In recent years, increasing attention has been paid to the factors of abnormal intraocular blood flow or vascular regulation ability in the development and progression of various types of glaucoma. With the widespread use of OCTA technology in clinic, the further understanding was obtained regarding the retinal microcirculation state in these patients with normal IOP after APAC. In the present study, the OCTA technology was used to accurately segment the vascular structure of superficial retina in the macula, quantify microcirculation function, and assess its diagnostic ability to APACG compared with traditional retinal structural parameters.
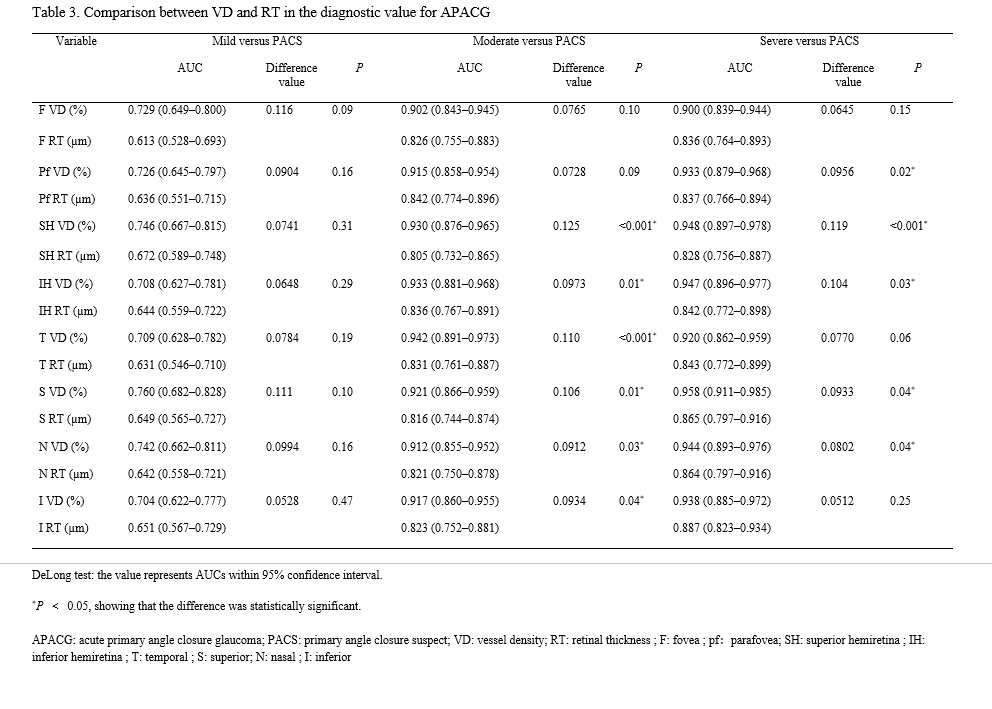
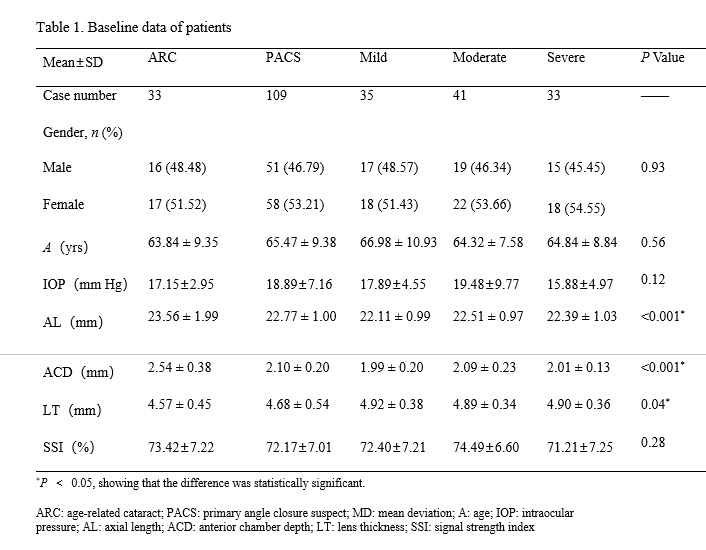
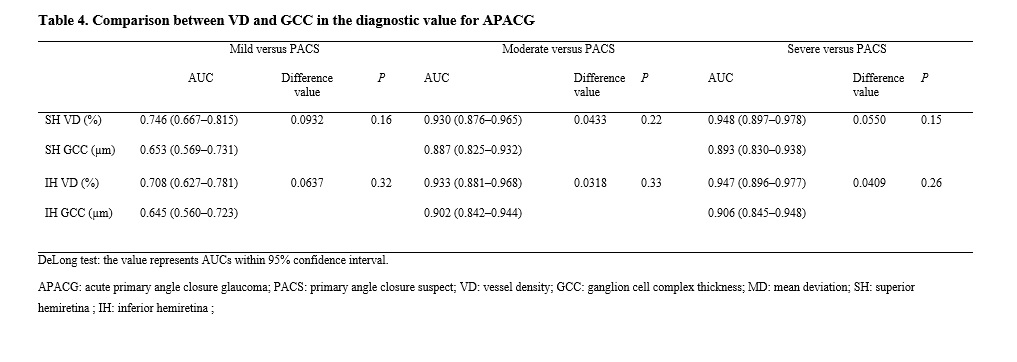
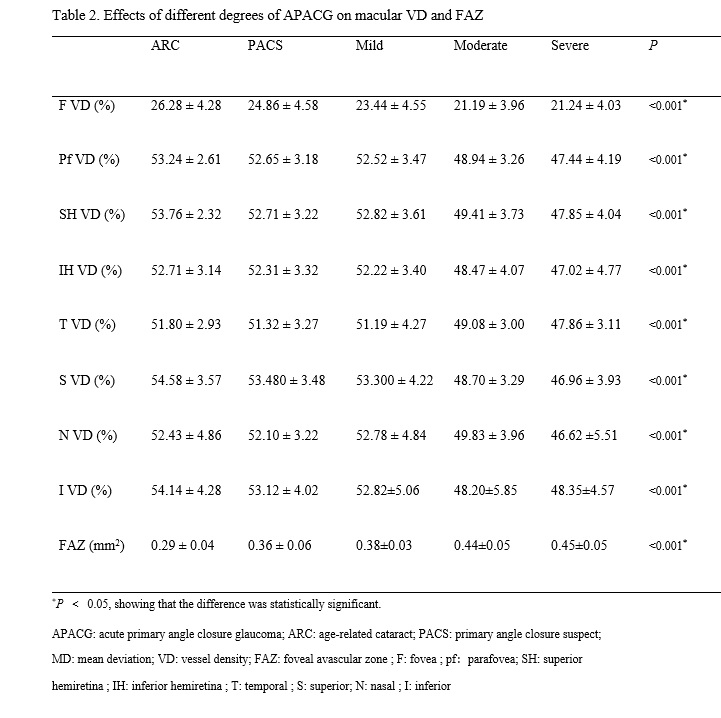
In the present study, no statistical difference in IOP was found among the five groups on OCTA examination, indicating that IOP, the main influencing factor, was excluded. The VD and FAZ still showed significant changes with the exacerbation of APACG. In the macular area, VD gradually decreased and FAZ gradually increased. The differences in F VD and FAZ were statistically significant between the mild group and the ARC and PACS groups, suggesting that the two parameters were sensitive indicators of the retinal microcirculation state in patients with APACG having a previous history of acute attack with mild visual field damage. At the same time, this study found that compared with RT, the diagnostic value of VD was higher. For the moderate versus PACS groups, the difference in AUCs between them in six areas was statistically significant. For the severe versus PACS groups, the difference in AUCs between them in the five areas was statistically significant, but the difference reduced. The difference in AUCs between VD and GCC in the macular area was not statistically significant in the three groups of APACG, indicating that compared with traditional structural parameter RT, VD had a higher diagnostic value for APACG. Also, compared with the classic indicator GCC for glaucoma damage, the diagnostic value of VD was higher.
This study focused on the macular area. Similar studies found that the VD around the optic nerve head after APAC was still low in the normal IOP [21]. Previously, due to limitations of examination methods, APACG was usually characterized by anterior segment ischemia, and 52.5% of patients with APACG had changes in iris ischemia [22]. It was believed that the iris stroma had the least anti-damage ability against IOP elevation during APAC. With the application of OCTA, the damage caused by transient IOP elevation to the retina was also significant. The decrease in VD in the retina and macular area led to chronic damage, such as ischemia and hypoxia. Of note, the VD obtained by OCTA was used to estimate the blood flow velocity. Instead, it should be understood as the two conditions of capillary detachment or slow blood flow velocity in the vessel. Therefore, in addition to the application of IOP-lowering drugs, those used for improving the retinal microcirculation should be given.
