In the fifth edition of the WHO Classification of Tumors of the CNS, the role of molecular diagnostics has been raised to an unprecedented level. Nevertheless, efficient biomarkers for glioma have not been found. Glioma cells were characterized by their heterogeneity, which means the divergent differentiation of glioma cells during proliferation 28,29. On the other hand, as a manifestation of heterogeneity, multidirectional differentiation trajectories often mean components that do not exist in the origin tissues that appeared. For example, muscle cell appears in glioblastoma 30–32. This phenomenon often implied high malignancy 33,34. Therefore, the characteristics of cell differentiation trajectories might be the linchpin to revealing the heterogeneity of glioma cells.
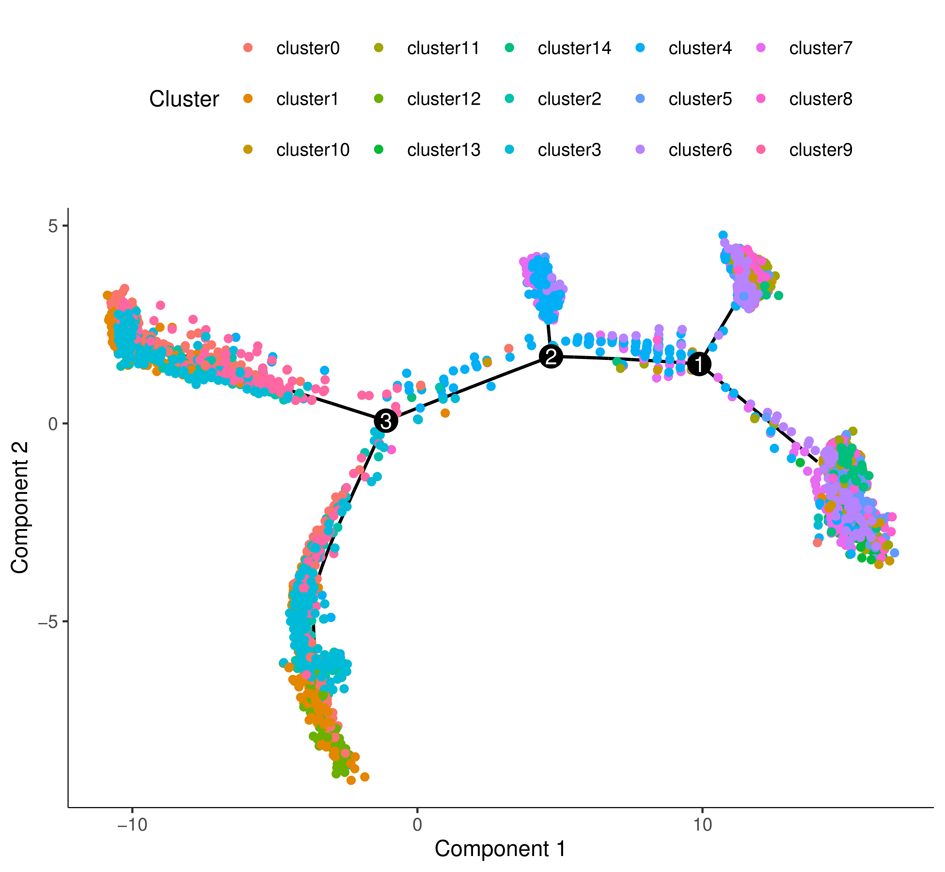
In our research, the pseudotime analysis revealed the correlation between heterogeneity and cell differentiation trajectory in glioma cells. Results indicated that glioma-related components, such as astrocytes and neurons, only appeared in specific differentiation trajectories. Therefore, the differential expressed genes in these trajectories were marked as GDRGs. Meanwhile, KEGG and GO analysis indicated that GDRGs were involved in cell differentiation, cell adhesion, cytoskeleton actin movement, cytotoxicity, and cell cycle regulation which were closely related to the malignancy of glioma cells 35–38. These results preliminarily prove that the multidirectional differentiation trajectories were related to the heterogeneity of glioma cells.
