The advent of BTKi has profoundly changed the treatment strategies in CLL and showed overall superiority to CIT in the frontline treatment of CLL17. However, such continuous treatment has led to new concerns about long-term toxicity, drug resistance, compliance of patients, and economic burden3, 18–20. Here, we prospectively analyzed iFCR as initial treatment in CLL/SLL, with or without IGHV mutation and TP53 aberrations. Among the 34 patients, including 61.8% with IGHV unmutated status and 17.6% with TP53 mutation or del(17p), iFCR induced deep and durable responses with a best response of CR/CRi and BM uMRD rates of 73.5%. The 3-year PFS and OS rates were 80.0% and 95.5%, respectively. TP53 aberrations were adversely associated with sustainable CR/CRi with BM uMRD during long-term follow-up.
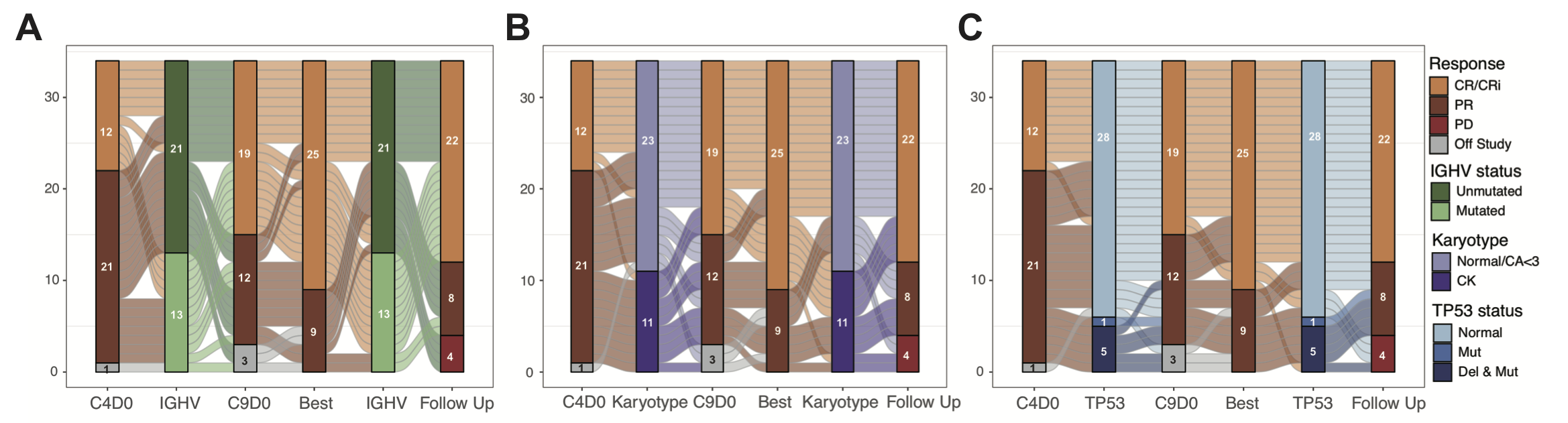
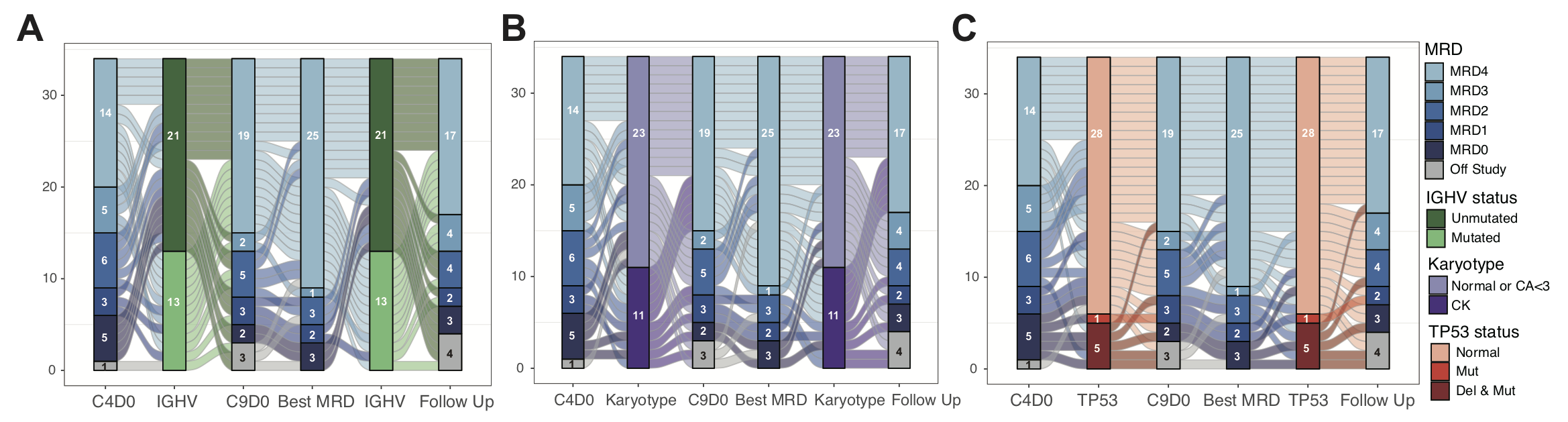
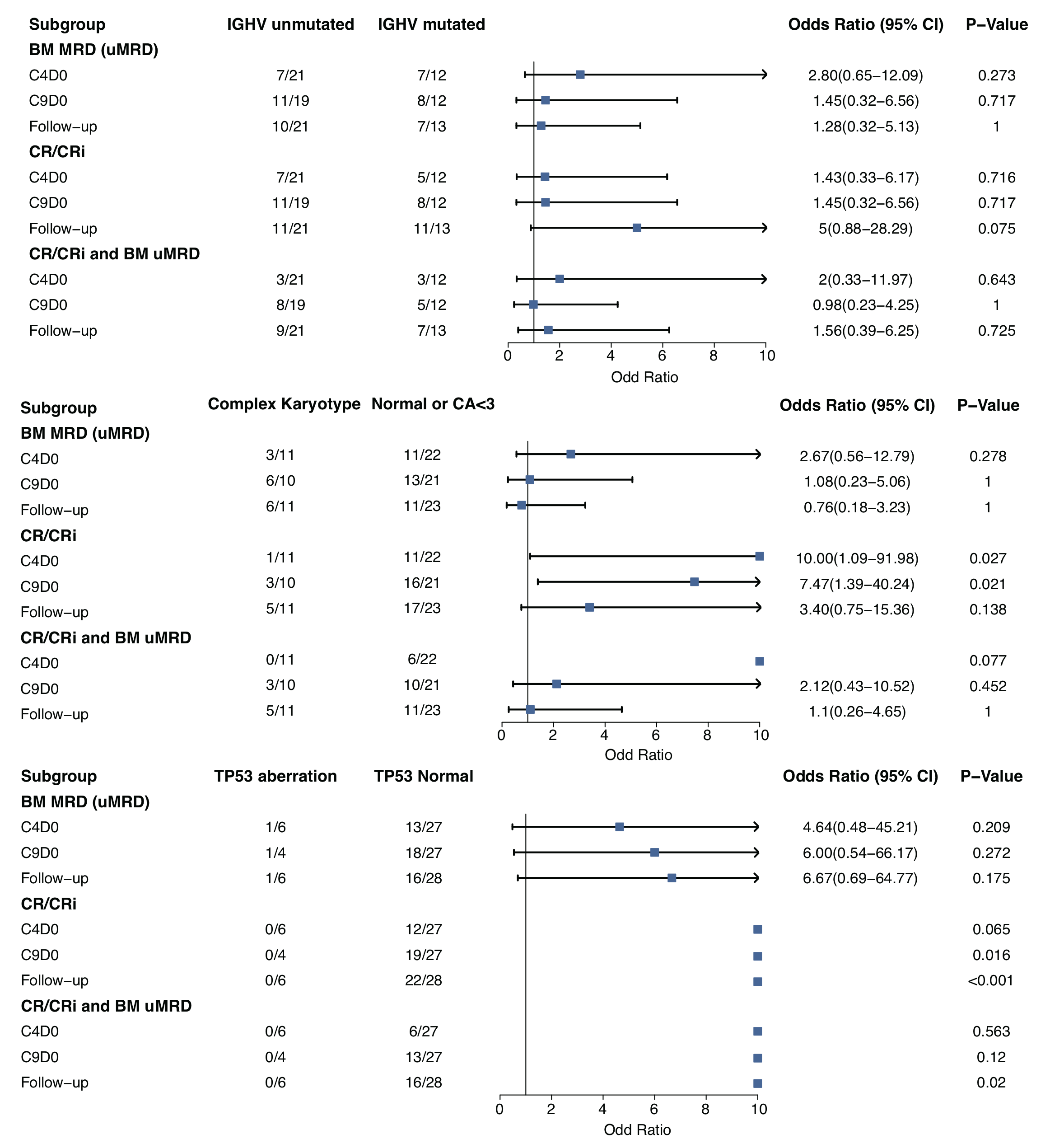
Three recent clinical trials assessed ibrutinib in combination with CIT in untreated CLL patients and achieved desirable CR and uMRD rate6, 21–23, indicating its prospect in those young patients who have demand for time-limited treatment. Davids et al. first explored six cycles of iFCR and two-year ibrutinib maintenance in previously untreated patients with CLL aged 65 years or younger6, 7. The best BM uMRD rate and CR/CRi with BM uMRD rate were 84% and 55%, respectively. No differences were founded between patients with mutated and unmutated IGHV. In our cohort, the CR/CRi rate was 38.5% and BM uMRD rate was 53.8% after three cycles and were both 84.6% at best in 13 patients with mutated IGHV. The CR/CRi rate was 46.7% and BM uMRD rate was 40.0% after