A 63-year-old male, who suffered from hematochezia and abdominal pain, was diagnosed with stage Ⅳ (pT3N1M1) colorectal carcinoma with liver metastases in June 2020. Since that the patient presented with intestinal bleeding, surgical resection was performed to alleviate the symptom. Endoscopic resection revealed two lesions on the surface of the colorectal, named A and B, and only tumor A was removed (Fig. 1). To search for an efficient therapeutic strategy, genomic DNA from formalin-fixed paraffin-embedded (FFPE) sample of tumor A and circulating tumor DNA (ctDNA) from plasma were subjected to targeted next-generation sequencing (NGS) of 425 cancer-related genes (Nanjing Geneseeq Technology Inc.) (Fig. 2A). Their genetic alterations were compared in Table 1. To our surprise, the mutation pattern was completely different between plasma and tumor A. Based on the KRAS G12D with with a mutation allelic frequency (MAF) of 41.9% identified in tumor A, the patient was administrated with the XELOX plus bevacizumab (oxaliplatin 130 mg/m2 day 1, capecitabine 1500 mg/m2 twice daily for 14 days, bevacizumab 7.5 mg/kg day 1) for every 3 weeks as first-line treatment. The patient achieved an initial partial response (PR) with sustained response ongoing for 11 months. In January 2021, the tumor was evaluated PD, which led to second-line chemotherapy involving irinotecan (180 mg/ m2 day 1), raltitrexed (3 mg/ m2 day 1) and bevacizumab (5 mg/kg day 1) for every 2 weeks. However, the size of liver lesion increased 35% compared to baseline, which indicated a PD (Fig. 2B).
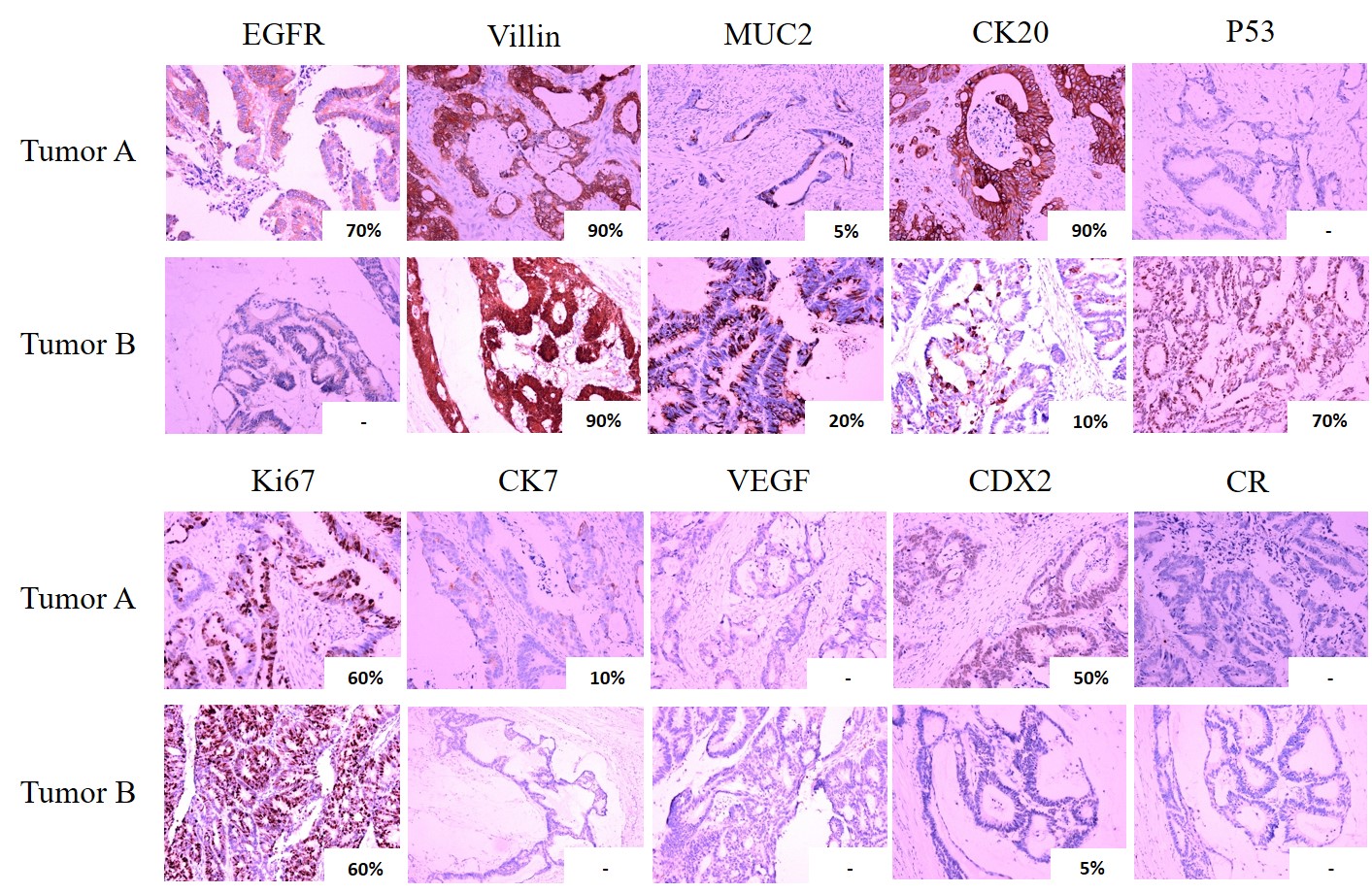
In April 2021, the plasma and tumor B were subjected to NGS, which identified four same mutation types without any KRAS mutations (Table 1). Compared genomic alterations between the tumor A and B, the mutation landscapes were completely different. Additional, Immunohistochemistry (IHC) staining showed significant differences between the two tumors (Supplementary Figure S1), consistent with the determination of MPCC. Based on the wild-type KRAS, the patient was subjected to the treatment of irinotecan (180 mg/ m2 day 1), raltitrexed (3 mg/ m2 day 1), plus cetuximab (500 mg/ m2 day 1), a monoclonal antibody that blocks the epidermal growth factor receptor (EGFR), for every 2 weeks in April 2021. Plasma ctDNA sequencing and CT scan were performed every two weeks and two months, respectively (Fig. 2B and C). Two months later, the size of liver metastases decreased by 75% compared to the results of last detection and ctDNA abundance quickly decreased to < 1% (Fig. 2B and D). Moreover, the tumor markers in CRC, carcinoembryonic antigen (CEA) and carbohydrate antigen 19 − 9 (CA19-9), also dramatically slipped to the normal level (Fig. 2C), which indicated a PR. Stable disease (SD) was observed in August 2021, with a 4% decrease in the size of liver metastases compared to last detection with no obvious increase in the level of CEA and CA19-9 (Fig. 2B and C), however, the allele frequencies (AFs) of ctDNA alterations in plasma samples were dramatically elevated (Fig. 2D and Table 1). One month later, the tumor size increased by 30% compared to last month with an obvious increase in CEA and CA19-9 (Fig. 2B and C), which indicated a PD. Due to the occurrence of KIF5B-RET fusion (MAF = 18.5%), we recommended the use of pralsetinib, a selective RET inhibitor, but the patient refused. Then, the fourth-line chemotherapy with XELOX and bevacizumab was treated. Two months later, the tumor size increased by 21% (Fig. 2B). Unfortunately, he died of hepatic failure later.
{kind=link}