The baseline information and the genetic profile of cholangiocarcinoma patients
A total of 43 patients were selected for this study. Detailed clinical information were displayed in Table 1. Among 43 patients, 5 patients were diagnosed with intrahepatic cholangiocarcinoma, 32 patients were diagnosed with extrahepatic cholangiocarcinoma, 5 patients were diagnosed with ampullary carcinoma, and 1 patient was diagnosed with pancreatic duct carcinoma..
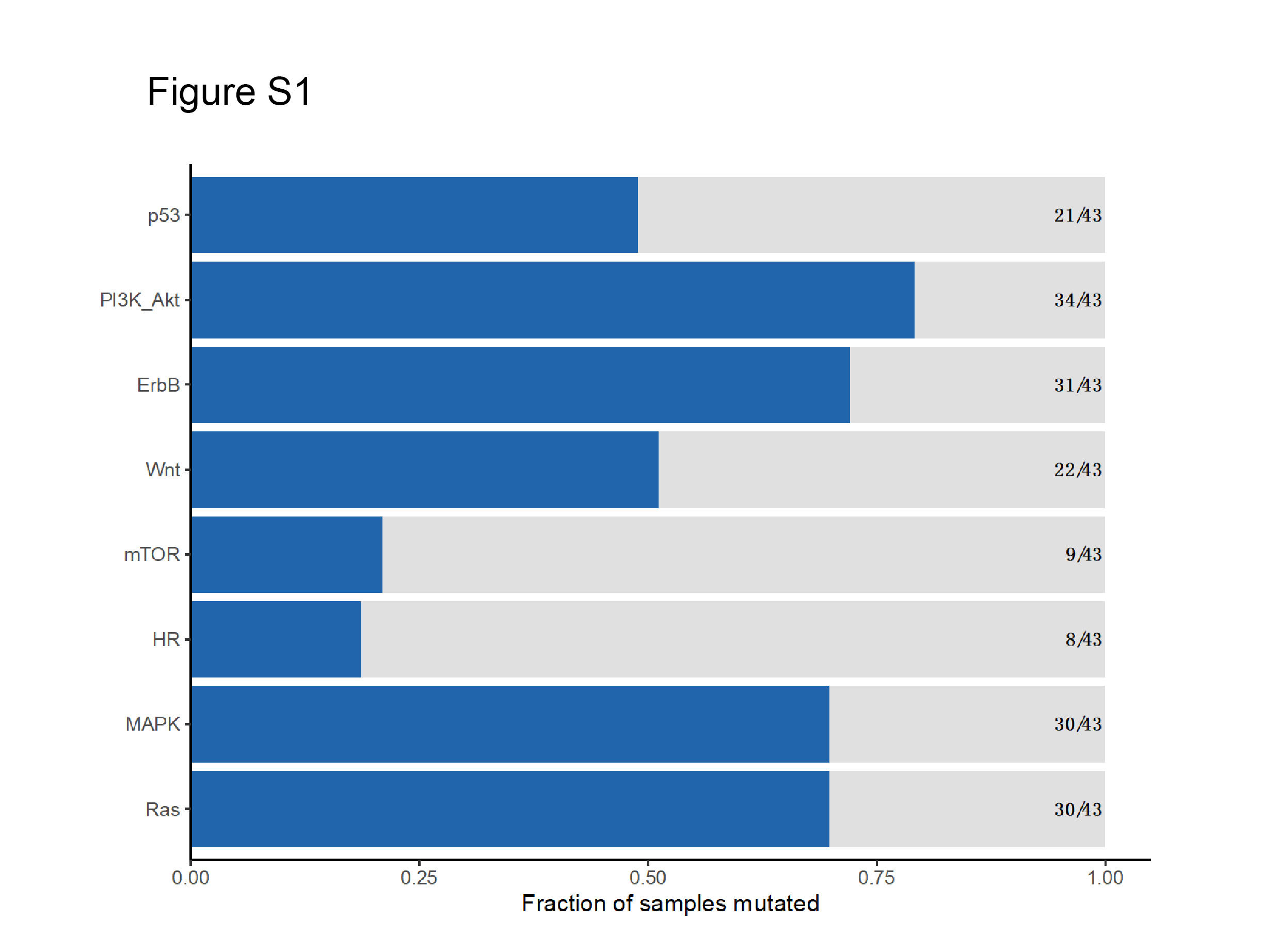
Besides, in the genetic analysis, a total of 8 kinds of genetic alterations were detected, including missense, copy number deletion, copy number amplification, indel, stop gained, frameshift, splice site, and gene fusion (Fig. 1A). Our data suggested that among 43 patients, gene alterations were observed in 38 patients, with a positive rate of 88.4%. The most commonly mutated genes included KRAS (44.2%), TP53 (37.2%), ARID1A (18.6%), SMAD4 (18.6%), CDKN2A (14.0%), BRAC2(11.6%), VEGFA (11.6%), KEAP1(9.3%), MYC (9.3%), and STK11(9.3%) (Fig. 1B). Only five patients harbor no somatic mutation. Among the top altered genes in our study, most high-frequency mutated genes are following previous sequencing results (Table 2). Of note, most mutations are enriched in PI3K/AKT, ERBB, MAPK, and RAS signaling ( see Additional file 2), indicating that these signaling might play essential roles in the pathological process of cholangiocarcinoma.