three cycles and were both 86.7% at best among 15 patients with unmutated IGHV and without TP53 aberrations, showing similar efficacy with mutated IGHV subgroup. In the present study, the efficacy was comparable to Davids et al., who studied patients without TP53 mutation and left a gap regarding the efficacy of iFCR in patients with TP53 aberrations. iFCG trial demonstrated a CR/CRi rate of 38% and a BM uMRD rate of 87% after three cycles in CLL with mutated IGHV and without TP53 aberrations, with the best CR/CRi rate and BM uMRD rate of 69% and 98%, respectively21. Relatively higher BM uMRD rate in iFCG cohort as compared to our cohort could partly be attributed to the additional benefit of obinutuzumab in eradicating MRD in BM24, 25.
The combination of BTK inhibitors and BCL-2 inhibitors with or without CD20 antibodies was another time-limited strategy as first-line treatment for CLL patients26. As recently reported in the ibrutinib plus venetoclax arm of GLOW trial, PB uMRD rates were higher and achieved earlier in patients with unmutated IGHV versus patients with mutated IGHV9.In the fix-duration cohort in CAPTIVATE trial, with 12 cycles of combined ibrutinib plus venetoclax, the patients with del(17p)/mutated TP53 could attain comparable CR/CRi rate (55% vs 56%) and relatively lower BM uMRD rate (41% vs 62%) compared with patients without del(17p)/mutated TP5310, 27. Jain et al. reported the efficacy of 24 cycles of ibrutinib and venetoclax combination for 120 CLL patients with high-risk factors including del(17p) (17%) and TP53 mutation (16%)28, 29. BM uMRD improved from 52% after 12 cycles to 64% after 24 cycles, suggesting deepening remission could