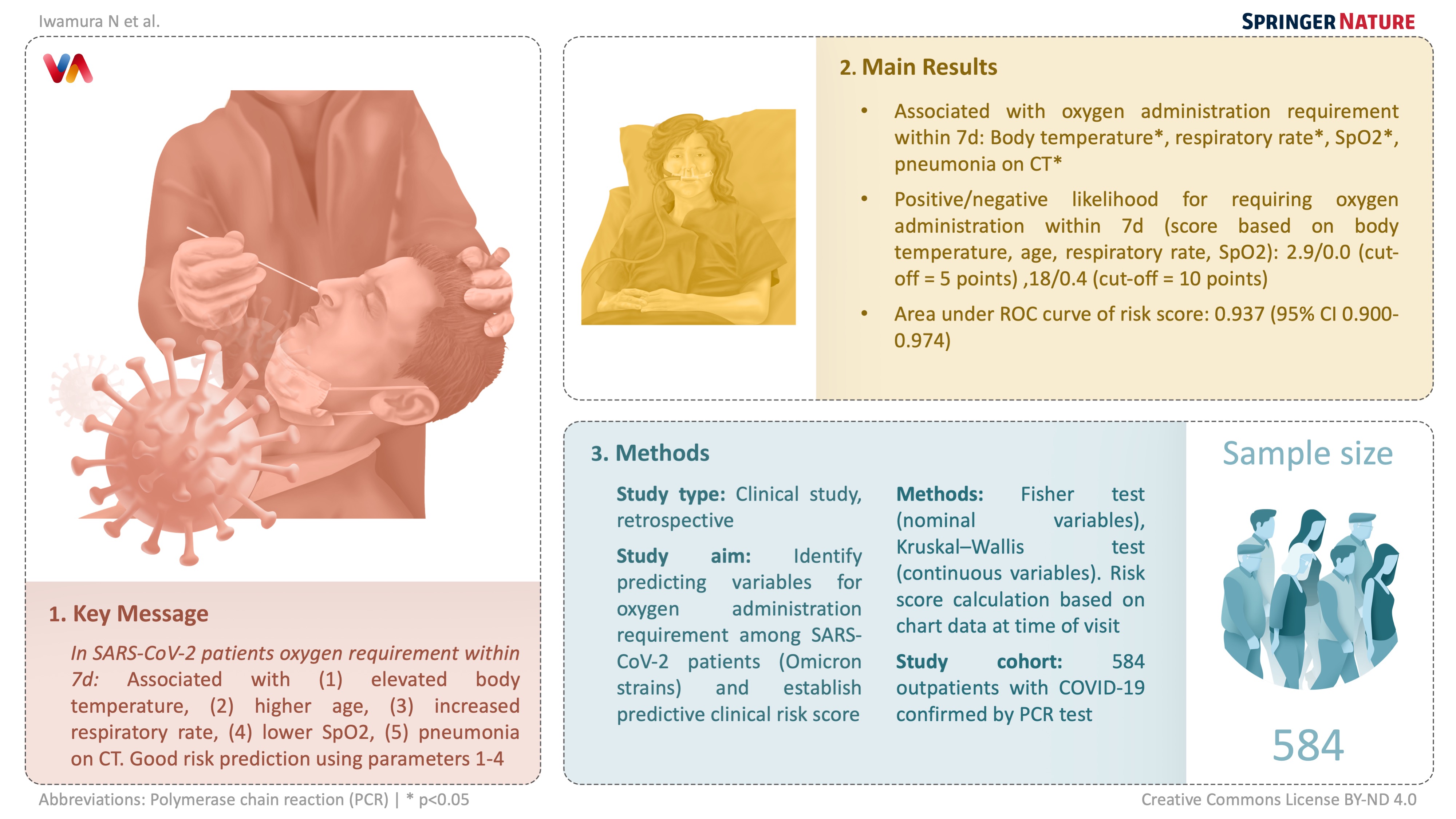
The AUC of the risk score for predicting oxygen administration required using the following evaluation items of temperature, age, respiratory rate, and SpO2 was 0.937 (95% Confidence interval [CI]: 0.900–0.974), which could predict oxygen administration within 7 days with high accuracy. The AUC of the risk score using the following evaluation items of temperature, age, respiratory rate, SpO2, and confirmation of pneumonia on CT was 0.947 (95%CI: 0.911–0.982), which could predict oxygen administration within 7 days with good accuracy. As there was no significant difference between the AUC of both risk scores, we propose a risk score based on the following evaluation items of temperature, age, respiratory rate, and SpO2, which allows a simpler risk assessment without a CT scan or interview with detailed medical history.
Although it is desirable to assess pneumonia by CT scan when deciding whether hospitalization is necessary, many medical institutions have difficulty accessing CT. The accuracy of scoring based on temperature, age, respiratory rate, and SpO2 without confirmation of pneumonia on CT was comparable to scoring with confirmation of pneumonia on CT as an evaluation item. The risk score can accurately predict oxygen administration within 7 days using only age and vital signs.
Nyman M et al. proposed a risk score for COVID-19 positive outpatients to predict 30-day risk of hospitalization based on a retrospective observational study of 67,470 patients with COVID-19 confirmed by PCR test between March 12, 2020 and February 8, 2021. The Mayo Clinic COVID-19 risk score, which is consisted of 13 components included age, sex, chronic lung disease, congenital heart disease, congestive heart failure, coronary artery disease, diabetes mellitus, end stage liver disease, hypertension, immune compromised, nursing home resident and pregnant, showed AUC of 0.837 (95%CI: 0.830–0.843) for the prediction of admission [9]. In our study, the AUC of the risk score for predicting oxygen administration required using the following evaluation items of temperature, age, respiratory rate and SpO2 was calculated as 0.937 (95%CI: 0.900-0.974). This means that our risk score can more efficiently and accurately predict oxygen administration required in an outpatient setting, although the outcomes are slightly different.
A risk score of fewer than 5 points could exclude patients requiring oxygen administration within 7 days with sensitivity/specificity of 100%/65% and a positive/negative likelihood ratio of 2.9/ 0.0. The proportion of patients in the study who required oxygen within 7 days was 3.77% (22/584). With the prior probability of 3.77%, the positive/negative predictive value with a cut-off of 5 points was calculated as 10.1%/100%. On the other hand, a risk score of 10 or more points could diagnose patients requiring oxygen administration within 7 days with a sensitivity/specificity of 59%/97% and a positive/negative likelihood ratio of 18/0.4. With the prior probability of 3.77%, the positive/negative predictive value at a cut-off of 10 points was calculated to be 41.9%/1.63%.
Given these results, we propose a risk category classification with a risk score of fewer than 5 points as a low-risk group, 5 to 10 points as a moderate-risk group, and more than 10 points as a high-risk group. In the study patients, the proportion of patients requiring oxygen administration within 7 days was 0.0% (0/367) in the low-risk group, 4.8% (9/186) in the moderate-risk group, and 42% (13/31) in the high-risk group [Table 6]. On this basis, it is suggested that in clinical practice, the low-risk group should not be required to be hospitalized, the moderate-risk group should be considered for hospitalization, and the high-risk group should be required to be hospitalized.
{kind=link}