In recent years, the study of the relationship between pelvic floor dysfunction and functional constipation has become a focus of research [10]. In the past, pelvic floor dyssynergia-type constipation was attributed to rectal protrusion and rectal intussusception and collectively called pelvic floor dysfunction syndrome. According to clinical experience, the postoperative effect in most patients is still not satisfactory due constipation recurrence [11], regardless of position of rectal mucosa suspension, range of tissue removal or enhanced repair of local muscle tissue. Due to the continuous development of three-dimensional ultrasonography techniques, this method has been increasingly applied to pelvic floor imaging [12]. The structures of the puborectalis muscle can be accurately assessed by three-dimensional perineal ultrasonography, which is convenient and non-invasive. The anatomical structures can be measured in the pubic symphysis, bilateral pubic ramus and medial and posterior edges of the puborectalis muscle [13,14]. Based on many clinical observations and data measurements, this study has shown that the puborectalis thickness at the 6 o’clock position (with patients in a lithotomy position) is an important factor. This study suggests that changes in the puborectalis angle and thickness may be important contributors to pelvic floor dyssynergia-type constipation.
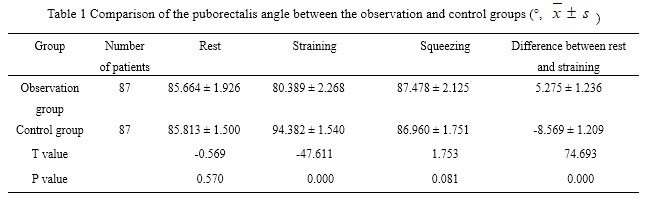
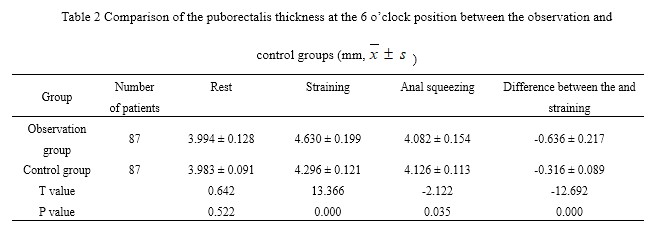
The puborectalis muscle is a striated muscle comprised of strip-shaped muscular fibres. The puborectalis muscle originates from the lower part of the pubic symphysis and is adjacent to the pubis. It extends posterior-inferiorly around the vagina or the prostate and merges to form an intact muscle behind the anorectal junction to retract the anorectal junction anteriorly to form an anorectal angle. The puborectalis muscle is a powerful “U”-shaped “sling” and the most powerful part of the levator ani muscle [15,16]. The puborectalis pubococcygeus, and iliococcygeal muscles form the majority of the levator plate [17]. The puborectalis muscle is more important than the pubococcygeus muscle and the iliococcygeal muscle. Previously, the anorectal angle and levator plate were considered to be good parameters to evaluate the pelvic floor structure [18],which plays an important role in defecation. However, this study suggested that the puborectalis muscle plays a decisive role in the evaluation of the pelvic floor structure. In normal defecation, the puborectalis muscle relaxes (i.e., increased puborectalis thickness), and the anorectal junction moves to the dorsal side in the sagittal plane to enlarge the anorectal angle and complete defecation. In contrast, in patients with pelvic floor dyssynergia-type constipation, the muscle movements are in the opposite direction [19]. In the 68 patients in the observation group, three-dimensional ultrasonography showed that the puborectalis angle was larger at rest than during straining. In the 67 patients in the control group, the puborectalis angle was smaller at rest than during straining, and only one patient had a larger puborectalis angle at rest than during straining. The difference in the puborectalis thickness between rest and straining was smaller in the observation group than in the control group. Although the puborectalis angle is larger at rest than during straining, the puborectalis thickness at the 6 o’clock position is smaller at rest than during straining.
In females, the pelvic floor hiatus may be injured during vaginal delivery [20]. In the observation group, three-dimensional ultrasonography showed a hypoechoic area in the right aspect of the puborectalis muscle in multiparas, which may be the consequence of changes or avulsion in pelvic floor tissue caused by obstetric procedures. Studies have shown that nearly half of women with a history of vaginal delivery have anatomical changes in the puborectalis muscle [21, 22]. A study by Serdar et al. [23] found that maternal overwork, oversized head circumference and an overweight of foetus can lead to puborectalis muscle injury, which causes changes in the pelvic hiatus, deformation of muscular fibres and muscle tone decline. In the observation group, three-dimensional ultrasonography showed that the puborectalis muscle is discontinuous in some patients. This discontinuation is more common in the junction of the pubic symphysis and the right aspect of the puborectalis muscle [24]. Thus, the left and right sides of the anorectal junction were unevenly affected during defecation. The left aspect of the puborectalis muscle produces excessive retraction at the anorectal junction. This prevents the puborectalis angle from expanding, and the puborectalis muscle is unable to be completely relaxed. As a consequence, varying degrees of pelvic floor dyssynergia-type constipation may occur [10]. This study suggests that pregnancy or changes in puborectalis muscle continuity can cause changes in the puborectalis angle and puborectalis thickness at the 6 o’clock position when patients are in a lithotomy position. Moreover, ageing is associated with degeneration and loosening of the pelvic floor support structures. Thus, the elasticity, extensibility, excitability and conductivity of the puborectalis muscle fibres are greatly reduced with ageing [17]. The anteroposterior diameter of the pelvic floor hiatus cannot be shortened, and the transverse diameter cannot be elongated accordingly. The differences in the puborectalis angle and the puborectalis thickness at the 6 o’clock position (with patients in a lithotomy position) between rest and straining were also increased. Follow-up of patients with constipation in this study showed that the increased differences in the puborectalis angle and the puborectalis thickness at the 6 o’clock position are associated with worsening symptoms of pelvic floor dyssynergia-type constipation (see Figures 3 and 4).
This study used three-dimensional ultrasonography to observe the changes in the shape and function of the puborectalis angle as well as changes in the puborectalis thickness at the 6 o’clock position with patients in the lithotomy position during rest, straining and squeezing. The results showed that the puborectalis angle decreased during straining of the pelvic floor structures in patients with pelvic floor dyssynergia-type constipation, and a smaller angle was associated with more serious symptoms of pelvic floor dyssynergia-type constipation. The puborectalis thickness at the 6 o’clock position is increased during straining, and the greater difference from that at rest is associated with more severe symptoms of pelvic floor dyssynergia-type constipation. Three-dimensional ultrasonography also has its limitations and is susceptible to more factors than two-dimensional ultrasonography. MRI can clearly show the pelvic floor structures.
{kind=link}
{kind=link}