Baseline characteristics
Forty-one patients (mean age 42.2 y ± 12.2, 75.6 % female) with previous SARS-CoV-2 infection and exhibiting PCS-typical symptoms were recruited. Patients were age- and gender-matched with 41 healthy volunteers (41.8 y ± 13.7) from a HC group (n = 204). After matching, CV risk factors were not significantly different between the two cohorts. The most frequent comorbidities and chronic medication in the PCS cohort are shown in Table 1. During acute SARS-CoV-2 infection, four (9.8%) patients were hospitalized, and one (2.4%) patient was admitted to the intensive care unit (ICU). Patients, which had been hospitalized with acute infection showed a tendency towards higher PCS severity scores (34.6 ±9.3 vs. 45.6 ±8.5, p=0.07). There was no difference between virus variants in PCS severity scores (Fig. E1: Online Supplement). The median time of PCS duration was ten months (7.0 - 18.0 months) with a mean PCS severity score of 35.7 (± 9.7). Fatigue (95.1%), exercise intolerance (90.2%), and brain fog (90.2%) were the three most abundant symptoms. Eight (19.5%) patients were laid-off, and the median cumulative time off sick leave was 122.0 days (4.0 - 291.0 days). Standard laboratory parameters showed significantly higher leukocytes in PCS patients (Table 1).
Table 1 Baseline characteristics
|
Clinical characteristics
|
SARS-CoV-2
naïve (n=41)
|
PCS
(n=41)
|
P
value
|
|
Age
|
|
years, Mean (SD)
|
41.8 (±13.7)
|
42.2 (±12.2)
|
0.89
|
|
Gender
|
|
female
|
31 (75.6%)
|
31 (75.6%)
|
1.00
|
|
BMI
|
|
kg/m2, Median (IQR)
|
23.6 (±3.5)
|
24.2 (±3.9)
|
0.55
|
|
RRsyst
|
|
|
|
|
mmHg, Median (IQR)
|
120 (116-130)
|
118(112-130.5)
|
0.53
|
|
Cardiovascular risk factors
|
|
Obesity
|
8 (25.8%)
|
15 (48.4%)
|
0.60
|
|
Nicotine abuse
|
5 (16.1%)
|
6 (19.4%)
|
1.00
|
|
Art. hypertension
|
7 (22.6%)
|
8 (25.8%)
|
1.00
|
|
DM
|
0 (0.0%)
|
0 (0.0%)
|
1.00
|
|
Hypercholesterolemia
|
-
|
19 (61.3%)
|
-
|
|
Acute SARS-CoV-2 Infection
|
|
Severity of acute infection
|
|
|
|
|
0
|
-
|
0 (0.0%)
|
-
|
|
2
|
-
|
24 (58.5%)
|
-
|
|
3
|
-
|
13 (31.7%)
|
-
|
|
4
|
-
|
2 (4.9%)
|
-
|
|
5
|
-
|
1 (2.4%)
|
-
|
|
6
|
-
|
1 (2.4%)
|
-
|
|
Variance
|
|
|
|
|
Alpha
|
-
|
3 (7.3%)
|
-
|
|
Delta
|
-
|
7 (17.1%)
|
-
|
|
Omicron
|
-
|
10 (24.4%)
|
-
|
|
Unknown
|
-
|
21 (51.2%)
|
-
|
|
Number of vaccinations
|
|
|
|
|
0
|
-
|
3 (7.3%)
|
-
|
|
2
|
-
|
15 (36.6%)
|
-
|
|
3
|
-
|
23 (56.1%)
|
-
|
|
PCS characteristics
|
|
PCS duration
|
|
|
|
|
months, Median (IQR)
|
-
|
10.0 (7.0 - 18.0)
|
-
|
|
PCS severity score
|
|
|
|
|
Mean (SD)
|
-
|
35.7 (9.73)
|
-
|
|
Fatigue
|
-
|
39 (95.1%)
|
-
|
|
Exercise intolerance
|
-
|
37 (90.2%)
|
-
|
|
Brain fog
|
-
|
37 (90.2%)
|
-
|
|
Cumulative days of sick leave
|
|
|
|
|
days, Median (IQR)
|
-
|
122.0 (4.0 - 291.0)
|
-
|
|
Work-loss due to PCS
|
-
|
8 (19.5%)
|
-
|
|
Comorbidities
|
|
Hypothyroidism
|
-
|
8 (19.5%)
|
-
|
|
Bronchial asthma
|
-
|
6 (14.6%)
|
-
|
|
Medication
|
|
ACE2-inhibitors
|
-
|
3 (7.3%)
|
-
|
|
ß-blockers
|
-
|
5 (12.2%)
|
-
|
|
Psychiatric/sleeping medication
|
-
|
8 (19.5%)
|
-
|
|
L-Thyroxin
|
-
|
8 (19.5%)
|
-
|
|
Asthma inhaler
|
-
|
6 (14.6%)
|
-
|
|
Lab parameters
|
|
Leukocytes
|
|
|
|
|
G/L, Mean (SD)
|
5.3 (4.7-6.3)
|
6.2 (5.3-7.4)
|
0.027*
|
|
Hb
|
|
|
|
|
mg/dl, Median (IQR)
|
14.9(13.7 – 15.3)
|
14.1 (13.5-14.4)
|
0.095
|
P-values are shown for statistical tests comparing PCS patients (n=41) with SARS-CoV-2 infection naive participants (n=41); t-test was used for normally distributed variables, the χ2 test for categorical variables, the Wilcoxon rank sum test for variables with a skewed distribution, and Fisher’s exact test for binary variables. BMI, body mass index; RRsyst, systolic blood pressure; Art., arterial; DM, diabetes mellitus I or II; obesity is defined as BMI > 25 kg/m2; hypercholesterolemia is defined as cholesterol > 200 mg/dl. Severity of acute infection was assessed using the WHO clinical progression scale[45]. PCS severity score was assessed using the score published by Bahmer et al. [36].
