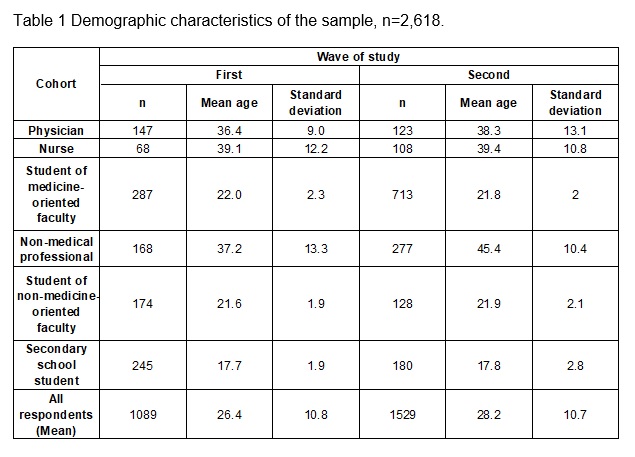
The COVID-19 pandemic is a rapidly spreading global threat that in one way or another affects everyone, regardless of their profession and age. The study reported in this paper was a spontaneous and quick response to a unique and new social situation, designed to gain a measure of understanding of Poland's population knowledge of and reactions at two very different phases of the epidemic's development in Poland. Due to the crucial role of medical professionals in tackling the pandemic, the sample was divided into the two main cohorts, medical and non-medical.
Communities’ knowledge about COVID-19
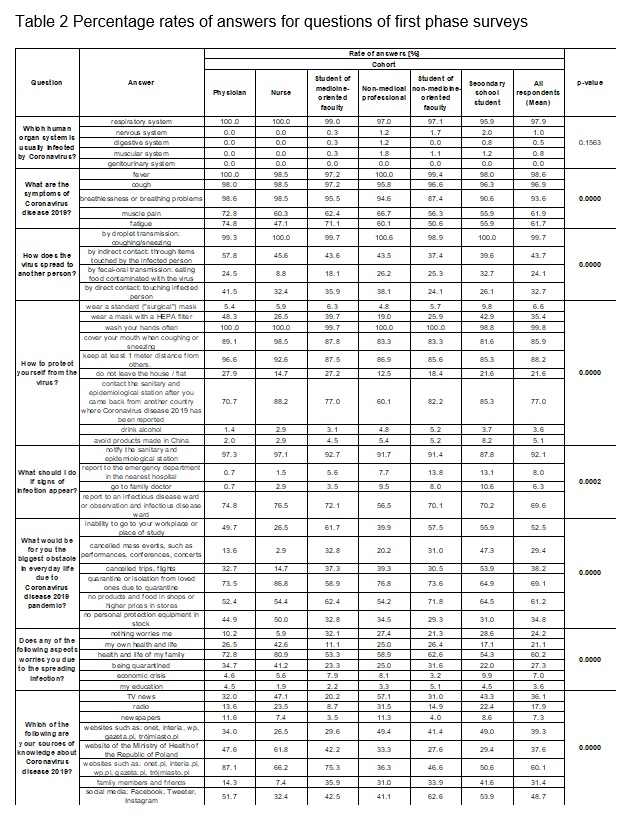
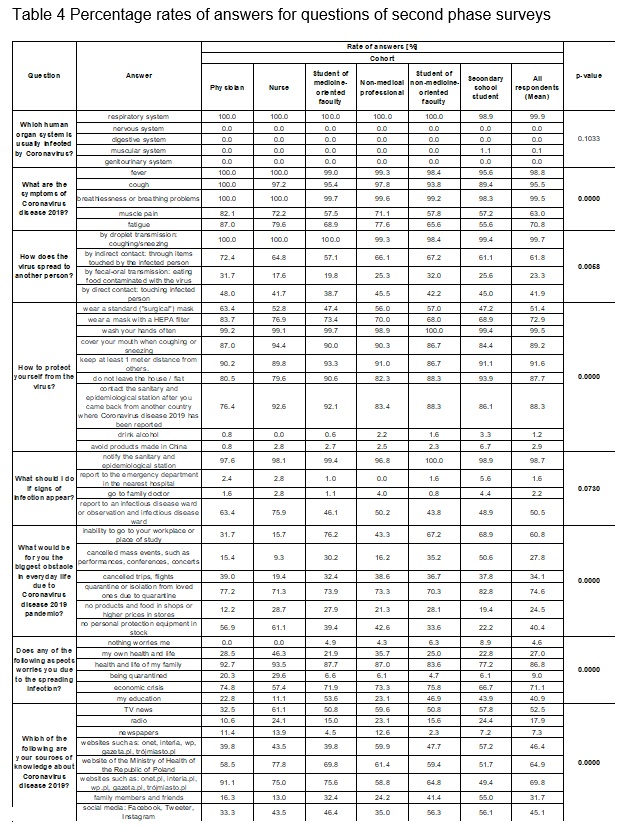
Even at the beginning of pandemic in Poland, nearly all of the respondents knew that the SARS-CoV-2 attacked the pulmonary system. Moreover, this level of knowledge was maintained a month later.