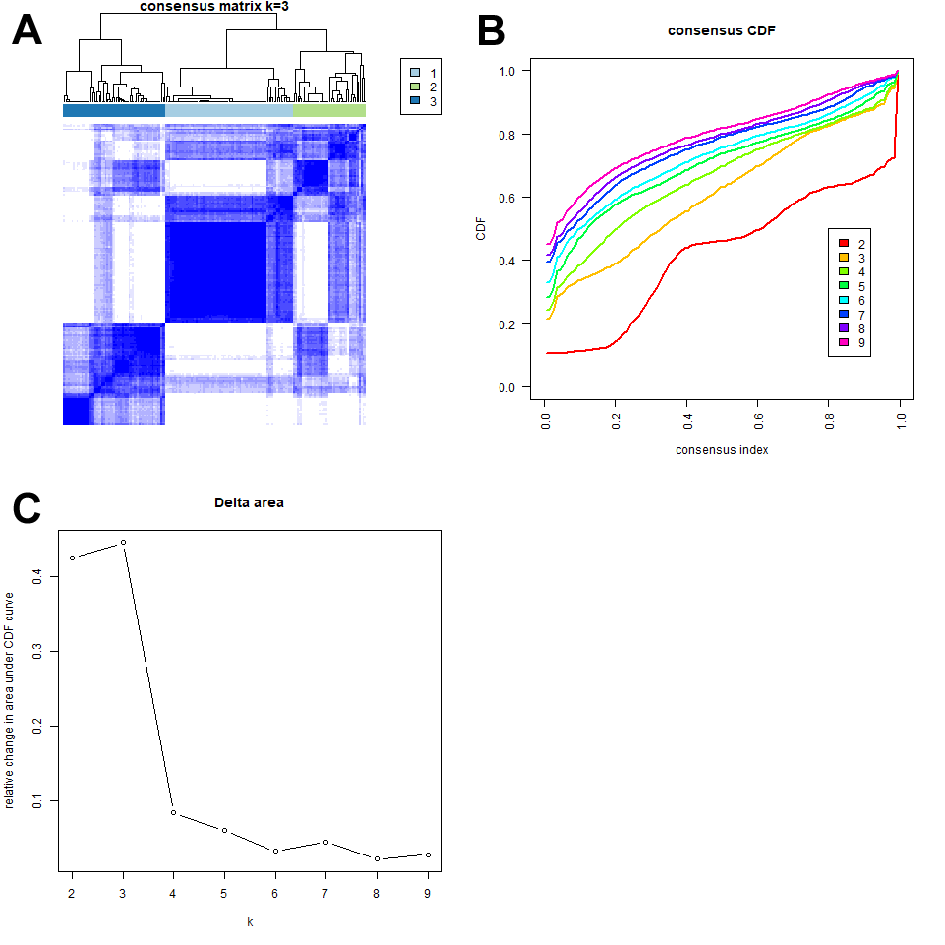
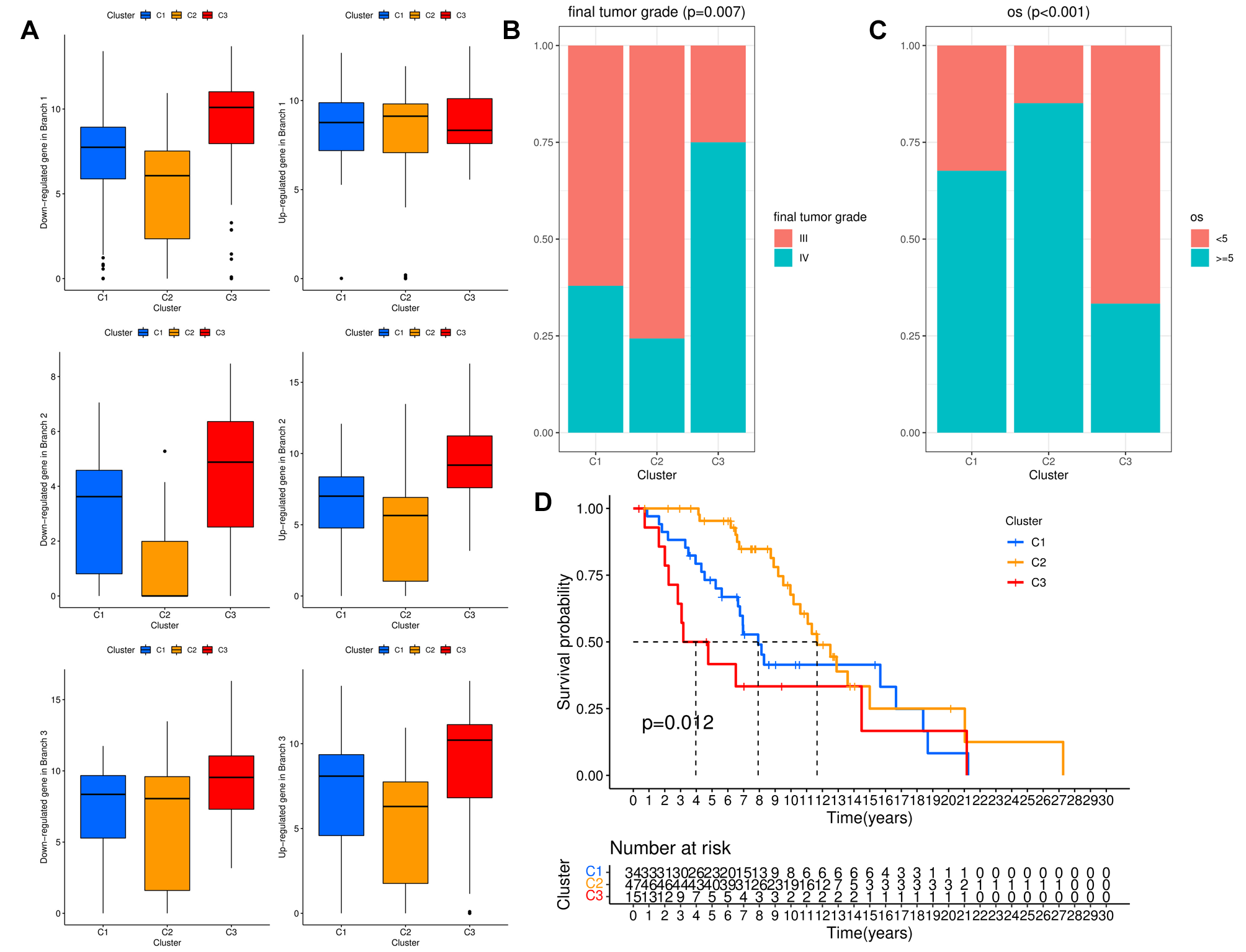
Previous studies have proved that immunocytes in glioma were mainly immunosuppressive anti-inflammatory M2, and the proportion in glioblastoma reached 30% 39–44. In this research, the pseudotime analysis also suggested that macrophage existed in glioma-related differentiation trajectories, which implied the potential connection between glioma cell heterogeneity and macrophage infiltration. Therefore, we established a GDRGs-based molecular subtype. ESTIMATE and CIBERSORT results suggested there were significant differences in the distribution of immunocytes between subtypes, among which the M2-dominated subtype had the highest immune/stromal scores, the lowest tumor purity, and the worst prognosis. All these results proved that GDRGs could regulate the M2-dominated immune landscape in glioma and affect the prognosis.
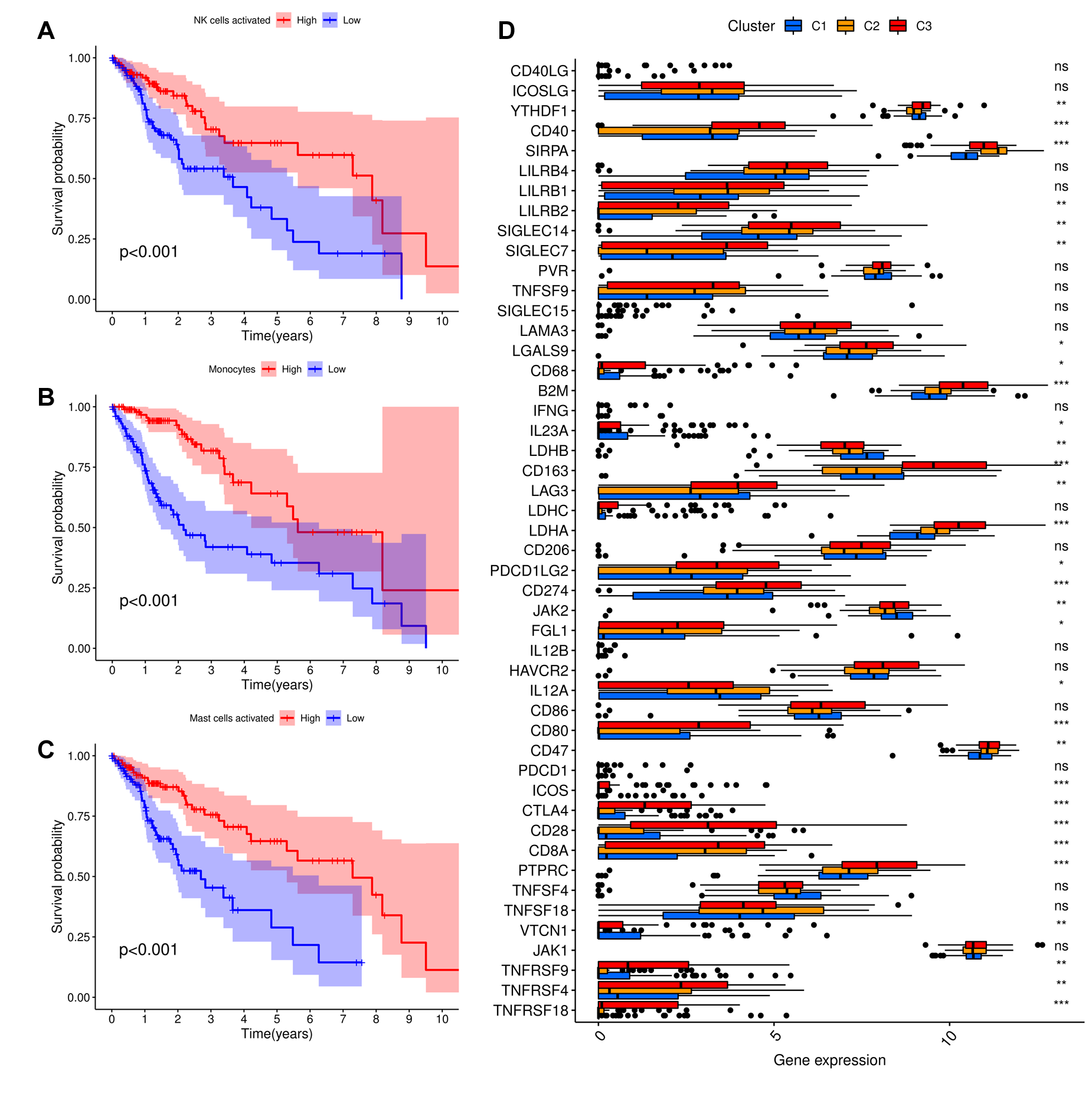
The inhibitory regulation of immune checkpoints might be the foundation of GDRGs regulating the immune landscape of glioma. Usually, immune checkpoints could stabilize the immune system and prevent autoimmune diseases by regulating the intensity, amplitude, and duration of