Immunohistochemical assay and cellular immunochemical assay to verify the high expression of FAP in OLK
FAP is a homodimeric integrative membrane gelatinase belonging to the serine protease family and is capable of cleaving the proline backbone of peptides and proteins[38, 39].Several studies have shown that FAP is expressed in tumor cells of epithelial origin like in breast, pancreatic, gastric, rectal, and cervical cancers, and OSCC, but not in normal adult tissues[40–42].Wang et al. showed that FAP downregulation inhibits cell proliferation and metastasis in OSCC, which suggests that FAP plays an important role in OSCC development[43].Numerous epidemiological and molecular biology studies have shown that inflammation significantly increases the risk of cancer[44].Progression from OLK to OSCC involves a complex inflammatory process[45]. Furthermore, Cai et al. showed that FAP expression is elevated in the tumor microenvironment and inflammatory settings[46].Based on the above, we hypothesized that FAP is highly expressed in OLK, and the sequencing results of Debodipta Das confirmed our conjecture that FAP is highly expressed in OLK. Next, we verify this result by experimental areas.
In the present study, we analyzed FAP expression levels in OLK and normal tissue sections via immunohistochemistry, and OLK tissues showed higher FAP expression than normal oral mucosa tissues. Notably, FAP was located in the epithelial layer and part of the mesenchyme of OLK tissue and localized mainly in the cytoplasm (Fig. 1a and b). The FAP expression levels in DOK cells and HOK normal cells were analyzed by cellular immunochemistry ,and DOK cells showed higher FAP expression than HOK cells, with FAP located in the cytoplasm of DOK cells (Fig. 1c and d). These results suggest that FAP is highly expressed in OLK.
Synthesis And Characterization Of Cgpf
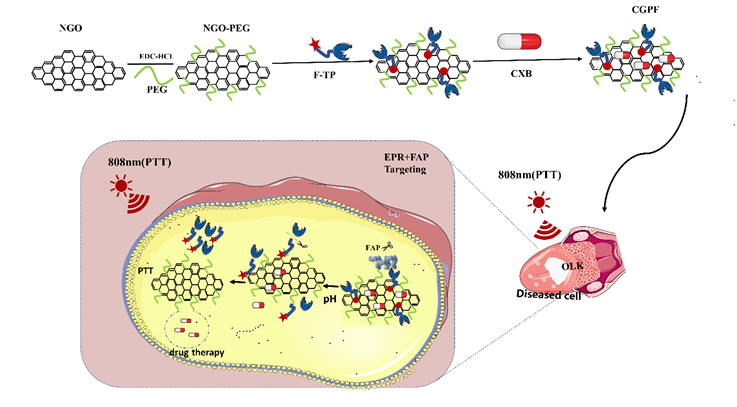
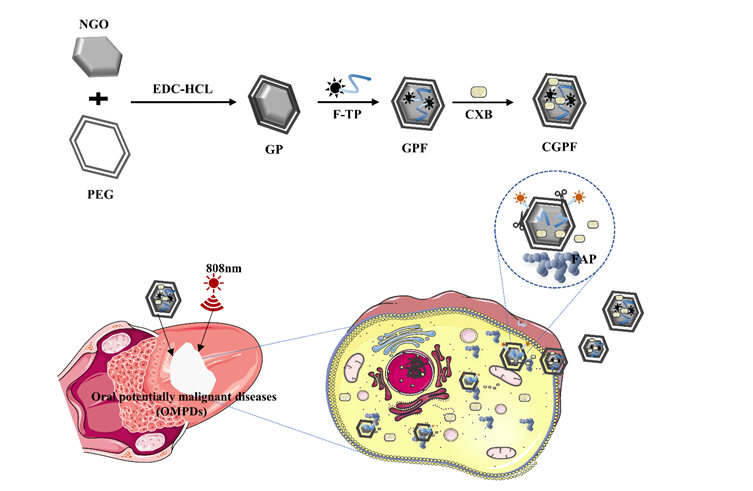
To synthesize CGPF, PEGylated NGO was synthesized by modifying the NGO with PEG by following the prevailing method in the literature. Subsequently, the NGO-PEG was bound to the peptide chain with a fluorophore attached, and CXB was added to construct a nano-drug delivery system. On exposure to UV rays, NGO had a maximum absorption peak at 230 nm, which is the characteristic absorption peak of C = O. After modifying with PEG, the NGO-PEG had a maximum absorption peak at 240 nm owing to the reduction of NGO by PEG through an amide reaction, which shifted the absorption peak to the right. The F-TP had a clear UV absorption peak at 495 nm, and the GPF showed the characteristic F-TP peak at 495 nm, indicating the successful binding of F-TP to NGO-PEG. There were clear absorption peaks at 254 nm for both CXB and CGPF. Therefore, CXB can be considered to have successfully bound to GPF (Fig. 2a).
