A total of 30 interviews were conducted. We interviewed participants from a total of eight out of ten PCNs, and all participants recruited at that point of time were involved in the delivery of chronic care at the primary care setting.
Participant characteristics
During the recruitment process, 28 participants were recruited by purposive sampling while two were recruited by snowball sampling. Out of 30 participants recruited for our study, nine where PCN leaders. The average age of our participants was 49 years of age (range 31-68 years old), and their average duration spent in primary care was 18 years (range 3-35 years). In fact, most participants had been in their own practice for a relatively long duration averaging 14 years (range 1-35 years). Our sample comprised of 27 male and three female private GPs.
Main findings
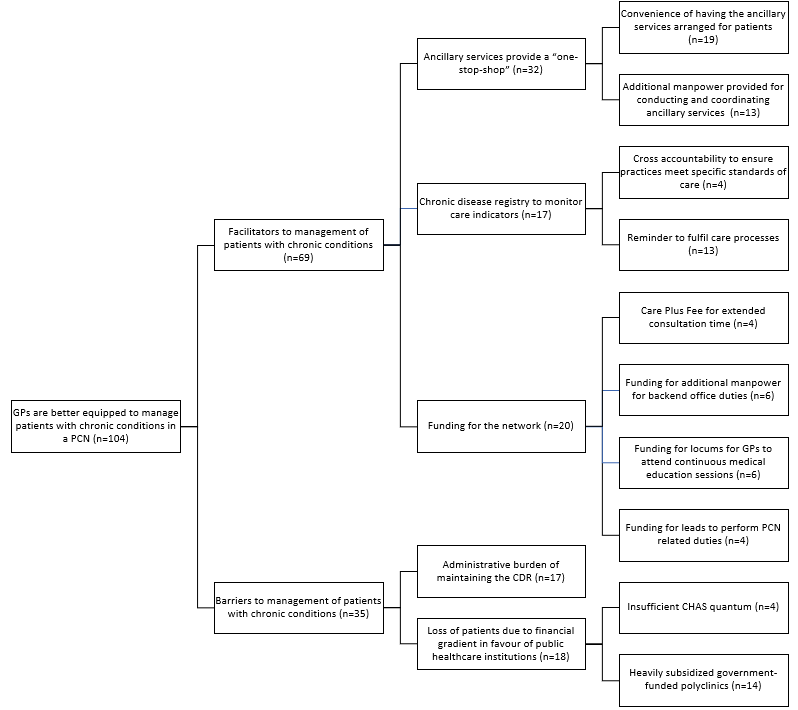
Fig. 1 Diagram of facilitators (+) and barriers (-) developed based on results
Three themes were identified as facilitators and two themes that were identified as barriers to the management of chronic conditions. The facilitators are 1) ancillary services to provide a “one-stop-shop”, 2) chronic disease registry (CDR) to monitor care indicators and 3) funding for network. The barriers are 1) administrative burden of maintaining CDR and 2) loss of patients due to financial gradient in favour of public healthcare institutions. All themes and subthemes, along with the number of data units, are reported in our coding tree (Additional file 3).
(+) Theme 1: Ancillary services to provide a “one-stop-shop”
Every PCN is outfitted with wrap-around ancillary services which included diabetic retinal photography (DRP), diabetic foot screening (DFS) and nurse counselling (NC). These ancillary services enabled private practices which were traditionally too small to sustain or arrange for such services an opportunity to provide more holistic and preventive care for their patients. The individual practices are also supported by a team of nurses and care coordinators, expanding the time for patient care by the entire primary care team.
Subtheme 1.1. Convenience of having the ancillary services arranged for patients
Traditionally, private GPs would have to refer their patients to the polyclinics or government hospitals for ancillary services. However, the PCN enables each clinic to provide ancillary services to their patients when the services of a roving team are employed. Therefore, patients will not only be able to see the same doctor but also have the ancillary services conducted at the same location. As most patients reside near the clinic, this “one-stop-shop” enables a higher level of convenience and lowers the perceived barriers to attend ancillary services.