Retinal vessel reactivity to flickering light (DVA) and structural aspects of retinal microvasculature (SVA) in PCS
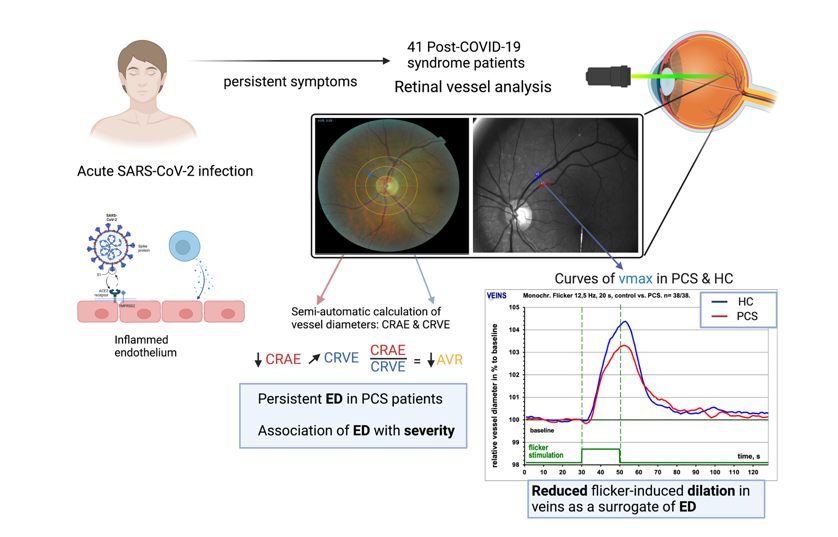
After matching, PCS patients showed significantly lower venular dilation after stimulation when compared to HC (vmax; 3.42% ± 1.77% vs. 4.64 % ± 2.59%; p = 0.02), suggesting a persistent alteration of microvascular endothelial function in PCS. There was no difference in arteriolar dilation (amax) between the two cohorts (amax; 3.26% ± 2.71 % vs. 3.25% ± 1.69 %; p = 0.98) (Fig. 1 a).
To assess retinal microvasculature in PCS patients, retinal fundus pictures were analyzed. PCS patients showed significantly narrower retinal arterioles, indicated by lower CRAE when compared with HC (178.1 [167.5 - 190.2] vs. 189.1 [179.4 - 197.2], p = 0.01). We did not observe differences in the central retinal venular equivalent (CRVE) between cohorts (213.1 [200.0 - 224.2] vs. 212.2 [197.1 - 220.8], p = 0.5). Subsequently, the arteriolar venular ratio (AVR) was significantly lower in PCS patients as it is the ratio of CRAE/CRVE (0.84 [0.8 - 0.9] vs. 0.88 [0.8 - 0.9], p = 0.007) (Fig. 1 b). After controlling for potential confounders, lower venular dilation (p = 0.03) and lower AVR (p = 0.048) remained associated with PCS. The strength of association with narrower retinal arterioles was smaller after adjustment (p = 0.077) (Table E1: Online Supplement).
To test whether RVA parameters could serve as a biomarker for PCS, we plotted receiver operated characteristics (ROC) curves and calculated the area under the curve (AUC) of variables. RVA parameters showed acceptable discrimination of the two cohorts for vmax (AUC: 0.61), CRAE (AUC: 0.67) and AVR (AUC: 0.67). When combining both parameters AVR and vmax in a logistic regression model the corresponding score reached good discrimination between HC and PCS patients (AUC: 0.75) (Fig. 1 c).
