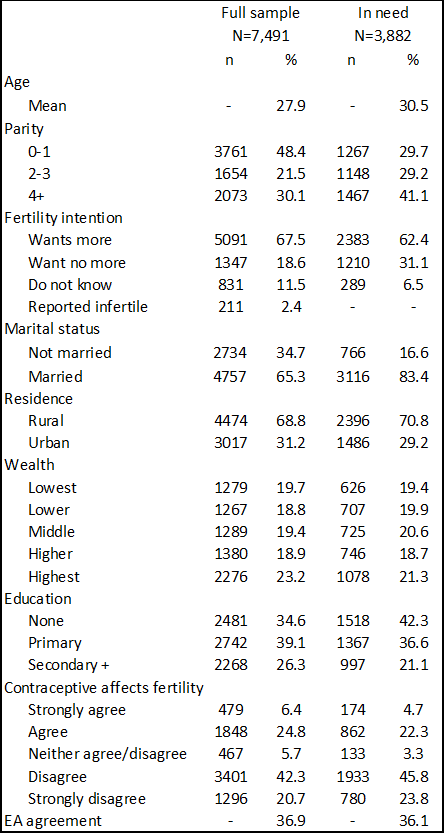
We find that concerns of contraceptive-induced fertility impairment are associated with lower hormonal contraceptive use in Ethiopia and that these concerns may be particularly influential for high parity and rural women. We also found, however, that approximately 6 in 10 women either disagreed or strongly disagreed that using contraception would make it harder to get pregnant later, indicating that while these concerns are impactful, they may not be as widespread as qualitative evidence suggests.
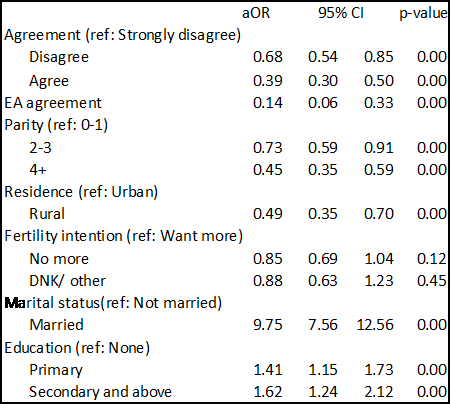
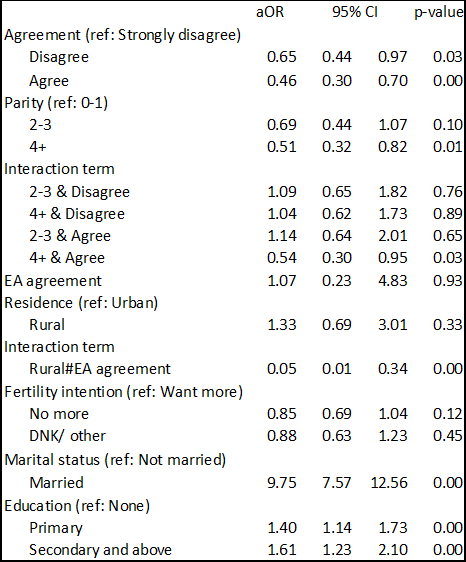
Given the range of negative mental, physical, social, and financial outcomes associated with infertility in sub-Saharan Africa (1, 3, 29), in addition to the importance placed on motherhood in high-fertility settings such as Ethiopia (22, 30), we hypothesized that the fear of contraceptive-induced infertility would be particularly impactful amongst nulliparous or primiparous women who are unlikely to have completed childbearing. We found that women who agreed that contraception could impact fertility were less likely to use contraception, but contrary to our hypothesis, this effect was particularly strong amongst the highest parity women. This is likely due in some part to reverse causality – women who are concerned about the safety of contraception are less likely to use it and thus, may be more likely to experience pregnancy. It does, however, suggest that high parity women may be a particularly important group to counsel on the safety of hormonal contraceptive methods, as they are also more likely to wish to limit childbearing than young and low-parity women (31, 32). Regardless of parity, however, it is clear that any level of agreement with this statement had a significant, negative effect on the probability of using contraception, underscoring that concerns about contraceptive-induced fertility impairment are a critical barrier to contraceptive use amongst women who wish to delay pregnancy. Addressing these concerns during contraceptive counseling is important but this will likely bear the greatest impact amongst women who are already seeking contraceptive services. Given the strong relationship we observed between endorsing beliefs about contraceptive-induced fertility impairment and contraceptive use among high parity women, incorporating counseling on the safety of contraception during the postpartum period, when women are likely to both wish to delay pregnancy and have frequent contact with the health system, may be an ideal period during which to counsel women.
After accounting for individual fears of contraceptive-induced fertility impairment, we also found a strong association between higher levels of concern in the community and reduced probability of hormonal contraceptive use at the individual level, but this effect was seen only among rural women. Though not shown in our results, there was no difference in the association between individual-level agreement and hormonal contraceptive use between urban and rural women. While the influence of individual-level concerns, thus, seems to operate largely the same between urban and rural level women, we found that community-level concerns were linked to contraceptive practices among women in rural areas only. This may be due in part to the way we operationalized community-level concerns as an average of women in the enumeration area. In rural areas, women in the same geographic area may be a more influential group on health behavior than in urban areas where immediate neighbors may not be as well-known or trusted sources of reproductive health information. While not specific to modern contraceptive use at the individual level, Metheny and Stephenson demonstrated how norms related to fertility and family planning behavior, when measured at the community level, differed in their effect on unmet need between urban and rural areas (33). The majority of other studies exploring the effect of social norms on family planning use tend to either be restricted to only urban (34, 35) or rural areas (36, 37), or include residence as a confounding factor (16, 38–40), rather than effect modifier, thus limiting our ability to compare results directly. Nonetheless, our findings indicate that addressing more widely held concerns about contraceptive-induced fertility impairment may be particularly critical in rural areas. Programs designed to engage communities and large-scale mass-media campaigns may be particularly pertinent means to address these concerns.
Our study is not without limitations, many of which are measurement related and would benefit from additional research efforts. As noted in other studies (15, 18), we do not include a specific time frame in the question which means we cannot differentiate between concerns about delayed return to fertility versus long-term or permanent impacts on fertility. Future research should attempt to differentiate between these concepts as they may differentially influence decision-making. Additionally, to estimate the influence of community-held concerns about contraceptive-induced fertility impairment, we relied on aggregation of individual beliefs from women of reproductive age, however there may be many individuals in the community, including older women and men, who share this concern and who are not represented. Finally, we asked about concerns related to contraceptive-induced fertility impairment arising from general contraceptive use, rather than identifying whether these concerns were associated with specific methods. Women may hold distinct beliefs about contraceptive-induced fertility impairment for specific methods versus others, however, which may shape their contraceptive behavior in different ways. In addition to the measurement challenges outlined above, we use cross-sectional data and cannot determine causality. As noted above, this allows for the potential of reverse causality in our findings. Finally, given the inclusion of the question in a survey that largely focuses on family planning, it is possible that respondents felt some degree of social desirability to respond favorably to questions related to family planning and may have overstated their disagreement with the statement.
Despite these limitations, however, our study has a number of strengths. We use data from a unique survey item, derived from qualitative data in Ethiopia and other sub-Saharan African settings, that is not regularly available in other large-scale surveys to explore concerns in data that are nationally representative data among reproductive-aged women. The large sample allowed for sufficient sample size to explore relationships across both parity and residence, adding further nuance to our understanding of how fears of contraceptive-induced fertility impairment operate.
{kind=link}
{kind=link}
{kind=link}
{kind=link}