In addition, we characterized the probe using FTIR spectroscopy (Fig. 2b). NGO-PEG had a C-O-C stretching vibration peak at 946 cm− 1, C-N stretching vibration peak at 1103 cm− 1, and C = O stretching vibration peak in the amide bond region at 1511 cm− 1. This indicates that the NGO -COOH group underwent an amide reaction with the terminal amino group of PEG(NH2)2. New peaks were observed at 1251 cm− 1. These changes in the chemical bonding vibrational peaks confirm that NGO-PEG formed bonds with F-TP through hydrogen and π–π bond interactions. The 1243cm− 1,2765cm− 1and 3606cm− 1 peaks were caused by benzene rings and other functional groups indicating that the nano-drug delivery system was successfully fabricated.
Zeta potential analysis was performed to verify NGO modification by PEG and the loading of F-TP and CXB. The negative potential of NGO-PEG (-22 mV) was lower than that of NGO (-27.3 mV) owing to the reaction between the negative NGO carboxyl group and the PEG amino group. The zeta potential reduced to -21 mV upon attachment of the FAP-targeting peptide and to -20.4 upon CXB attachment (Fig. 2c). The change in potential indicates the successful synthesis of the nano-drug delivery system.
The morphologies of the studied nanoparticles (NGO, NGO-PEG, GPF, and CGPF) were investigated using transmission electron microscopy (Fig. 2d). Notably, the thin and transparent NGO sheets had a relatively large and smooth surface. After polyethylene glycolization, the nano-sheet surfaces appeared corrugated that facilitated functionalization of the nanoparticles with drugs or other bioactive molecules. After loading F-TP and CXB, the NGO-PEG sheet layers had different shapes.
The NGO, NGO-PEG, GPF, and CGPF hydrated particle sizes were determined using DLS. The particles were 345.6, 122.7, 140.5, and 179.5 nm in diameter, respectively indicating that the NGO particle size was effectively reduced following PEG modification. Furthermore, the particle size increased following FAP-targeting peptide and CXB attachment. In addition, the particle size reduced after polyethylene glycolization, as the size range of NGO particles was 295–459 nm, while that of NGO-PEG particles was 106–142 nm (Fig. 2e).
Stability Experiments
Because of poor hydrophilicity of NGO, we used PEG to enhance its stability. As shown in Fig. 2f, in PBS containing NGO, a clear precipitate was observed after 1 day of resting (f-①). In contrast, NGO-PEG and CGPF were uniformly dispersed in PBS and were stable even after 6 days (f-②③). To simulate the blood environment in vivo, we examined nanocomposite stability in 10% FBS. As shown in Fig. 2f, a large amount of precipitate was observed in 10% FBS containing NGO after 1 day (f-①). In contrast to NGO, NGO-PEG and CGPF remained stably dispersed in 10% FBS without precipitation(f-②③).
Fluorescence Quenching And Recovery
The excitation wavelength of FITC is 495 nm, and the fluorescence quenching experiment showed that when the concentration of NGO was 0.1 mg/mL, the peak fluorescence absorption of FITC dropped to 0. This indicates that 0.1 mg/mL of NGO can quench the fluorescence coupled to 10 µg/mL of the FAP target peptide (Fig. 3a). To investigate if FITC can dislodge from the NGO carrier to restore florescence upon encountering the target molecule and thus act as a fluorescence “switch,” we analyzed the recovery of fluorescence intensity after incubation of GPF containing different concentrations of NGO with DOK cells for 40 min by flow cytometry.As shown in Fig. 3b, despite the strong fluorescence quenching effect of 0.1 mg/mL NGO, equal amounts of fluorescence were detected in all five experimental groups when compared with that in the control group. The amount of fluorescence detected in the experimental group was close to that in the control group. Taken together, these results indicate that FITC can shed from GPF to localize to OLK after the probe encounters the target molecule FAP.
