Trial Design
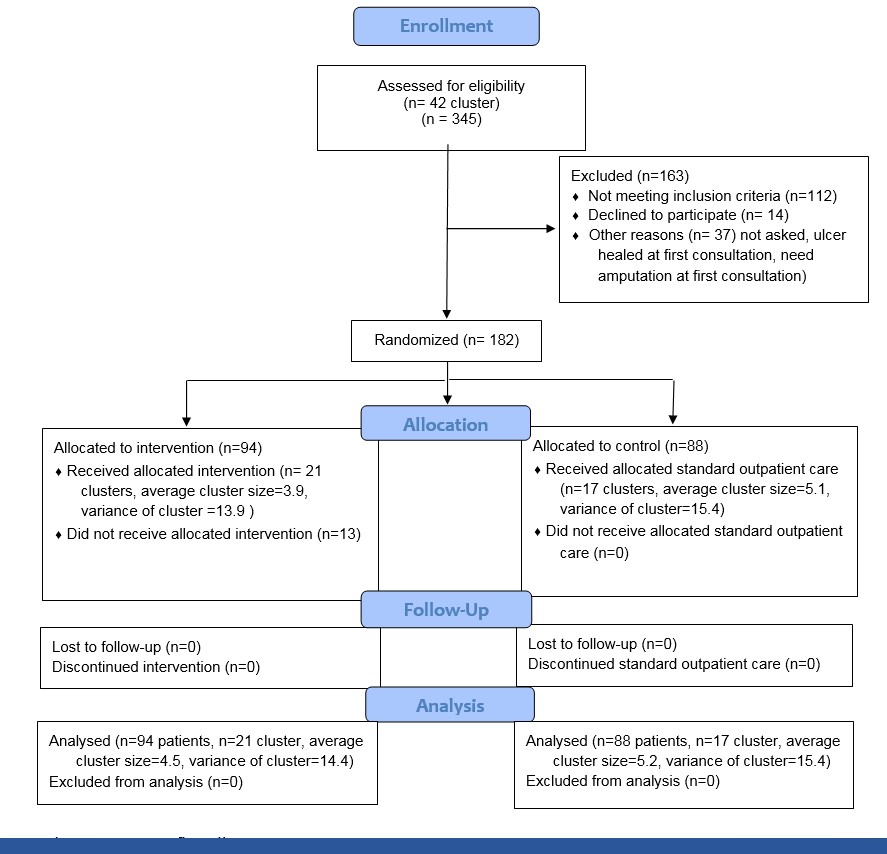
The design of the study has been described previously [9, 10]. Briefly, this was a multicenter cluster-randomized controlled noninferiority trial. Patients from three clinical sites in western Norway were included (NCT01710774). The recruitment period lasted from September 2012 to June 2016. A total of 182 patients were included, 94 in the TM group and 88 in the control group in 42 municipalities/districts. Forty-two clusters were matched in 21 pairs which were then randomized to either TM or control. These were matched in pairs according to population size and rural/urban characteristics. The randomization sequences were generated by an independent statistician using SPSS version 21 statistical software (IBM Corp) [10]. The study was approved by the Western Norway Regional Committee for Medical and Health Research Ethics (2011/1609). All participants gave written consent. The study adheres to CONSORT guidelines (Additional file 1).
Participants
Included in the original trial were patients with type 1 or type 2 diabetes who were 20 years or older, diagnosed with a new DFU [9], defined as a skin lesion below the ankle. Excluded were patients who had an ulcer on the same foot treated during the last 6 months in specialist healthcare or a diagnosis of mental disorder or cognitive impairment. Another exclusion criteria was having a life expectancy less than one year, and the patient also had to be able to understand and write Norwegian [10]. Patients in both groups were followed until ulcer healing, amputation, or death, up to a maximum of 12 months of follow-up. (The Consort flow chart for the primary study is available as Figure S1 in the supplementary appendix.)
In the current study we included all participants with at least one valid patient-reported outcome measure at baseline in the TM group (n=78 (83.0 %)) and in the control group (n= 78 (88.6%)). PROMs were collected at baseline and at predefined endpoints (healed ulcer or amputation or at 12 months if the ulcer did not heal). For persons who died during follow-up or were lost to follow-up for other reasons, only the baseline measurements were used in analyses and these persons did thus not contribute to the estimation of the intervention effect.
Intervention
Telemedicine (TM). The randomization procedures and a more in-depth description of the intervention have been reported previously [9]. Briefly, community nurses used a mobile phone to take pictures of the ulcer which was then sent via a web-based platform to the hospital for review by a specialist health care professional, facilitating counseling and feed-back. This platform is a web-based ulcer record system accessible from mobile devices and computers via the Internet [9-11]. The system makes it possible to register relevant data regarding the ulcers, digital images of the ulcers, describe the situation and possible problems, and to ask for and give advice. Measurements can be compared over time to visualize the healing process of the ulcer. This allows all involved staff to contribute, even though some of them will not necessarily be situated in the vicinity of the patient. The system has functionality for documentation related to ulcer treatment at a far higher level than standard electronic health records in use in Norway. This system is customized for collaboration, discussions, and advice regarding the treatment between cooperating medical staff in different health care institutions. The main reason for using the web-based ulcer record system is the collaboration functionality that enables integrated care across different levels of the health care sector. All relevant ulcer data are stored in a shared database, accessible to medical staff involved in the treatment of the patient and registered in the user directory of the system, regardless of which institution they are employed by. During follow-up, the community nurses provided care under supervision of the specialist nurses at the outpatient clinics and communicated at least weekly with the specialist nurses at the outpatient clinic [10].