The three main symptoms of the infection (cough, fever, shortness of breath) were well known. This is similar to some studies [16–18], but different to other studies [19, 20]. Only the three main symptoms of the infection were shown on the governmental posters [21] and that is probably the reason why the non-medical respondents were mostly aware just of those. At the beginning of the epidemic, muscle pain and tiredness were mentioned only by specialised sources of scientific knowledge [1, 22] and that is probably the reason why only physicians knew about them. After a month, an overall increase in the awareness of other symptoms was observed.
In March 2020, Poles knew the COVID-19 was an airborne disease, similar to the UK and US populations [16]. After a month, they also knew that the virus could spread via direct and indirect contact. Researches marked answers pointing to these three ways of transmission as correct, as the preventive measures promoted by the government [21] to limit the spread of COVID-19 were: hand washing that limits indirect contact, covering mouth to reduce airborne transmission and social distancing, which reduces direct contact. People were highly aware of these prevention steps.
At the beginning of the epidemic, Poles knew they should call sanitary-epidemiological services or visit an infectious diseases ward if experiencing COVID-19 symptoms. Unfortunately, some people would also visit a general practitioner clinic or an emergency department. This would be a fundamental mistake as these places were not taking sufficient anti-COVID-19 preventive measures [23]. The same behaviour was noticed in South Korea during the MERS epidemics [24]. This is most likely due to the typical way the healthcare systems operate, including the Polish one. If one needs to see a physician, one goes to a general practitioner (mild cases) or an emergency department (severe cases). This changed during the pandemic as the healthcare system had to adapt to the new conditions. Fortunately, during the second assessment, a threefold and fourfold drop was observed in the percentage of respondents mentioning a general practitioner or emergency department visit with COVID-19 symptoms, respectively. This is an excellent improvement in the society's knowledge that limits the COVID-19 spread. This happened as the “do not’s” were added on posters, too [25].
Why did the Poles have such high levels of knowledge about COVID-19 that further increased later on? At the beginning, the most crucial information (transmission routes, prevention, what to do if one has symptoms) was broadly disseminated via leaflets, posters [21, 25], and mass media news reports, and repeated multiple times so people had a chance to encounter and learn it. A similar pattern was observed in other countries affected by the pandemic [26]. What is more, before the virus arrived in Poland in March, the pandemic had already been ongoing for several weeks (months, if counting from the first Wuhan infections) and had already affected many other countries worldwide (China, South Korea) and in Europe (Italy) [3]. Thus, people in Poland had more time to prepare for the new threat. Searching for information using various media could be used to reduce anxiety levels by helping people to understand the upcoming, unprecedented situation [12, 26, 27]. On the practical level, increasing one's knowledge helps to avoid infection [16].
The differences between medical and non-medical populations are understandable in the light of the requirement for continuous professional education among medical professionals. Furthermore, medical professionals form the first line of defence against COVID-19. Thus, this group had naturally more interest and a larger need to prepare early and more effectively to protect themselves.