be attained with a prolonged combination. The present cohort was as far the first CIT-based fixed-duration study that included a high proportion of patients with TP53 aberrations; subgroup efficacy analysis showed that TP53 aberrations had a tendency to be adversely associated with achieving CR/CRi in early phase and was further found to be adversely associated with both CR/CRi and CR/CRi with BM uMRD during long-term follow up. On the other hand, among 28 patients without TP53 aberration in our cohort, long-term follow-up CR/CRi rate, BM uMRD rate and CR/CRi with BM uMRD rate was 78.6% (22/28), 57.1% (16/28) and 57.1% (16/28) respectively, comparable to patients with combination of ibrutinib and venetoclax. These results suggested a recommended selection of chemo-free fixed-duration treatment in CLL/SLL with TP53 aberrations while BTKi plus CIT could be a feasible fixed-duration treatment in CLL/SLL without TP53 aberrations irrespective of IGHV mutational status. In addition, patients with CK also showed a lower rate of CR/CRi both after three and eight cycles, but there were no differences in CR/CRi rate during follow-up due to deepened remissions achieved during ibrutinib maintenance. A pooled analysis also showed that IGHV and NOTCH1 mutation retained their prognostic role with both CIT or venetoclax-based therapy30. Although neither IGHV status nor NOTCH1 mutation was found to be adversely associated with sustainable CR/CRi and BM uMRD in our cohort, considering that all four patients with progression shared unmutated IGHV and two shared NOTCH1 mutation, the prognostic significance of IGHV status and NOTCH1 mutation need longer follow-up and larger cohort.
