We designed a perspective, randomized placebo-controlled double-blind trial (RCT) in order to assess the possible effect of iron supplementation on neurological development (primary outcome of the study) in healthy LPT. The RCT was sponsored by Pediatrica Specialist®, that provided both iron and placebo preparation.
Sixty-six healthy LPT infants born between 340⁄7 and 366⁄7 weeks of Gestational Age (GA) at Fondazione Policlinico Gemelli IRCCS - Catholic University of Rome and admitted to the Neonatology Unit (Rooming-in ward) were enrolled in the study, once informed consent was obtained from the parents. GA was evaluated according to the first trimester ultrasound scans or, when not available, with the last menstrual period confirmed by Ballard's score14.
All enrolled neonates were submitted to cerebral ultrasound assessment at birth.
Infants with uncertain GA, major congenital anomalies, congenital or neonatal infections, neurological and/or neurosensory disorders, cerebral ultrasound anomalies, severe intrauterine growth restriction (SGA <3° centile), neonatal asphyxia, respiratory distress, hematologic disorders were excluded from the study, as well as newborns admitted to Neonatal Pathology Unit or Intensive Care Unit.
All neonates had a complete blood count check to exclude anemia at two weeks of age according to Christensen reference values15.
The newborns enrolled in the study were randomized in two equal groups (thirty-three patients each group); one group received martial prophylaxis from the third week of life to six months of post-conceptional age (Iron group), the other received placebo (Placebo group), similar in shape and flavor and administered in the same way. Iron supplementation consisted of a dosage of 2 mg/kg/day orally in two administrations of iron pidolate in drops (Pediafer plus® drops 15 ml).
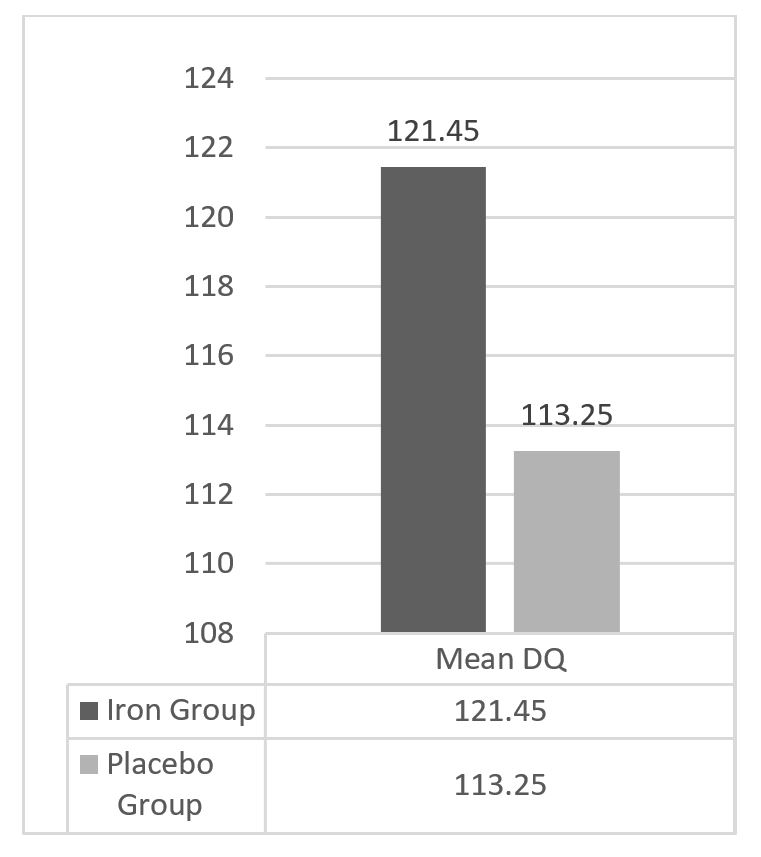
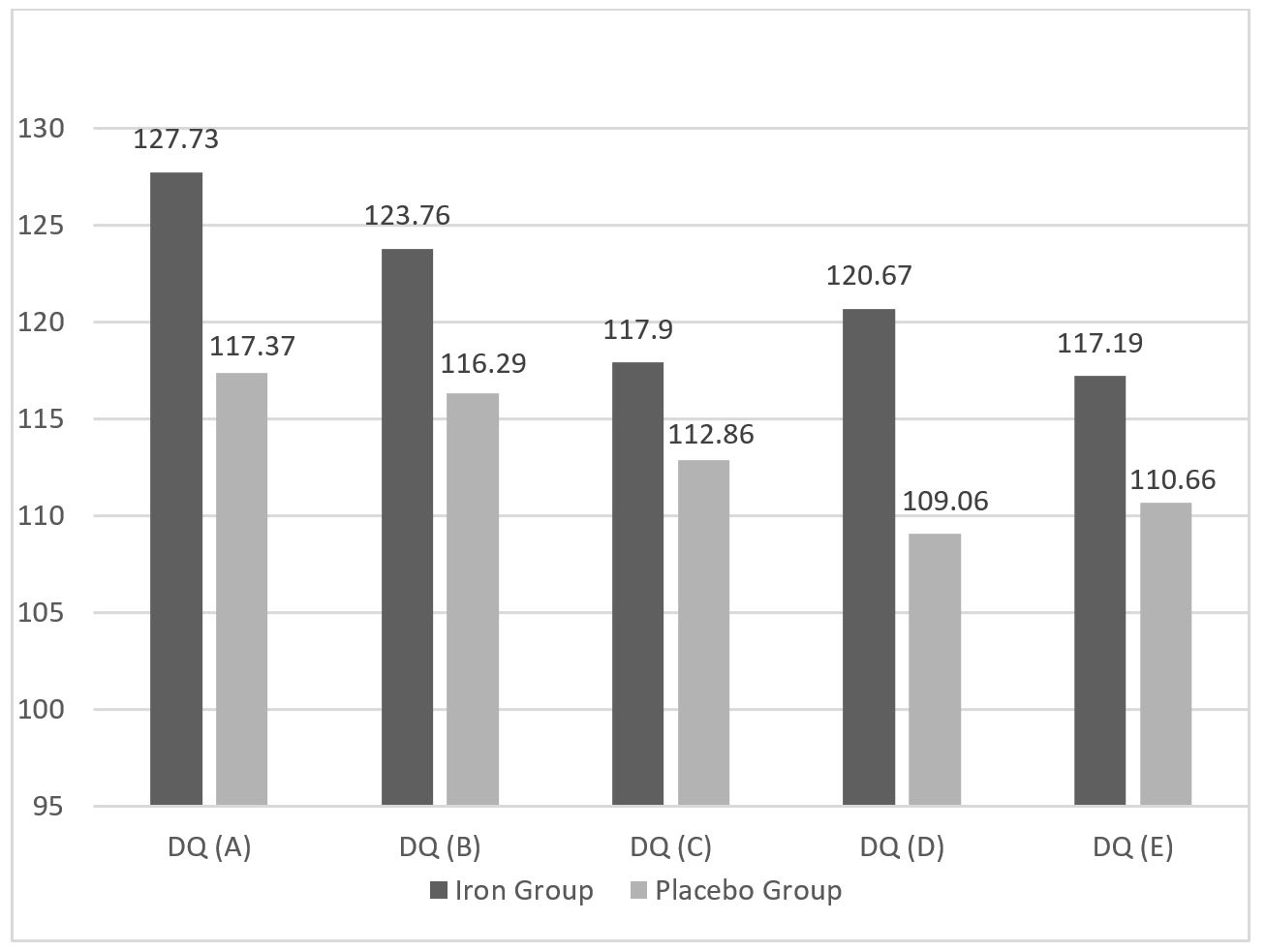