Drug Loading And Release Experiments
The UV-Vis absorbance of CXB was measured at 254 nm, and the standard curve was plotted (Fig. 3c). The linear regression equation of CXB was:
A = 0.02683C + 0.09927 (R2 = 0.98156),
where A is the UV-Vis absorbance of CXB at 254 nm and C is the concentration of CXB (µg/mL), and R2 = 0.98156 indicates a good linear relationship and plausible standard curve. The corresponding CXB concentration was derived from the above linear regression equation, and the drug loading rate of the nano-targeted probe was calculated as 38.82% according to Eq. 1.
Owing to the difference in the microenvironments between inflammatory and normal tissues, we set up different pH values to simulate each tissue. The drug release properties of the nano-delivery system were evaluated in PBS solutions at pH 7.4, 6.5 and 5.5.The CXB release profiles from the nano-drug-loaded system at different pH values are shown in Fig. 3d. CXB exhibited a sustained in vitro release from the nano-carrier system and showed some degree of pH sensitivity. The amount and rate of drug release at pH 5.5 was the highest followed by that at pH 6.5 and pH 7.4, at the same time interval. The nano-carrier system eventually released 65.02% and 81.96% of CXB at pH 6.5 and 5.5, respectively, but at pH 7.4, only 51.47% was released. Taken together, these results suggest that the nano-drug delivery system is pH-sensitive and can selectively release CXB. The results of this experiment suggest that our constructed CGPF is sufficiently stable to prevent it from releasing the drug before it reaches the lesion site.Our results are in good agreement with those of previous studies describing similar pH-responsive drug-release behaviors[47].
In Vitro Photothermal Effect
Figure 4 In vitro photothermal effect. (a) Photothermal profile images of PBS, NGO, NGO-PEG, GPF, and CGPF under 808 nm radiation. (b) Photothermal profile images of CGPF aqueous solution with different concentrations under 808 nm radiation. (c) Photothermal profile images of CGPF aqueous solution with different power under 808 nm radiation. (d) Photothermal performance of CGPF over five laser on/off cycles
Prior studies have shown that graphene oxides exhibit a photothermal effect and can convert absorbed light energy into heat energy under near-infrared light irradiation, resulting in an increase in the temperature of the surrounding environment. To determine whether NGO-PEG also has a photothermal therapeutic effect, near-infrared light (808 nm, 1.0 W/cm2) was used to irradiate the NGO, NGO-PEG, GPF, and CGPF solutions, while PBS was used as a control. As shown in Fig. 4a, the NGO, NGO-PEG, GPF, and CGPF solutions warmed rapidly under laser irradiation, while PBS showed essentially no significant warming. The temperature of the CGPF solution increased sharply with increasing time and concentration (Fig. 4b). At the same concentration, the temperature of the CGPF solution increased with increasing power of irradiation (Fig. 4c). The infrared (IR) thermal images confirmed similar results. Notably, no significant decay was detected in the temperature increase after five heating and cooling cycles, indicating excellent photothermal stability (Fig. 4d). These results indicate that GO modification by PEG does not destroy the photothermal effect of the material itself. Owing to the effective restoration of π–π conjugation via chemical reduction, the energy absorbed by the reduced GO nanomaterials can be rapidly converted to higher thermal energy. The GO photothermal performance improved after modification by PEG, and the radiothermal effect of CGPF under irradiation with near-infrared light caused a significant increase in the temperature of the surrounding environment, which is of great significance for the photothermal treatment of white spots.