Table 2
Top mutated genes in cholangiocarcinoma in different cohorts.
| |
TCGA cohort (N = 36)
|
ICGC cohort (N = 489)
|
MSK cohort (N = 192)
|
Our study
(N = 43)
|
|
Top mutated genes
|
PBRM1(19.4%)
|
TP53 (35.3%)
|
IDH1
(24.6%)
|
KRAS (44.2%)
|
|
BAP1(19.4%)
|
ARID1A (19.2)
|
TP53
(23.6%)
|
TP53 (37.2%)
|
|
IDH1(13.9%)
|
KRAS (18.2%)
|
ARID1A(20.5%)
|
ARID1A (18.6%)
|
|
TTN(11.1%)
|
SMAD4 (14.4%)
|
BAP1(13.3%)
|
SMAD4(18.6%)
|
|
EPHA2(11.1%)
|
SYNE1(11.0%)
|
KRAS(11.8%)
|
CDKN2A (14%)
|
|
ARID1A(11.1%)
|
MUC16(10.6%)
|
PBRM1(10.3%)
|
BRCA2(11.6%)
|
|
DNAH5(11.1%)
|
LRP1B(9.4%)
|
SMAD4(8.2%)
|
VEGFA (11.6%)
|
|
KMT2C(11.1%)
|
BAP1(9.4%)
|
ATM(7.7%)
|
KEAP1(9.3%)
|
|
TP53(11.1%)
|
FSIP2(8.9%)
|
PIK3CA (6.7%)
|
MYC (9.3%)
|
|
ADGRV1(8.3%)
|
EPHA2(8.6%)
|
KMT2C (6.7%)
|
STK11(9.3)
|
In cholangiocarcinoma, the genetic mutation is closely associated with the clinicopathological feature.
After depicting the genomic profiling of cholangiocarcinoma, we investigated the associations between the genetic mutation and clinicopathological features (Figure 2A). At first, we investigated the correlations among the clinicopathological features, which turned out that patients with extrahepatic cholangiocarcinoma had a higher rate of lymph node metastasis, and all intrahepatic cholangiocarcinoma patients were female (Figure 2B). Besides, distal cholangiocarcinoma is more common in male patients and male patients are diagnosed at earlier ages (Figure 2C). In terms of the clinical significance of the Ki67 index, our data indicated that patients with a higher Ki67 index have a higher rate of lymph node metastasis. As for the correlation between the Ki67 index and tumor site, it was observed that distal cholangiocarcinoma had a higher Ki67 index than other subtypes of cholangiocarcinoma (P=0.002; Figure 2D). Next, we analysis the correlation between the TNM stage and tumor site, which suggested that patients with distal cholangiocarcinoma were diagnostic with a relative earlier stage (Figure 2E). Moreover, we found that the CA19-9 level was positively related with the rate of organ invasion, suggesting that CA19-9 level was associated with the tumor invasion capacity in cholangiocarcinoma (Figure 2F).
As for the correlation between the gene mutation and the clinical information (Figure 3A), we found that the STK11 mutation was related to the tumor site, this mutation was mainly observed in the intrahepatic cholangiocarcinoma. Besides, we found out that TP53 mutation was associated with a low division degree (P=0.040)(Figure 3B). Moreover, we observed that ERBB2 mutation was closely related to the organ invasion and TNM stage(Figure 3C). These results suggested that these mutations might contribute to the pathological process of cholangiocarcinoma. Moreover, the correlations between the genetic mutations were presented in Figure 3D, reflecting the complex correlation between genetic mutations.
The prognostic significance of specific genetic mutation
We further investigated the prognostic value-specific genetic mutation, especially commonly altered genes, including ARID1A, BRCA2, CDKN2A, ERBB2, ERBB3, KEAP1, KRAS, MET, MSH6, MYC, NRAS, RET, RNF43, SMAD4, STK11, TP53 and VEGFA (Figure 4A). Kaplan-Meier analysis was applied to evaluate the prognostic significance of these genes, and it turned out that ERBB3, MYC, STK11, TP53, and KRAS were related to the prognosis of these patients. To be specific, patients with ERBB3 mutation have shorter RFS (P=0.007, Hazard ration (HR) [95% Confidence interval (CI)] =7.00 [1.34-36.55]) (Figure 4B). Besides, patients with MYC mutation have worse RFS (P=0.007, HR [95%CI] = 6.23 [1.37-28.39]) and OS (P=0.010, HR [95%CI] =7.57 [1.24-46.14]) (Figure 4C). Meanwhile, patients with STK11 mutation have worse RFS (P<0.001, HR [95%CI] =29.18 [2.94-289.77]) and OS (P<0.001, HR (95%CI) =18.79 [3.33-106.15]) (Figure 4D). The mutation types of TP53 and KRAS genes were presented in Figure 4E. Of note, patients with TP53 mutation have worse RFS and OS (Figure 4F). A similar result was observed for the patients with KRAS mutation (Figure 4G). Taken together, all these data indicated that the genetic feature could serve as a potential prognostic biomarker for cholangiocarcinoma patients.
PAT analysis
Massive efforts have been implicated to translate genomic alterations into actionable targets. In this study, we defined PATs as genomic alterations classified by the scoring system of OncoKB (tier ≤level-3A) or the ESCAT (tier≤II-B), as their matched therapies have shown compelling clinical efficacy in treating BTC and other tumors. In this study, we propose 19 genes as PATs in BTC. In this context, 34 (71.4%) patients harbored at least one PAT(Figure 5A). The most commonly detected PAT is the KRAS mutation (23.8%), followed by the TP53 mutation (20.2%), and the missense mutation was the most commonly detected mutation type (48.8%) (Figure 5B). These data indicated that this 168-gene panel could provide clues for the targeted therapy of cholangiocarcinoma patients.
{kind=link}