A clinical examination was performed at 6 months of age to ascertain the compliance in treatment regimen and to assess the infants’ general wellness. Every patient was assessed using the Griffith Mental Development Scales (GMDS)-II edition at 12 months of post-conceptional age. The GMDS includes five subscales: A (locomotor), B (personal and social development), C (hearing and speech), D (hand and eye coordination) and E (performance). Each scale provides a mental age and a developmental quotient (DQ). The total DQ was calculated from the mean of the developmental quotients obtained in each of the five subscales.
The DQ was considered “normal” if greater than 85, “borderline” between 85 and 70 and suggestive of development delay if less than 70.
The RCT was approved by the Ethical Committee of our institution, Protocol N° 11218/13.
STATISTICAL ANALYSIS
We calculated the sample size on the hypothesis that iron supplementation would be able to increase
neurodevelopmental GMDS scores by approximately 8%. We decided to fix an 8% improvement in supplemented group based on Morag et al.16 study results. The Authors compared the scores obtained by 124 late preterm and 33 term infants and found significantly lower scores in the preterm group in all subscales, being 8% the greatest difference obtained in the Performance scale. According to the study by Morag et al.16, where the mean Developmental Quotient for Performance Subscale was 84, with a Standard Deviation (SD) of 10, the expected mean Developmental Quotient for Performance Subscale was estimated as 91 with a SD of 10. Setting a significance level of 0.05 and a power of 0.80, the calculated sample size required was determined to be 33 for each study group.
Statistical analysis was performed using Graphpad software 2018®. Student t test for independent data was used to evaluate differences in neurological assessment between the two groups of our study. For all analyses a p-value <0.05 was considered significant.
{kind=link}
{kind=link}