In Vitro Cytotoxicity
Prior to in vitro evaluation of the synergistic therapeutic properties of CGPF, its cytotoxicity and therapeutic feasibility were investigated using standard CCK8 assays. The cytotoxicity of NGO, PEG, NGO-PEG, F-TP, GPF, CXB, and CGPF in DOK and HOK cells was assessed. Twenty-four hours post-treatment, we observed that in the concentration range studied, NGO-PEG exhibited lower cytotoxicity than NGO in DOK and HOK cells, and NGO-PEG and GPF had no significant effect on DOK and HOK cell proliferation. In addition, we found that cell viability of the CGPF group was significantly lower than that of the NGO-PEG and GPF groups. However, cell viability was higher in the CGPF group than in the free CXB group at the same CXB concentration. The toxicity of free CXB in DOK cells was much higher than that in HOK cells (Fig. 5a). Under photothermal conditions, the cell viability of the NGO, NGO-PEG, GPF, and CGPF groups decreased relative to that of the non-photothermal group, especially the CGPF group, which showed a significant decrease in cell viability (Fig. 5b). This can be explained as follows: (1) NIR radiation kills DOK cells and promotes cell membrane permeability and increases nanomaterial internalization, accelerating drug release in DOK cells and enhancing medication effects; (2) NIR laser-assisted thermal therapy destroys drug-resistant DOK cells and helps promote accumulation of CXB in the nucleus, thereby improving medication efficacy. In addition, cell viability of the CGPF group was much higher than that of the free CXB group for the same CXB concentration, which may be explained by the incomplete release of CXB at pH = 7.4.
Subsequently, DOK cell viability tests were performed under different pH conditions, and the results are shown in Fig. 5c. The cell viability of the control and CXB groups did not change significantly at different pH values, whereas the viability of the CGPF group decreased with the pH of the culture medium. This further suggests that the pH of the culture environment affects drug release and thus cell viability and that the acidic pH of the inflammatory environment surrounding the leukoplakia tissue limits the effective release range of our drugs and reduces their toxicity to normal cells and tissues.
Cellular Uptake Experiments
To verify the targeting of F-TP, the FAP-responsive properties of CGPF at the cellular level, and whether the nanoparticles could be effectively administered, laser confocal scanning microscopy experiments were performed to assess the uptake of the F-TP, GPF, and CGPF in DOK and HOK cells. Blue fluorescence (excitation, 460 nm) was used to identify the nuclei of DOK and HOK cells, while the red channel (excitation, 490 nm) represents the FITC fluorescence signal. As shown in Fig. 5e, the FITC fluorescent signal colocalized to the red signal. F-TP were observed on the cell membrane and cytoplasm of DOK cells, consistent with the FAP expression profile. In the negative control, no red fluorescence signal was observed in HOK cells. In summary, the F-TP, GPF, and CGPF showed high binding to FAP expressed in DOK, which could be taken up by DOK cells, and the FAP-specific peptide on CGPF was cleaved to activate FITC.
Additional time-dependent assays of the F-TP, GPF, and CGPF were performed using DOK cells. The results showed that the uptake of the F-TP, GPF, and CGPF by DOK cells was time-dependent. The cellular uptake of the F-TP and GPF did not differ significantly, indicating that NGO had no effect on F-TP uptake. Cell uptake rates in F-TP and GPF groups were 82.235% and 83.77% at 30 min and 85.08% and 83.9% 120 min, respectively. The cellular uptake rate of CGPF was 80.22% at 30 min; at 120 min, it decreased to 64.85% (Fig. 5d). This is owing to the decrease in the uptake rate as a result of cell death due to drug release after the nano-drug delivery system was internalized into the cells.