Related studies on POAG found that the retinal capillary density in a normal population was different from that in patients with moderate POAG. No difference was found in the comparison between patients with moderate and severe POAG[9], which was basically consistent with the change trend of VD in the macular area for different degrees of APACG in this study. Comparing the moderate and severe APACG groups with the ARC and PACS groups, the differences in all parameters were statistically significant. In the comparison between the moderate and severe groups, the difference in VD in the three areas was not statistically significant. This might be because early glaucoma was characterized by progressive microvascular changes, and as the disease progressed to a severe stage, the apoptosis of RGCs was predominant, and the microvascular changes were few. Therefore, the OCTA parameters had a better ability for the early diagnosis of the disease than the late diagnosis [23].
The parameter FAZ is progressively enlarged under conditions of advancing age, diabetic retinopathy, retinal vein obstruction, and so forth [24-26]. This is because the macular capillary loss, as a marked characteristic of ischemic and vascular occlusive retinal disease, can lead to significant changes in FAZ, which can be assessed according to the area, perimeter, and so forth, of the FAZ [27-29]. At present, little is known about the association between FAZ and glaucoma. Studies have shown that patients with glaucoma having central visual field defects have larger and irregularly shaped FAZ compared with those with normal or peripheral visual field defects, but there was no significant difference in FAZ area between peripheral and central visual field defects [30, 31]. At the same time, patients with NTG have a larger FAZ area and decreased peripheral vascular density. The OCTA technology has been used to further demonstrate that NTG is an ischemic disease characterized by vascular dysfunction [32]. In the present study, FAZ significantly changed in the early stage of APACG, indicating that it was a sensitive indicator of APACG-induced changes in retinal circulation.
Prior studies have shown that VD measured by OCTA can be used as an indicator to identify healthy eyes and glaucoma, and also distinguish between healthy people and those with suspicious glaucoma [10, 33]. Henry et al. studied the AUCs of glaucoma and healthy eyes. They showed that the retinal nerve fiber layer (RNFL; 0.95) and GCC (0.95) had the highest values, followed by the macular VD (0.94) and peripapillary VD (0.93) [34], indicating that the diagnostic value of VD in the macular area was similar to that of other known indicators, such as RNFL and GCC, which was consistent with the results of this study. The advantages of using the macular VD in the diagnosis and assessment of APACG were as follows. First, the damage of early glaucoma might occur more clearly on the omentum away from the optic nerve head [35], and therefore early changes in peripapillary VD or RNFL may not be detected. Second, early retinal edema after an acute attack caused no difference in GCC and RNFL thickness between APACG and PACS eyes. Third, the myopic optic disks, especially high myopia, were usually characterized by a slanted appearance and atrophy of the temporal optic nerve head, and the perfusion of retina of the optic nerve head was less than that of the emmetropic eye, impeding the differential diagnosis of APACG and normal eyes [36, 37].
This study had some limitations. The study showed that the scan pattern of 6 ´ 6 mm2 region in the macular area was more accurate than that of 3 ´ 3 mm2 region in terms of diagnostic accuracy. The smaller scan range might miss part of the GCC area [9]. However, most of the patients with APACG having a history of acute attack were treated with 1% pilocarpine eye drops. Also, pupils of the affected eyes were small, and the scan pattern of 3 ´ 3 mm2 region was more reasonable. The IOP-lowering eye drops have a potential confusing effect on eyeball hemodynamics and retinal vascular autoregulation. For example, carbonic anhydrase inhibitor and prostaglandin analogues could result in vessel dilatation and increased blood flow [38, 39], but the effect took 1–4 weeks to be removed after discontinuing IOP-lowering eye drops. Therefore, it was not discontinued on examination. No measurement of the blood pressure of participants or recording of their antihypertensive medications was performed. However, a previous study also suggested no correlation between blood pressure readings and VD of the optic nerve head on OCTA [33]. Several studies found that the decrease in VD of the optic nerve head and the corresponding macular area could be detected in patients with glaucoma having unilateral visual field defects [40]. VD (59.0% and 51.1%) in the hemi-optic nerve head and macular areas for the intact visual field was higher than that for the affected visual field (54.7% and 48.3%, respectively), but lower than that of healthy eyes (62.4% and 53.8%). These findings suggested that vascular changes might occur before detectable visual field defects. Therefore, the correlation between VD and visual fields in patients with APACG needs further investigation.
In conclusion, for patients with APACG and IOP returning to normal after treatment, the VD and FAZ in the macular superficial layer were still lower than normal, and the damage of VD and FAZ aggravated with the exacerbation of APACG. The VD in the macular superficial layer showed higher diagnostic ability than RT, which was equivalent to that of GCC. These findings provided new insights into the pathophysiological study of patients with APACG having a history of acute attack, and also new indicators for the clinical diagnosis of APACG.
{kind=link}
{kind=link}
{kind=link}
{kind=link}