COVID-19 information sources and their evaluation
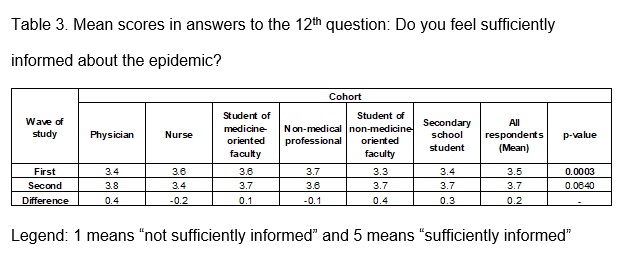
In general, people felt quite well informed to start with, and after a month the information confidence had slightly increased further. This is a result similar to other studies [18, 19, 28]. General news websites and social media were the main sources of knowledge for non-medicine-oriented respondents, which explains why at the beginning of the pandemic many people were not familiar with the up to date events and findings presented in scientific knowledge sources. Conversely, medicine-oriented community preferred science-oriented or governmental websites. Again, this group choose these sources to educate themselves as they were the first line of defence against COVID-19.
In the second wave of the study the respondents indicated using other sources of knowledge than they had used a month earlier. More respondents visited governmental and science-oriented websites. This difference was particularly noticeable among the non-medical cohort. Additionally, due to the lockdown restrictions and isolation [29], people were spending much more time at home. Thus, more people had time to watch television and learn about COVID-19 from TV broadcasts, which explains the greater popularity of this information source in the second round of the study.
Pandemic-induced fears and their changes
At the beginning of the pandemic in Poland the virus had already spread to all inhabited continents and clearly affected societies worldwide. In general, insecurity was the most alarming factor for the Poles, who sometimes felt more threatened with COVID-19 compared to, for example, people in China [26]. The probable reason was that at the beginning of the epidemic in China, the residents were not aware of the gravity of the situation and the consequences that the pandemic would bring. Moreover, media were devoting a lot of coverage to the epidemic in China [30]. All these induced additional fears and psychological impact on the Poles and other nations [31].
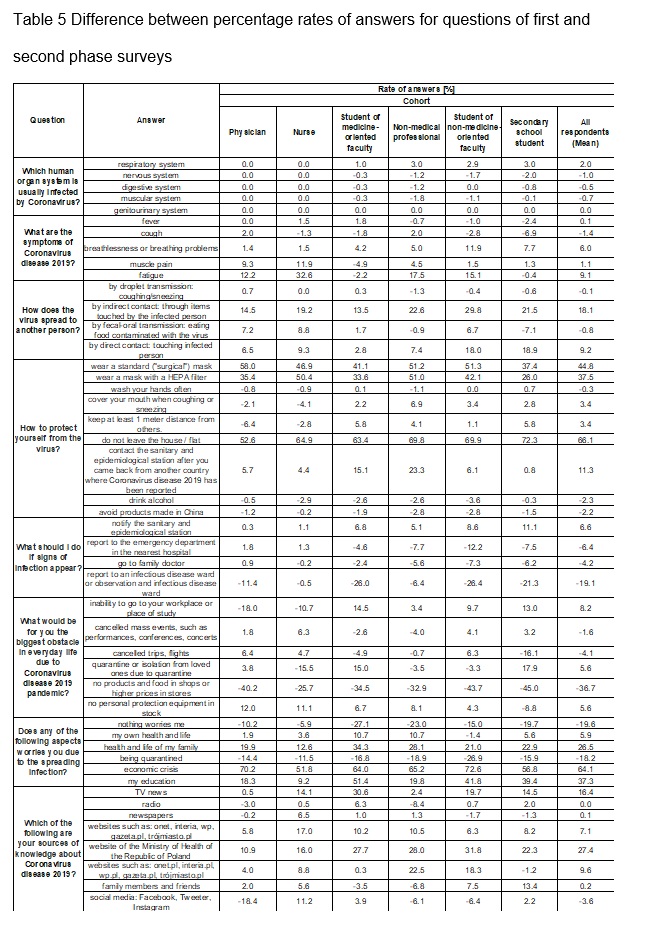
A month after the first survey was conducted, the situation in Poland had changed dramatically. Numerous governmental restrictions were imposed on the citizens in order to stop COVID-19 from spreading [4–6]. As a result, more than 95% of the respondents surveyed in the second wave of the study were scared of something (picked at least one item in the 10th question) and a 20% increase in this measure was observed between the first and the second wave of the study (Table 4, Table 5).
More specifically, however, at the beginning people were worried about the quarantine (69.1%), rising grocery prices (61.2%), and their families (60.2%) (Table 2). Later on, the main fears included economic crisis (+64.1%), education system crisis (+37.3%), and families’ health (+26.5%). On the other hand, the respondents were less often afraid of quarantine (-18.2%) or price increases (-36.7%) (Table 5).
