This study showed that a higher vitamin K status at baseline was associated with decreased LVMI after 7.6 years of follow-up, only among women. Vitamin K status was not associated with other cardiac measures. Vitamin K intake was not associated with cardiac structure and function.
This study is the first prospective study investigating the association between vitamin K status and cardiac structure and function measures. Our results are in line with earlier cross-sectional studies showing that a low vitamin K status was associated with reduced systolic function (18) or a higher prevalence of diastolic dysfunction (20). However, in our study, a higher vitamin K status was associated with LVMI only among women and not among men, but such effect modification by sex was not investigated in earlier studies. We didn’t observe any association between vitamin K status and LVEF or LAVI.
Nevertheless, the studies that found an associations between vitamin K status and systolic or diastolic function were performed in populations with different features than those of the present study, the participants being affected by valvular diseases, HF or cardiomyopathy.
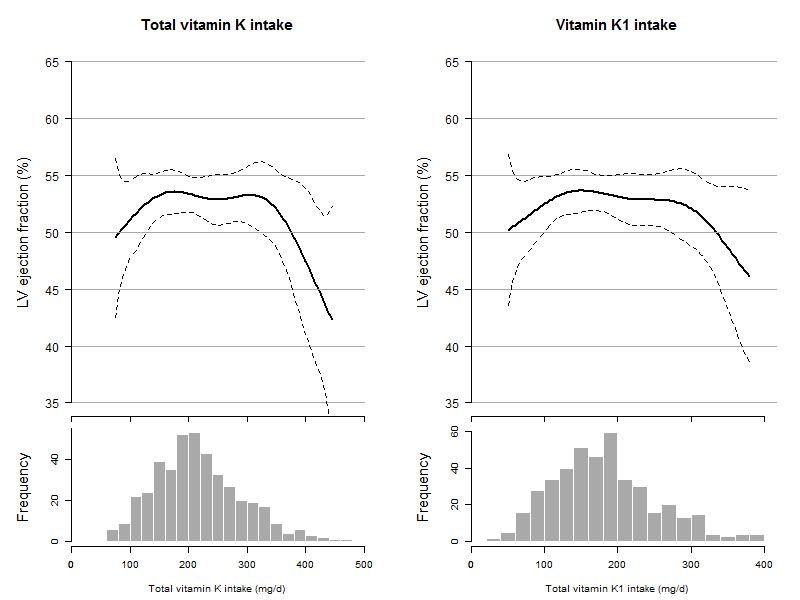
Despite this association between vitamin K status and LVMI, we could not detect any clear associations between any of the forms of vitamin K intake and cardiac measures. This is inconsistent with the study by Eshak et al. showing that a higher vitamin K intake was associated with a 37% reduced risk of HF mortality after 19 years of follow-up among Japanese women (17). The inconsistent findings between both studies could be due to the relatively low sample size of our study combined with the relatively low validity of the FFQ to accurately assess vitamin K intake. For LAVI and LVEF, we observed significant non-linear associations with several forms of vitamin K intake. These associations showed slightly, but non-significantly higher LVEF and LAVI in the second and third quartile of vitamin K intake.
The underlying mechanism of vitamin K status and intake, cardiac structure and function and risk of HF may be explained by improved arterial stiffness with increased vitamin K intake and status. Vitamin K functions as a co-factor to carboxylate MGP, a potent inhibitor of vascular calcification. Animal experiments indeed showed that antagonism of vitamin K leads to vascular calcification, in particular of the medial layer of the arteries (31). Medial calcification leads to vascular stiffness (32, 33), which in turn is consistently associated with diastolic dysfunction (34). In fact, vascular stiffness may increase the systolic load on the ventricles and decrease aortic pressure during diastole, thereby increasing pulse pressure (35). Increased pulse pressure increases myocardial oxygen demand during systole and is associated with LV hypertrophy. These changes can lead to impaired relaxation and eventually LV diastolic dysfunction and HFpEF (36). Indeed, earlier studies have shown vitamin K status to be associated with increased arterial stiffness (19, 37, 38). One possible explanation of why in our study vitamin K status affected LV structure only in women, is that women, especially after menopause, seem to be more prone to develop LV hypertrophy in response to pressure overload compared to men. Consequently, the effect of vitamin K status on arterial stiffness and cardiac overload might manifest itself only in women [32].
Strengths of this study include its prospective design and detailed phenotyping of the participants, allowing to adjust for multiple confounders. However, certain limitations need to be addressed. First, the prospective associations may be biased due to the high loss to follow-up rates in this study. Although we observed similar associations in our analyses after inverse probability weighting, we cannot exclude some selection bias. Second, for the assessment of vitamin K intake we relied on self-reported data.
Although the FFQ was validated for the assessment of vitamin K intake, the relative validity in particular for the assessment of vitamin K1 and short-chain vitamin K2 was low.
In combination with the relatively small sample size, this may have yielded the study insufficiently sensitive to detect associations with vitamin K intake. Third, the definition of vitamin K status was based on a single baseline measurement of dp-ucMGP, which may only reflect short-term vitamin K status. Therefore these associations should be interpreted with caution.
{kind=link}