Despite the advent of various imaging modalities, such as PET/CT and multiparameter MRI, have been developed to detect cancer skeletal metastasis, bone scintigraphies with 99mTc-MDP remains one of the most effective diagnostic techniques for its considerable sensitivity and cost performance (21, 22). Skeletal imaging occupies 61.3% of 2.09 million of SPECT scans annually in China, and most of them were not fused with CT by the limited device utilization (23). Thus, the diagnosis of BS planar image is still a challenge for the nuclear medicine physicians in China. Fortunately, automated system might be an effective tool to overcome this dilemma. In this study, we constructed an AI model with deep neural network based on 12222 cases to extract image features, and evaluated its efficiency for diagnosing cancer bone metastasis with BS images. This model simultaneously improved diagnostic performance and time-cost for interpreting images, and the AI consulting system could potentially improve physicians’ diagnostic skills specially for younger physicians lacked experience. Besides, by the first time, the lung cancer was separated as an individual subgroup for AI analysis and indicated diagnostic accuracy of 93.36%, which seems promising for clinical use in future study.
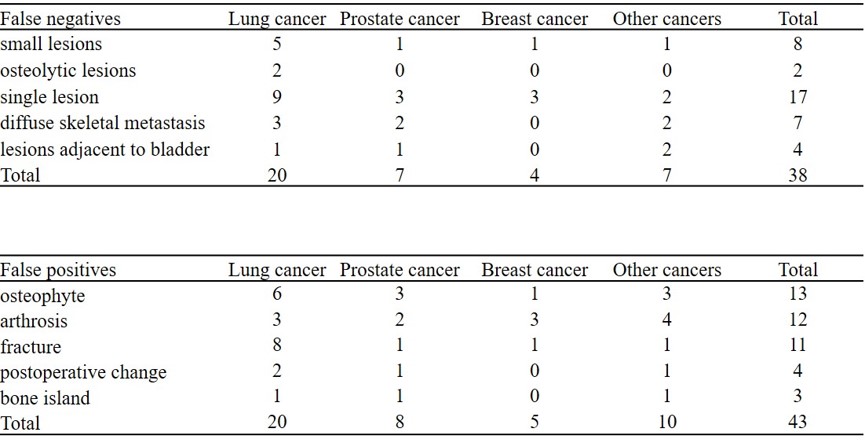
Generally, deep neural networks with sufficient valid dataset is usually conducive for improving the final outcomes for AI analysis (24). In this study, a dataset contained 12222 BS examinations from 40 cancer types, which is the largest dataset for single-center BS image interpreting by now, was used to construct the DNN for AI modeling. Compared with traditional methods using hand-crafted features, the usage of multi-input deep convolutional neural network allows AI model to follow the natural distribution, reduced subjective judgment of physicians, having better generalization performance and closer to the usual clinical environment. For example, previous studies (15, 25) usually excluded cases that could be misleading during the training process, such as patients with large bladder, sternotomy, or fracture. However, there was not any atypical cases were excluded in our dataset to help the AI model come closest to a real index. Thus, as expected, our AI model represented improved diagnostic accuracy of AUC values (0.964) compared with other BS diagnostic AI models in previous reports (0.858, 0.91, and 0.932)(18–20). Notably, although the AI model have made false-negative of 8 cases in navigating small lesions in testing cohort, it displayed better capability in small lesion recognition than human in following competition.
Although the AI model was able to efficiently improve the detection of missed small metastatic lesions by human and beneficial to reduce the readers’ error rates of BS interpretation, there are several limitations should be noted. First, the estimations by our datasets were based on BS images only, however, in “real” clinical works, the patients’ medical records, such as injury history, surgical record, characteristics of other imaging modalities and the results of laboratory tests, must be considered to obtain accurate BS interpretation. According to this, construction of a new AI model based on the fused SPECT/CT bone images is currently undergoing by our team, and we hope the addition of fused reference CT and medical records would effectively reduce the diagnostic errors, such as the false case in Fig. 7. Secondly, the unsatisfied capability in recognizing the diffuse skeletal metastasis and add-ons on patients, such as catheter, is still a noticeable disadvantage of this AI model. Last but not least, the retrospectively acquired database was collected from only one hospital for the present work. The patients at our hospital might not be considered typical of other centers, and the findings might be considered to be relatively institution-specific. A prospective multi-center study will also be needed to evaluate whether the AI model would be able to show satisfactory performance on BS images acquired with different gamma cameras, protocols, interpretive styles and incidence of metastatic disease. These processes require considerable time for collecting more clinical data and will be studied in future works.


{kind=link}