The quarantine and isolation
As quarantine and isolation cause a separation from the family, loss of freedom, and boredom, it is understandable [27] that people would like to avoid it and that at the beginning of the epidemic they were scared of it. However, the quarantine and isolation is crucial in preventing the pandemic from spreading [1]. Due to their concerns quarantine and isolation some people might not comply with the lockdown rules, which could result in higher incidence rate in the population. After a month, the quarantine became widespread and many people themselves or their family members had to undergo quarantine. This familiarity may be the reason why, after a month of the lockdown, the respondents were less afraid of being quarantined.
Worry about family members
At the beginning many people were worried about the health of their family, similarly to the results noted in other studies [28, 32, 33]. Such concerns increased as the government imposed physical distancing, quarantine and isolation, especially for the elderly who have the greatest mortality risk [29]. Over time, the number of cases of COVID-19 in Poland increased [8]. Additionally, many healthcare systems could not manage COVID-19 without being overwhelmed (lack of hospital beds and medical personnel) which resulted in a high death toll, for example in Italy [9]. These may be among possible reasons why concerns about the health of respondents' families considerably increased and were the most frequently selected reason for worry in the second wave of the survey.
Financial crisis
It was expected that the prices for products in shops would rise or be instable, as an effect of decreased and prolonged delivery services, access, utilization and stability [34, 35]. Such thinking caused many people to stockpile for the upcoming pandemic [36]. Moreover, a global economic recession is projected [37]. The fear of job loss is experienced by 26% of the Poles [38]. As a result, the threat of an economic crisis registered the greatest increase among all reasons for worry listed in the survey.
Education crisis
Relatively low fear rate at the beginning of pandemic in three surveyed "student" cohorts was observed. With introduction of the lockdown restrictions, students could no longer attend their educational facilities. With time, students started to worry about their future and their fear rates increased in the wave two of the study. Similar trends are observed globally [14, 39, 40]. Students of medicine-oriented faculties reported this worry most frequently, likely because their courses included practical classes like laboratory classes or clinical workshops that cannot be taught online.
Fears among medical professionals
Being the first line of defence against COVID-19 for over a month, there was no respondent among nurses and physicians who did not pick at least one reason for worry. This shows that as the pandemic spread, medical professionals felt more and more endangered, possibly due to rising stress levels and tiredness. Moreover, in the second wave of the study medical professionals were the only group who did not indicate their absence at work as a worrisome problem. There is a likelihood that they would rather not go to work if they had any choice. This interpretation is consistent with the results from other studies, where physicians reported reluctance to work and even considered resignation [41] or showed poorer mental health than the population’s average [18]. Moreover, doctors experience high levels of posttraumatic stress [42], which suggests a need to pay more attention to psychological problems of the medical professionals, especially as members of this population suffer from vicarious traumatization [12] and seek increased social support during the pandemic [43].
The significant advantage of this survey is the fact that the first phase of the survey was conducted at the onset of the pandemic in Poland [3]. This allowed for monitoring of the change in level of knowledge and attitudes to COVID-19 among the Poles by repeating the same survey after a month. Furthermore, an online survey is an optimal method for collecting data during this dynamically changing situation, since it is faster and requires no contact between people, thus being more convenient than traditional methods.
Due to the shortness of time available for creating an ad hoc spontaneous survey, the interpretation of the findings from the study was subject to methodological limitations. It should be mentioned that some facts about the virus have not yet been scientifically proven and they change over time. Moreover, the samples in wave one and wave two of the study were not matched, and their demographic and professional composition differed to some extent, as the researchers did not conduct a follow-up survey and, as a result, anyone could fill in the survey in either or both waves – thus it is possible that some of the responses in wave two were from respondents who completed wave one, and some responses were from new respondents. Regardless of this methodology limitation, the samples were treated as independent samples coming from the same population. To increase the likelihood of obtaining a comparable sample, the survey was distributed by the same information channels in both waves. It is also problematic to assess whether respondents looked up answers to any of the knowledge questions while completing an online questionnaire. In addition to that, the mean age of the sample was young, so in order to get wider and stronger results the survey should have included the whole adult population.