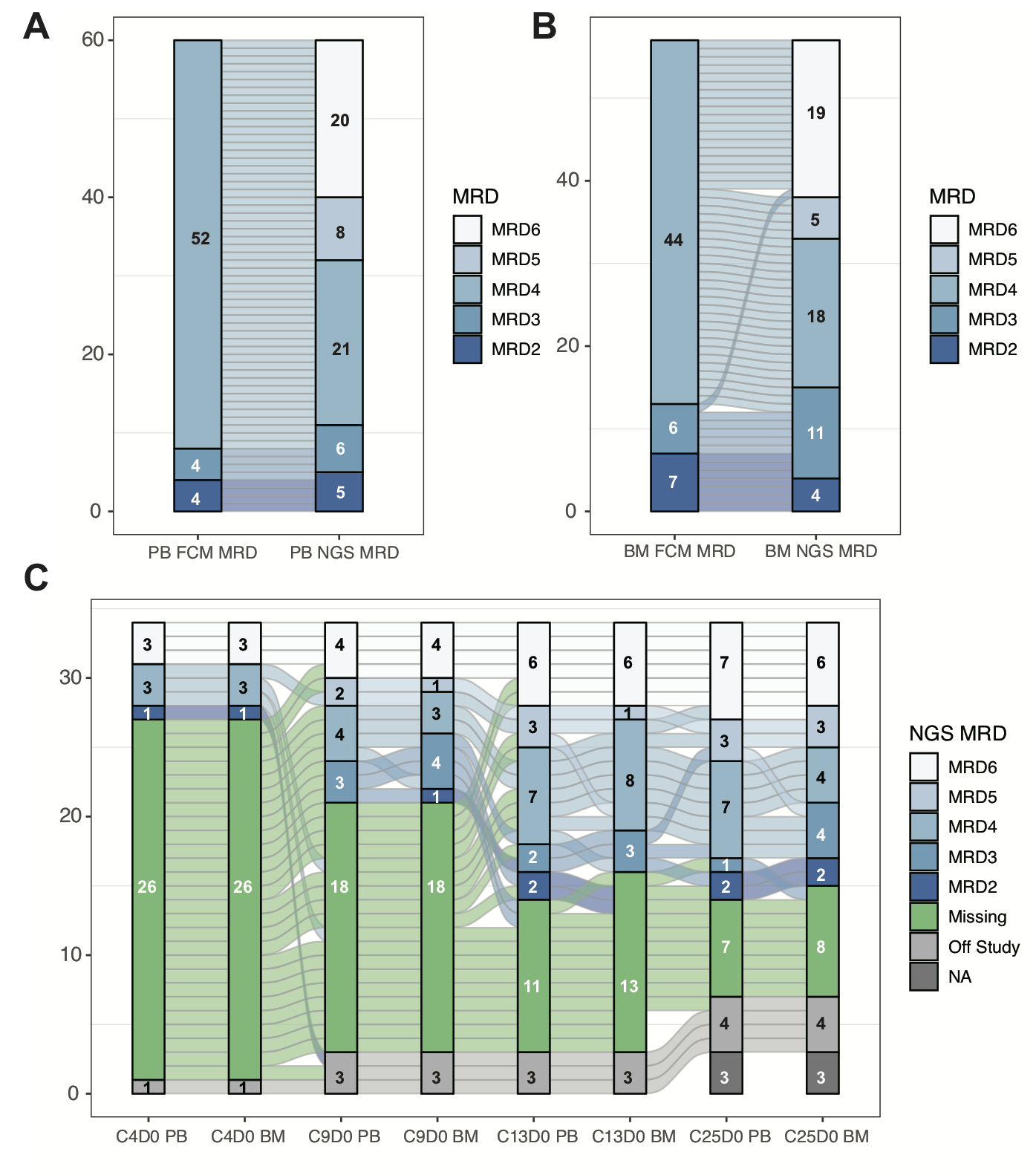
MRD was a sensitive reflection of disease burden and was proved to be correlated with PFS and OS, not only in trials of CIT such as FCR but also in trials of time-limited novel drug combinations like venetoclax plus CD20 antibody or BTK inhibitors plus venetoclax. MRD is an important surrogate endpoint in clinical trials aimed at maximizing the depth of remission and may inform treatment decision and drug discontinuation31–33. Strati et al. found that patients who achieved uMRD after three cycles of FCR failed to benefit from additional three cycles in terms of PFS34. The subgroup analysis in the present study also revealed that for most patients who achieved BM uMRD after three cycles of iFCR, ceasing further FC regimen led to a sustained or further remission, while additional three cycles of FC regimen failed to benefit either patients who achieved PR or BM MRD ≥ 1% after three cycles of iFCR. Moreover, patients who achieved BM 10− 6 by NGS with FCR treatment showed a superior PFS to those who achieved BM 10− 4 by FCM while remaining MRD positive at the 10− 6 level35. In the iFCG trial, with a median follow-up of 44.2 months