antigen presentation in the immune response. However, due to its ability to block antigen presentation, the over-activation of immune checkpoints resulted in immune tolerance and immune escape during tumor progression 45–49. In this study, 41 immune checkpoints related to the activation of M2, T cells, and NK cells were cross-validated by differential and Kaplan-Meier analyses. The expression of macrophage-related immune checkpoints among trajectories was consistent with the immune/stromal scores and the distribution of macrophages among molecular subtypes. These particular immune checkpoints included the iconic M2 receptors CD206 and CD163 50–53; CD47-SIRPα, which were functioning as ligand-receptor pairs that transmit phagocytosis signals of macrophages54,55; LILBRs family members of LILRB1, ILLRB2, and LILRB4, who directly expressed on the surface of tumor cells and stimulated tumor cells growth by combining with MHC-Ⅰ 56,57.
After all these, a GDRGs-based prognostic RS signature composed of SOX4, MEX3A, EGFR, NES, ENC1, NEFL, NNAT, and TMSB15A was established. The results showed that the OS of the low-risk group was significantly better than that of the high-risk group, and the calibration curves for predicting 3-year and 5-year survival were consistent with the observed values, which confirmed the effectiveness of these 8 GDRGs as prognostic risk factors. It should be noted that the role of SOX4 and EGFR in the anti-PD-1 immunotherapy of non-small cell lung cancer (NSCLC) was partially verified. They might have potential advantages in immunotherapy glioma. At last, according to the clinical pathological characteristics and RS, a nomograph was established to predict 3-year and 5-year survival. The calibration curve confirmed the accuracy of the prediction.
In conclusion, this study pioneered discovering a novel cell differentiation trajectory-related molecular subtype and preliminary exploring the regulatory role of GDRGs on the M2-dominant immune landscape in glioma. In the meantime, GDRGs formed an efficient diagnostic RS signature and nomogram that predicted the glioma's prognosis. Of course, there are some limitations to this study. The most obvious problem is that this study only uses transcriptome, high throughput sequencing, and scRNA-seq data for bioinformatics analysis without experimental support, and subsequent validation in vitro and in vivo is required.
{kind=link}
{kind=link}
{kind=link}
{kind=link}