Standard Outpatient Care. Patients in the control group received standard care provided by the outpatient clinic, normally scheduled to take place every second week. The medical treatment given to the control and intervention group is based on the same evidence-based procedures [10].
PROMs
We used both generic and disease-specific PROMs to assess the patients’ perceptions of the intervention on self-reported health and well-being, and QOL. Included were three generic instruments (Euro-QOL EQ-5D-5L/ EQ-5D-VAS, the Hospital Anxiety and Depression Scale (HADS), the WHO-Five Well-Being Index (WHO-5)), and two disease-specific measures; Problem Areas In Diabetes (PAID-20) and Neuropathy and Foot Ulcer–Specific Quality of Life (NeuroQOL).
We used the EQ-5D-5L questionnaire as a health utility score [12]. The first part comprises five single item dimensions of health: mobility, self-care, usual activities, pain/discomfort and anxiety/depression, with ratings on five levels of perceived problems from no problems (1) to extreme problems (5). The level scores are presented as global health indices with a weighted total value for health status [13]. Part two is a Visual Analogue Scale (VAS) ranging from 0 (worst health state) to 100 (best health state), and used as an overall measure of perceived health status [12]. The WHO-5 was used to describe well-being during the previous 2 weeks [14]. Five items with ratings from 0-5. Item scores are summed (0-25) and transformed to a 0–100 scale with higher scores indicating better well-being. The HADS assessed anxiety and depressive symptoms during the past week [15]. This instrument comprises seven items on anxiety (HADS-A) and seven items on depression (HADS-D). Each item is scored from 0 to 3, yielding a maximum score of 21. Higher scores indicate a higher symptom load.
Diabetes distress was measured with PAID-20 [16, 17]. The instrument covers frequently reported emotional states. Scale scores are transformed to a 0–100 scale, with 100 indicating greater distress. The cut-off score is suggested to be equal or more than 40. The NeuroQOL assessed patients’ perception of the impact of foot ulcers on their QOL [18]. The instrument consists of six domains: 1) painfully symptoms and paresthesia; 2) symptoms of reduced/lost feeling in the feet; 3) diffuse sensory motor symptoms; 4) restrictions in daily activities; 5) interpersonal problems and 6) emotional burden. Higher scores indicate a greater negative impact of foot ulcers on QOL.
Other measures
Healing of the ulcer was defined as healing (intact skin) of the whole foot without minor or major amputations. Amputation was defined as minor or major amputation before ulcer healing. Amputation performed below the ankle was defined as minor amputation, whereas amputation above the ankle was defined as major amputation. Death was defined as death before ulcer healing.
In addition, clinical data, comorbidities and foot ulcer specific data were collected from the electronic medical journals at the clinical sites. Those with grade 2 or grade 3 combined with stage C and D were defined as high severity and all other grades and stages were combined to a group with versus low and medium severity [19]. Other measures as demographic data and lifestyle characteristics were self-reported by the patient [10] (Table 1).
Statistical Analyses
Data were analyzed according to the initial group allocation (intention to treat). Continuous variables are presented as mean and standard deviations (SD), and categorical variables are presented as proportions. We used linear mixed effects regression analyses with random intercept to account for clustering within treatment groups. Intra-cluster correlation for the primary outcome healing time in the main study was 0.0014. All models were specified with the sum score of the PROMs (EQ-5D-5L, HADS, WHO-5, PAID-20 and the NeuroQOL subscales respectively) as dependent variables with fixed effects for time, group allocation and interaction between time and allocation group. The coefficient for the interaction term between time and allocation group was reported as the intervention effect and can be interpreted as the difference in change in PROM score between the two groups after adjustment for baseline differences in PROM score. The intervention effects are reported as regression coefficients with 95% CIs. For analyses of the dichotomous outcome PAID>40 we used generalized estimation equations (GEE) instead of linear mixed models. Sample size calculation is reported previous [9].
Additional Analyses
In additional analyses, we tested whether distance to the outpatient clinic moderated the intervention effect. We conducted a subgroup analysis with a linear mixed model, including only patients who lived 25 km from the outpatient clinic. All analyses were also repeated excluding 13 patients originally assigned to the TM group who did not receive TM (per protocol analyses) [9, 10]. A greater percentage of participants in the intervention group with ulcers on the toes than in the control group suggested possible differential selection. In sensitivity analyses we therefore repeated the linear mixed-effects regression analyses and GEE adjusted for localization of ulcer. We also did analyses with stratification on severity of ulcer measured in terms of grade and stage from the UT classification system [10, 20]. Statistical significance was defined as P < 0.05. Statistical analyses and graphs were performed and constructed in Stata (version 14).
{kind=link}