“[…] eye screening and nurse education [services available at polyclinics], but whereas in primary GP clinics, we are unable to offer that, right? So the current workflow is we need to refer patients back to even polyclinic or back to other service centres for eye screenings right? So these extra referrals or extra effort for the patient is not an optimal workflow for the patient and that will reduce the uptake on a lot of services. So PCN with our own ancillary and even mobile services, hopefully, it will provide a bit more convenience to the patient.” (R26)
Subtheme 1.2. Additional manpower provided for conducting and coordinating ancillary services
The lack of ancillary service support and busy clinic hours raise the challenge of counselling patients on disease-modifying behaviours, diabetic eye and foot examinations for independent GPs. Having additional manpower in the form of nurses hired by the PCN contributes towards the practices in carrying out these essential ancillary services to prevent avoidable amputations or blindness in patients. PCNs have the liberty to either employ and train their own nurses or outsource the services to external vendors that provide a roving team of nurses to conduct ancillary services at their clinics.
Furthermore, PCNs are provided with additional manpower to arrange for ancillary services and remind patients to attend the arranged services which alleviate the workload for clinic assistants and reduce patients’ default numbers. This task is fulfilled by primary care coordinators (PCCs), but it should be noted that PCCs can also be assigned other PCN related tasks such as the consolidation of patient data for maintenance of the CDR (elaborated in subtheme 3.2).
"[…] CAs [clinic assistants] or my doctors will just have to register the patient, and then the PCCs will then follow up with patients on their appointments, and then they will book, and then they will then get their appointments, work with the patients to get their appointments and then bring the provider [roving ancillary services team] to provide their service in our clinic." (R46)
"The DRP, DFS I believe is done by Diabetic Society [external vendor]. Their nurses will be running inside the van. [Name of PCN] has their own roving nurse, so I understand that they will be providing the nurse counselling and also maybe helping with some of the DRP, DFS." (R21)
(+) Theme 2: Chronic disease registry to monitor care indicators
The CDR is a platform that enables the systematic tracking of care components for patients. Data is tabulated into an excel spreadsheet which comprises over 200 fields, from basic sociodemographic data, date of clinical diagnosis and screening attendances to clinical parameters for chronic conditions in accordance with local clinical practice guidelines. CDR data is submitted to AIC to ensure required care components are fulfilled before care plus fee (elaborated in subtheme 3.1) is dispersed by AIC to the PCN. Thus, the CDR gives GPs and AIC a dashboard view of the quality of care provided, allowing for the identification of opportunities to refine existing management practices using quantitative parameters by improving processes and outcomes.
Subtheme 2.1. Cross accountability to ensure practices meet specific standards of care
Most solo GP practices work in silos, and a certain level of accountability is needed to ensure that practices not only follow guidelines but provide the best care for their patients. Therefore, anonymized results of performance indicators of all practices are made available during implementation and review sessions every quarter to perform benchmarking. This can potentially reduce the variation in performance and improve quality of care for patients.
"[…] my understanding of the CDR, is that they want to benchmark, they want to benchmark the care of the patient, that means ah, for example, the PCN, within the PCN, let's say, everybody, the average PCN for example, the HbA1c for diabetic, you know is let's say 8, and my clinic, all my patient are 9, then they say, I am below average, so there is a benchmarking […]" (R39)
Subtheme 2.2. Reminder to fulfil care processes
This platform allows practices to follow-up with patients when required and ensure judicious completion of necessary procedures in their care management plans.
"Alright, so I guess in a way it [CDR] reminds especially the private doctors, especially when your clinic so busy. A lot of times we will overlook, or we will forget certain things […] So this, in a way, is a constant reminder to making sure that this is done for the patient." (R26)
(+) Theme 3: Funding for the network
Every PCN is entitled to funding from the government. A commitment of $45 million per annum by the government [30] will equip the network with more resources to better manage chronic patients than what could be harnessed as an individual private practice. This funding is mainly dispersed on a reimbursement basis through AIC.
Subtheme 3.1. Care Plus Fee for extended consultation time
Private practices are business entities that generate revenue mainly through consultation fee and the sale of medicines. As a result, the revenue generated is volume-based, making it more profitable for GPs to see to more acute cases. However, complex chronic patients require a lengthened consultation. Hence, the care plus fee (CPF) was introduced to reimburse clinics for extended consultation time. However, process and clinical outcome indicators stipulated in the CDR must be completed before the CPF is dispersed by AIC.
"The care plus fees are incentives for all members of the PCN […] who are managing the complex chronic cases. They will receive a financial incentive per patient because it takes longer and more time resource to manage these patients. So per year, they are given a quantum of 100 dollars [per chronic patient], but of course, you must satisfy all the criteria [CDR requirements] stipulated to prove that you are managing a complex patient." (R15)
Subtheme 3.2. Funding for additional manpower for backend office duties
Funding is provided for PCNs to employ PCCs to coordinate ancillary services, track patients, remind patients to attend ancillary services and to consolidate data for the CDR as most solo practices do not have the manpower to conduct non-clinical duties. Funding for PCCs come in the form of full-time equivalents which is furnished by AIC based on the PCN’s projected chronic patient load.