after ibrutinib discontinuation, only six of 41 patients had MRD occurrence of PB and none of them showed clinical progression8. Notably, all six patients were among the 16 patients who were BM MRD positive at 10− 6 by NGS after three cycles of iFCG, while no patients displayed MRD occurrence of PB among 20 patients who were BM MRD negative/indeterminate at 10− 6, suggesting the clinical significance of achieving deep MRD remission in early phase. Clonal evolution models were also explored by longitudinal targeted-gene NGS of MRD samples from patients with progression. TP53, NOTCH1 and EGR2 mutation clones underwent linear evolution while ibrutinib-resistant subclones such as BTK C481S and PLCG2 mutation gradually expanded under ibrutinib treatment pressure, leading to drug resistance.
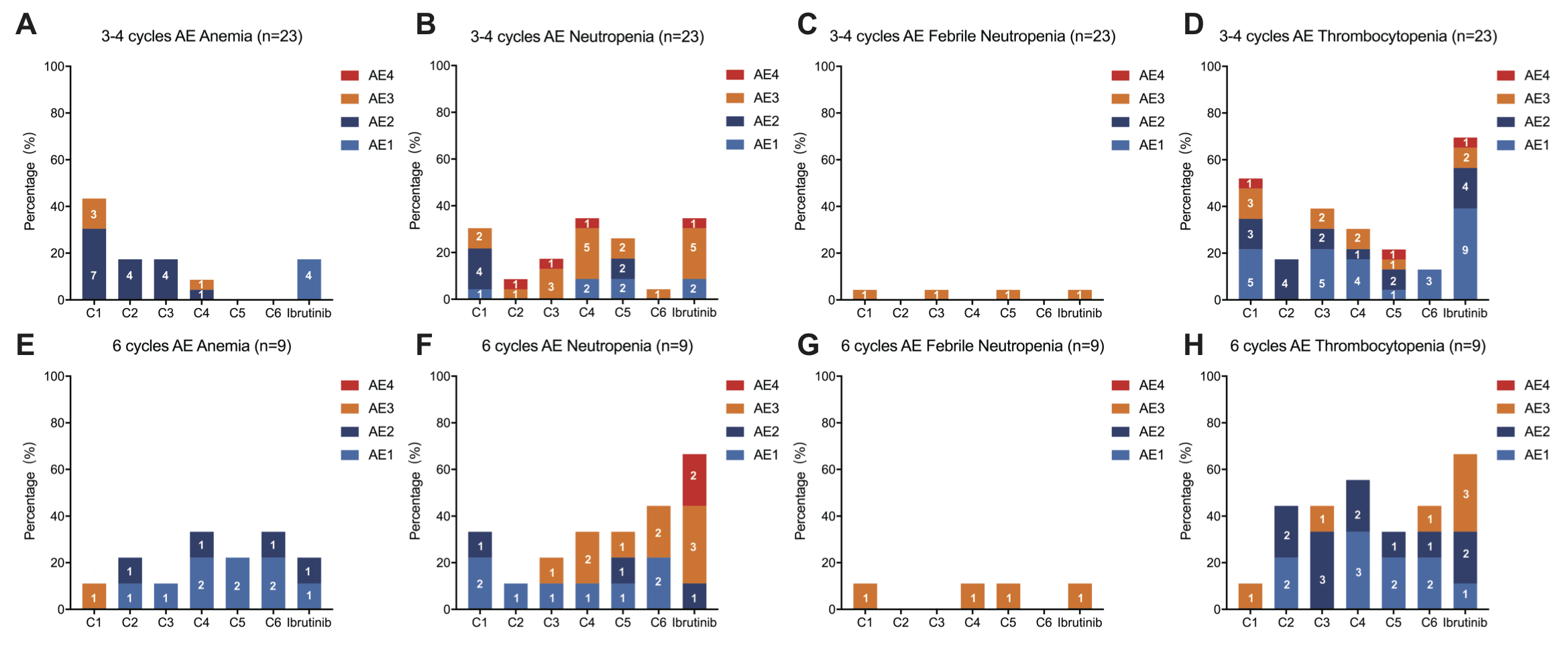
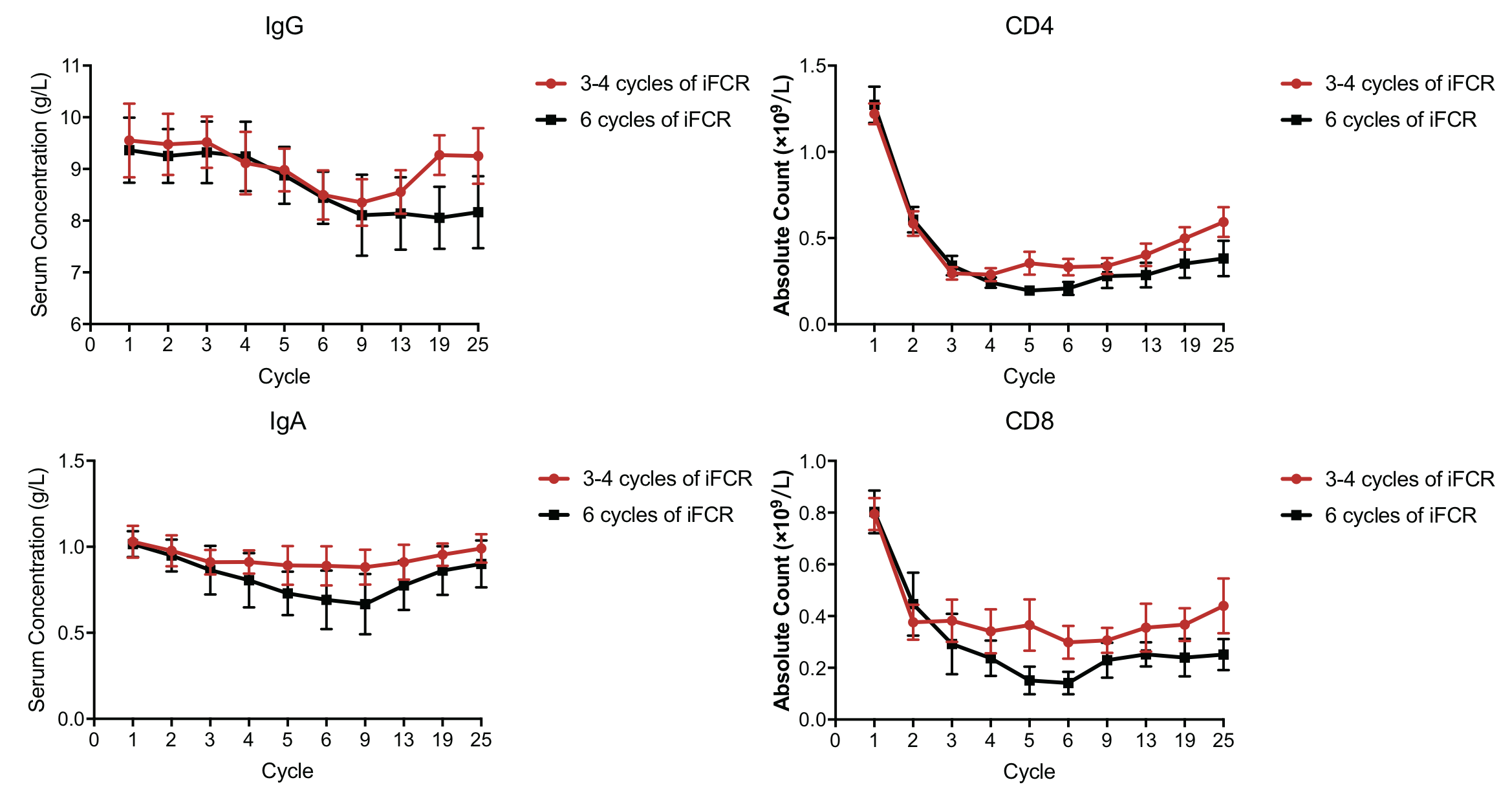
In the present study, iFCR did not display new safety signals, and the occurrence of AEs was comparable to previous studies 6, 21. During ibrutinib maintenance phase the occurrences of dose-hold ≥ 7 days and dose reductions and were lower than those reported in RESONATE-2 trial (median age 73, range from 