Successful Establishment Of A Mouse Olk Model
4NQO is an aromatic amine heterocyclic compound that is extensively recognized as a chemical precursor carcinogen[48].Studies have shown that 4NQO can help develop pre-cancerous or cancer models by inducing intracellular oxidative stress, DNA endocytosis, mutagenesis, and tumor initiation[49, 50].The 4NQO-induced pre-cancerous lesion model has a multi-stage dynamic continuum, from normal oral mucosa to OLK to OSCC, with pathological stages that undergo hyperplasia, heterogeneous hyperplasia (mild, moderate, and severe), carcinoma in situ, and invasive squamous cell carcinoma[51].This model closely mimics the heterogeneous oncogenic proliferation process in the human oral cavity and is suitable for studying the specific OLK oncogenic process for the development of biomarkers for early detection and epithelial cell transformation[52, 53].After 100 µg/mL 4NQO was administered via drinking water, all mice were anesthetized by injection of chloral hydrate at 8, 12, and 16 weeks[54].We observed the 4NQO-induced changes by pulling the tongues outward and selected the typical tissues for histopathological examination. At week 8, the mice had mild atrophy of the tongue papillae and a smooth white dorsum of the tongue, and HE staining showed a mild or normal heterogeneous lesion phenotype. At week 12, the dorsum of the tongue was rough and smooth, white plaque-like lesions appeared on the tongue tissue, and HE staining showed mild or moderate heterogeneous hyperplasia. Thereafter, all mice gradually developed inseparable white plaques. At week 16, they developed typical lesions similar to those in human OLK (Fig. 6). 4NQO has been shown to cause cancer in different sites of the oral cavity such as the dorsum of the tongue, ventral part of the tongue, palate, and esophagus. Many researchers have shown that lesions of the tongue occur almost 100% of the time, particularly in the dorsal mucosa of the tongue. In the present study, lesions were predominantly located on the dorsum of the tongue, with a few lesions located on the floor of the mouth or along the lateral edge of the tongue, which is consistent with previous reports. These findings indicate the successful establishment of an OLK mouse model, with no significant damage to the major organs by 4NQO, which can be used for further in vivo experiments.
In Vivo Biodistribution
Precise localization and optimal timing are essential for the successful synergistic treatment of leukoplakia. To assess the ability of FAP to activate fluorescence in vivo, F-TP and CGPF were injected intraperitoneally into mice, and the PBS group was used as a control. As shown, the activatable CGPF fluoresced rapidly and specifically at the white spots within 8 h, which helped distinguish the white areas from normal tissue. Interestingly, no detectable fluorescence was found in any other area without leukoplakia lesions owing to the initial fluorescence quenching of CGPF. Thereafter, the images showed gradual enhancement of FL signal in both F-TP-injected and CGPF-injected mice in the leukoplakic areas and reached a maximum 8 h post-injection. In contrast, no FL signal was observed in the control group 24 h after the PBS injection. This suggests that the F-TP and CGPF can be effectively delivered to white spots and that CGPF can be specifically activated by FAP. Subsequent in vitro FL imaging of the excised tongues and major organs of F-TP and CGPF-treated mice after 24 h clearly showed that fluorescence activation was visible at the white spot of the excised tongue and had a superior FL signal than the major organs (Fig. 7a). Notably, a weaker fluorescent signal was present in the isolated liver than in other organs, reflecting the major hepatic clearance process of F-TP and CGPF.
In Vivo Targeting And Photothermal Effects
Encouraged by the activatable NIR fluorescence imaging data, we next explored the feasibility of CGPF for NIR PTT in vivo, and the results provided the correct time point and location specificity for laser irradiation. CGPF and PBS were injected intraperitoneally into mice with white plaque lesions, and infrared thermography and temperature changes at the tumor site were monitored 5 min after NIR irradiation. Considering the threshold temperature for PTT (43°C), the high temperature of CGPF 8 h after administration far exceeded the requirement for thermotherapy to achieve an optimal photothermal treatment effect. Notably, lesion temperatures in the 6- and 24-h post-injection groups showed lower maximums than those in the 8-h post-injection groups owing to insufficient accumulation in the leukoplakic lesion sites. In contrast, PBS-treated mice showed only slight warming (Fig. 7b). With photothermal imaging guidance, we selected 8 h after injection as the appropriate time for synergistic treatment. Figure 7c and d show that the temperature of the oral white-spot site of mice irradiated with NIR for 5 min after 8 h of GPF and CGPF injection increased significantly, while the temperature of mice injected with PBS and CGP did not change significantly after irradiation. This is because PBS has no photothermal effect and CGP had a photothermal effect; however, the absence of F-TP prevented it from aggregating at the oral white-spot site in the mice.
In Vivo Therapeutic Effect And Safety Assessment Of Olk
To evaluate the in vivo therapeutic performance of CGPF in OLK, we selected 45 mice with typical white plaque lesions on the dorsal surface of the tongue and randomly divided them into nine groups (n = 5) for different treatments, with PBS-injected mice as negative controls. Changes in white plaques of the tongue were continuously monitored and recorded in each group for 1 month after the different treatments. Impressive leukoplakia suppression was achieved within 1 month after CGPF combined with 808-nm laser treatment, but not in the other groups, indicating that chemotherapy in synergy with PTT achieved better therapeutic effects than chemotherapy alone (Fig. 8a).