"Primary care coordinators if I am not mistaken […] I think it is one is to one FTE [full-time equivalent] to 3000 patients […]" (R36)
Subtheme 3.3. Funding for locums for GPs to attend continuous medical education sessions
Funding is provided for PCNs so that GPs can hire locums when they attend continuous medical education (CME) sessions. The availability of locums motivated GPs to attend CME sessions while maintaining clinic services in the interim.
"[…] I know that specifically there is funding for them to employ locum, so if they have to employ locum to go for this (CME sessions), there is funding to pay for their locum.” (R48)
Subtheme 3.4. Funding for leads to perform PCN-related duties
Funding for PCN leads is used to backfill time lost at their practice when performing PCN-related duties. Duties include developing working relationships with leads of other PCNs, providing strategic and clinical leadership and spearheading quality improvement over member practices.
"[…] PCN leads are given 0.4 FTE [full-time equivalent] […] for a GP because it is an opportunity cost for you to be taken away from his clinic, that money goes directly into his pocket, that is to compensate him for the time lost because he could be otherwise seeing patients." (R36)
(-) Theme 4: Administrative burden of maintaining the CDR
The maintenance of the CDR requires consolidation of data regarding the process and clinical indicators by both GPs and clinic assistants. Despite having additional administrative support from PCCs to consolidate registry data, routine documentation has proven highly laborious for practices overstretched by other administrative duties and lean manpower structure, leading to more man-hours or overtime duties. Clinics also face difficulty in extracting data from their clinical management system (CMS) due to the lack of a smart extraction tool that aligns with CDR requirements.
"Fortunately, our staff are understanding, but you cannot say so for the same for other solo practice, so the technical staff may not actually want to do paperwork, and if it falls on the onus of the doctors to do it, I don't think they have the time also beyond their clinical time too." (R18)
"For those clinics using Clinic Assist [CMS] with the CMS that is linked to PCN yes, that will be easier. You just need to key in your numbers and click submit [smart extraction tool function], but for a lot of other clinics not using Clinic Assist and integrated with PCN, what do we do? We need to manually write it down or manually key in individual patient clinical indicators for both MOH and PCN. So with the busy clinic, the doctor has no time to do it, the staff has no time to do it, so we need to OT [overtime] to submit all these." (R26)
(-) Theme 5: Loss of patients due to financial gradient in favour of public healthcare institutions
Perceptions of the affordability of healthcare affect the uptake of medical services. The high levels of government subsidies offered at public healthcare institutions such as the polyclinics and public specialist outpatient clinics are highly attractive to price-sensitive patients. The launch of Community Health Assist Scheme (CHAS), which extends healthcare cost subsidies to patients visiting private GPs is a finite quantum calibrated based on patients’ financial circumstances. CHAS attempts to alleviate the stress placed on the public healthcare sector resulting from the huge volume of patients drawn to their subsidized services and medicines.
Subtheme 5.1. Insufficient CHAS quantum
Complex chronic conditions require multiple visits to the clinic and long-term medication. Participants reflected that the quantum is usually sufficient for patients with simple chronic conditions but insufficient for patients with complex chronic conditions, as more medications need to be prescribed. Therein lies the possibility that care for multimorbid patients provided by their private GP might discontinue after the CHAS quantum has been exhausted.
"The CHAS subsidies help, but it is for simple chronic illness, for simple cases […] But when it comes to more medication […] it makes it very difficult, even with the CHAS subsidy." (R48)
Subtheme 5.2. Heavily subsidized government-funded polyclinics
The financial gradient between private primary care and government subvented primary care at polyclinics promotes specific health-seeking behaviour. As patients are price-sensitive, they turn to the largely government-funded polyclinics to obtain subsidized medications. Aside from cheaper medications, the heavily subsidized consultation fee makes polyclinics more appealing to price-conscious patients, promoting the severance in care continuity with their private GP.
"You cannot fight with the polyclinic because they are subsidized so you cannot compare. We have no subsidy for drugs. We have no subsidy for consultation." (R48)
“I would say that we have been able to keep a certain number of chronic patients within the registry. But of course, the challenge is keeping them in […] they didn’t come back after one visit, since last year. So this group of patients I would assume that they have kind of withdraw themselves from the system […] Sometimes, they are, for example, going back to the polyclinic. Most of the time is cost issues.” (R20)
{kind=link}