Epidemiological and clinical characteristics upon development of ARDS
As shown in Table 1, patients with COVID-19 were older than those with H1N1 influenza (median age: 56 vs. 43 years). None of the patients with H1N1 influenza (residents of Xiamen City) had any underlying diseases, whereas patients with COVID-19 had various underlying diseases, such as atrial fibrillation (n = 1), hypertension and obstructive sleep apnea syndrome (n = 1), diabetes (n = 1), diabetes and hypertension (n = 1), coronary artery disease and hypertension (n = 1), and malignancy (n = 1).
Five patients with COVID-19 were from Hubei province, and one was from Quanzhou City (Fujian province). Patients with H1N1 influenza had neither a recent travel history nor any family-based clusters of cases. The seven patients with COVID-19 had a clustered onset within a family.
Patients with COVID-19 presented with a significantly longer period from the onset of symptoms to ARDS development (7 vs. 4 days) and longer duration of stay in the RICU (mean, 18 vs. 14 days) than those with H1N1 influenza.
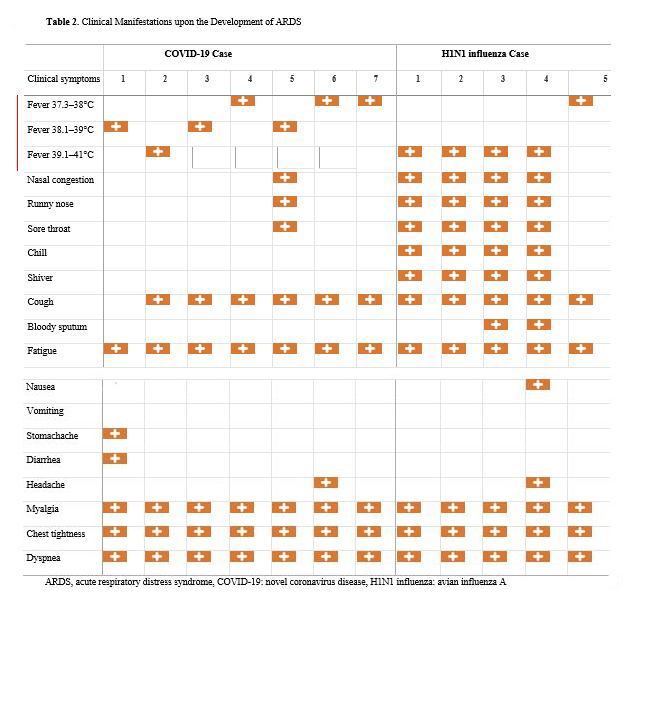
Clinical manifestations upon development of ARDS
Fever was the most common symptom, and low-to-moderate fever was significantly more common in patients with COVID-19 than in those with H1N1 influenza (85.7% vs. 20.0%). Upper respiratory tract symptoms were significantly less common in patients with COVID-19 than in those with H1N1 influenza (14.3% vs. 80.0%); however, lower respiratory tract symptoms (including cough, chest tightness, and dyspnea) were exhibited by all patients in both groups. Hemoptysis was documented in two patients with H1N1 influenza but in none of the patients with COVID-19. Gastrointestinal tract symptoms were equally rare (Figure 1).
Laboratory investigations upon development of ARDS
In the ARDS stage, patients with COVID-19 were more likely to have abnormal coagulation than patients with H1N1 influenza, such as increased D-dimer levels (100.0% vs. 20.0%). However, patients with H1N1 were more likely to have abnormal cardiac function, such as increased myocardial injury markers (troponin I, 80.0% vs. 14.3%) and increased heart failure indicators (brain natriuretic peptide, 80.0% vs. 14.3%) than patients with COVID-19. Leukopenia, decreased albumin levels, and elevated C-reactive protein levels were common in both groups, as were lymphopenia and elevated serum transaminase levels (which occurred in all patients). In addition, hypoxemia was recorded in all patients (Table 2).
Blood culture results in all patients were negative. Only one case tested positive for mycoplasma antibodies (titer, 1:640). Of the five patients with H1N1 influenza, two cases tested positive for Aspergillusfumigatus in galactomannan assays of bronchoalveolar lavage fluid.
Imaging characteristics
Computed tomography (CT) imaging showed that all patients with COVID-19 had multiple, bilateral lung lesions. In all cases, the lesions had a multi-lobar, multi-segmental distribution pattern (overlap between subpleural and lobular cores). Two cases showed ground-glass opacities only, while five cases had ground-glass opacities combined with consolidation. In all cases, there were nodular and patchy-type lesions. We also noted pleural parallel sign (6) in five cases, the fine-grid sign in six cases, the bronchogram sign in five cases, the vascular thickening sign in five cases, bronchiectasis in three cases, and the halo sign in two cases. There was a single case with anti-halo sign, one case with pleural effusion, and one case with pulmonary bulb. Representative images of patients with COVID-19 are shown in Figure 2.
On chest CT, all patients with H1N1 influenza had multiple lung lesions, all of which were diffusely distributed along the bronchial vascular bundle. All were ground-glass opacities with consolidation. All five cases showed bronchogram signs, three cases showed central leaflet nodules, three cases had a thickened leaflet septum and fine-mesh sign, and three cases presented with pleural effusion. Figure 3 shows the representative CT images of a patient with H1N1 influenza.
Treatment and prognosis
Antiviral drugs were initiated in all patients. Patients with COVID-19 received a-interferon nebulization, lopinavir/ritonavir, arbidol, ribavirin, and chloroquine phosphate according to the 4th-7th edition of the Pilot Program for the Diagnosis and Treatment of Novel Coronavirus Pneumonia (7-11). Patients with H1N1 influenza received systemic oseltamivir according to the Influenza Diagnosis and Treatment Plan 2019 Edition (12). Gamma immunoglobulin and anti-coagulation therapy were initiated in patients with COVID-19, but only for a single patient with H1N1 influenza.
Nasal high-flow humidified oxygen therapy was initiated in four patients with COVID-19 (all had mild ARDS) and three patients with H1N1 (with mild-to-moderate ARDS). Alternating use of nasal high-flow humidifying oxygen therapy and non-invasive ventilator- assisted ventilation was initiated in three patients with COVID-19 due to moderate-to-severe ARDS, but in none of the patients with H1N1 influenza. Moreover, tracheal intubation with ventilator-assisted ventilation was initiated in two patients with H1N1 influenza (with severe ARDS), but in none of the patients with COVID-19.
Septic shock, thromboembolism, and renal insufficiency were absent in both groups. All patients had acquired pneumonia and abnormal liver function. Pneumothorax and mediastinal emphysema were found in a single patient with COVID-19, while gastrointestinal bleeding occurred in a case in each group. Myocardial damage and cardiac dysfunction were more common in the H1N1 group than in the COVID-19 group (80.0% vs 14.3%). Overall, patients with COVID-19 achieved viral assay conversion from clinical diagnosis in a significantly longer duration as compared with the patients with H1N1 influenza.
Furthermore, the duration of hypoxemia as well as the duration of stay in the RICU was longer in patients with COVID-19 (Table 3). None of the patients died throughout the course of our study due to timely clinical interventions.
{kind=link}