Interestingly, the CGPF + laser group showed almost complete eradication during the treatment period without any recurrence. In contrast, the CGPF and GPF + laser groups showed limited cancer suppression with partial improvement, indicating that neither drug treatment alone (CGPF) nor targeted material alone combined with laser treatment (GPF + laser) could achieve superior results than the targeted material delivery system combined with photothermal treatment (CGPF + laser). This may be owing to the graphene oxide structure, which allows CXB to make full contact with the lesion site. In the presence of the F-TP, the material and drug can accurately and rapidly reach the OLK lesion site with high FAP expression. This is similar to the specific recognition and binding of antigens to antibodies. Furthermore, when the CGPF successfully reached the lesion and achieved significant aggregation, excellent photothermal properties of NGO allowed laser irritation to rapidly warm the lesion, and when the photothermal temperature reached approximately 50℃, the lesion area experienced a significant effect. This explains why the treatment effect of CGPF + laser was better than that of CGPF or GPF + laser, while anisotropic hyperplasia in the CGP, CGP + laser, and CXB groups continued to deteriorate. We consider that in the absence of targeted peptides, the material delivery system or the drug alone cannot reach the lesion accurately and quickly, and only a small amount of the drug can work at the lesion after it is injected intraperitoneally into the systemic circulation, so the effect of the laser becomes very weak in these treatment groups. While the cancer in the GPF, PBS, and laser groups progressed, which again proved that the material or laser alone could not exert any therapeutic effect.
In summary, even though the targeted nano-delivery system achieved specific binding of the targeted peptide to the lesion site FAP, improving the contact area of the drug will provide better therapeutic effects,the treatment effect of CGPF alone was limited. In contrast,the targeting of CGPF provided good combined photothermal chemotherapy for the treatment of OLK, and the CGPF + laser treatment group achieve better results; its therapeutic effects were superior to those of CGPF, and it effectively inhibited the malignant development of OLK.
In addition, we did not use local injection in the experiment but used intraperitoneal injection for the following reasons: first, the local drug delivery method will be affected by factors such as saliva secretion and tongue movement, which will make the operation more difficult, and the stimulated saliva secretion will dilute the drug and eventually affect the therapeutic effect. Secondly, the number of injections will cause damage to the tongue and affect feeding, which further affects the efficacy of the drug. Thirdly, the injection itself is one of the stimulating factors, which may induce or aggravate the leukoplakia lesion, and the result has certain influence. Then again, our experiment successfully proved that the oral leukoplakia in mice was cured by intraperitoneal injection of CGPF, which indicates that our nano-targeting system CGPF has a good targeting effect and can make it gather well in the oral leukoplakia lesions to achieve the ideal treatment effect.
In addition to therapeutic effects, long-term safety of the material must be considered. Mitigating drug biotoxicity is essential for biomedical applications. Therefore, we investigated the biocompatibility of different materials using C57BL/6 mice. We continuously monitored and recorded weight changes in the mice during treatment. Notably, negligible body weight fluctuations were observed during treatment (Fig. 8b), and the material exhibited superior biosafety. To further confirm the treatment effect, tongue leukoplakia tissue was dissected at the end of treatment, and pathological changes were assessed through histological and immunohistochemical analyses. As shown in Fig. 8c, significant leukoplakia cell damage and diminished or absent anisotropic proliferation were observed in the CGPF + laser group, and partial leukoplakia cell damage and diminished anisotropic proliferation were observed in the CGPF and GPF + laser groups. In contrast, enhanced heterogeneous hyperplasia and cancerous lesions were observed in the CGP, CGP + laser, CXB, GPF, PBS, and laser groups. In addition, the experimental results showed that the expression of FAP, KI67 and p53 was highest in the control group, compared to a significant downregulation of FAP, KI67 and p53 expression after treatment with CGPF + laser. (Fig. 8d).
As expected, HE staining of the major organs (heart, liver, spleen, lung, and kidney) showed no significant histopathological damage or inflammation in any group (Fig. 8e). These results suggest that our targeted nano-drug delivery system combined with PTT significantly improved the therapeutic efficacy of OLK with a good biosafety profile.
{kind=link}
{kind=link}