65–89)1, 36, 37, partly due to the relative young age, and also for tailored chemotherapy after 3 cycles of combination in over half of patients. In our cohort, one patient who experienced FC dose-reduction twice achieved CRi and BM uMRD at C4D0 and progressed at C31D0. Furthermore, among 4 patients in our cohort who showed MRD recurrence without clinical progression, three experienced at least once of ibrutinib discontinuation or dose-reduction due to AEs or lung cancer surgery. Based on these, long-term ibrutinib discontinuation or dose reductions might adversely impact the maintenance of uMRD during 2-year treatment. For patients who achieved early CR/CRi and BM uMRD remission, 3 cycles of combination and further tailored chemotherapy might benefit the early immune restoration, and grade 3–4 AEs reduction during ibrutinib maintenance, which might contribute to response improvement and sustainable MRD level maintenance38. Studies reported that FCR regimen could lead to t-MDS/AML in 2%-7% of the patients, but with a median follow-up of 33 months, no t-MDS/AML was found in the present study39, 40.
The present study had limitations. It was a single-center real-world study with a limited number of patients. Lack of randomization to patients who received 3–4 to 6 cycles of iFCR and a relatively short follow-up of 33 months. Although the level of evidence of real-world studies is lower than for clinical trials, real-world studies provide complementary data to clinical trials because they include patients with TP53 mutations.
In summary, the present study demonstrated the durable effectiveness and favorable safety profile of the iFCR combination regimen in a real-world young fit Asian population of patients with CLL/SLL. Fit young patients without TP53 aberrations could benefit from iFCR to achieve early remission and durable drug holiday, irrespective of the IGHV mutational status, and most patients were well during the 2-year treatment. The clone evolution analysis might provide clues for the further study on the mechanism of treatment resistance. Future studies should explore the subgroups that might benefit the most from the treatment and compare the efficacy and tolerability with other time limited chemo-free strategies, such as a combination of BTK inhibitors and BCL-2 inhibitors.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}