PCS severity amplifies changes of retinal microcirculation
In this PCS cohort, 34 (82.9%) patients were severely affected (PCS severity score >26.25), and 7 (17.1%) patients were moderately affected (PCS severity score >10.75 and ≤26.25). Severely affected patients were more obese (0.0% vs. 44.1 %; p = 0.04) and as expected, Fatigue Severity Scale (FSS) was higher (4.1 [3.6 - 5.8] vs. 6.1 [5.8 - 6.7], p = 0.02). Severely affected patients showed tendencies towards more PCS-related work loss (0% vs. 23.5%, p = 0.3) and cumulative days of sick leave (106.0 [0.0 - 157.0] vs. 122.5 [15.5 - 303.8], p = 0.2). Laboratory parameters showed no relevant differences between groups (Table E2: Online Supplement).
For DVA parameters, we did not see any relevant differences between moderately and severely affected patients (Fig. E2: Online Supplement). For SVA parameters, we observed a trend towards narrower retinal arterioles (CRAE) and broader retinal venules (CRVE), both failing to reach significance (Figure 2 a). AVR was significantly lower in severely affected PCS patients (0.83 [0.78 - 0.88] vs. 0.91 [0.87 - 0.94]; p = 0.02) and proved to be an excellent marker to discriminate between severely and moderately affected PCS patients (AUC:0.79) (Fig. 2 a and c).
Spearman’s correlation coefficient shows a negative, correlation between AVR and PCS Score (R= -0.37 p = 0.017) (Fig. 2 b) and the association of lower AVR with higher PCS score (p = 0.002) and severe phenotype (p = 0.03) remained significant after adjusting for potential confounders (Table 2).
Table 2 Association of AVR with PCS severity

Regression model shows potential confounders of RVA, PCS severity score and severe PCS phenotype as a univariatea model. The multivariate modelb was corrected for age, gender, obesity, arterial (Art.) hypertension and nicotine abuse and is shown for PCS severity score and severe PCS phenotype. All models are shown for the depended variable AVR. The respective R2 are shown for the multivariate modelb after correction. To fit a linear model, residuals were tested for normality.
Chronic fatigue in PCS and impairment of retinal microcirculation
Chronic fatigue is one of the most debilitating symptoms in PCS patients, and SARS-CoV-2 infection has been reported to cause ME/CFS [46]. We evaluated whether there is an association between RVA and ME/CFS.
In our cohort, 60.9% (25/41) of PCS patients met the Canadian Consensus Criteria for ME/CFS. PCS patients with CFS were more obese (12.5% vs. 52.0%, p = 0.02); other CV factors were not different. PCS patients with CFS had a higher PCS severity score (30.4 ±8.7 vs. 39.1 ±8.9, p = 0.004) and were more fatigued and depressed, indicated by higher FSS (5.8 [4.1 - 6.2] vs. 6.2 [5.8 - 6.9], p = 0.02) and higher PHQ9 score (8.9 ±4.6 vs. 11.8 ±4.1, p = 0.040). There were no relevant differences in laboratory values between the two groups (Table E3: Online Supplement).
We observed significantly narrower retinal arterioles in PCS patients with CFS, indicated by lower CRAE (183.5 [177.4 - 197.0] vs. 174.0 [161.5 - 181.0], p = 0.03). There was no difference in the size of retinal venules between groups (214.9 [204.1 - 221.9] vs. 211.1 [199.9 - 226.0], p = 0.98) (Fig. 3 a). AVR was significantly lower in PCS patients with CFS (0.88 [0.82 - 0.91] vs. 0.82 [0.77 - 0.86], p = 0.02), and both AVR (AUC: 0.72) and CRAE (AUC: 0.70) were good markers to distinguish between PCS patients with or without CFS (Fig. 3 a and b).
After controlling for confounders of SVA, association for lower AVR (p = 0.3) and narrower retinal arterioles (p=0.04) with CFS was smaller (Table E4: Online Supplement).
Association of chronic inflammation and microvascular alterations in PCS
Higher levels of CXCL10 (p = 0.01), D-Dimer (p = 0.03), and TAG (p = 0.03) were significantly associated with lower AVR. Narrower retinal arterioles showed no associations with inflammatory parameters, however, with higher levels of D-Dimer (p = 0.008) and TAG (p = 0.002). Wider retinal venules were significantly associated with higher levels of CXCL10 (p = 0.02) and IL-6 (p = 0.04) (Table 3). As we observed associations of inflammatory biomarkers with microcirculation parameters, we were interested, whether chronic inflammation would amplify our observed correlation between microvascular changes and PCS severity score. Therefore, we fitted a regression model with interaction effects between PCS severity score and laboratory parameters.
The described association between lower AVR and higher PCS severity scores was stronger in patients exhibiting higher levels of CXCL10 or IL-6. We observed interactions between CXCL10 and PCS-severity score (p < 0.001) and interactions between IL-6 and PCS severity score (p = 0.03) (Fig. 4 a). In line with this, the association between high PCS severity score and lower CRAE was more pronounced in PCS patients with higher CXCL10 levels (p < 0.001) and higher ferritin levels (p=0.04) (Fig. 4 b).
The association between higher CRVE and lower PCS severity was not influenced by CXCL10 and IL-6 (Fig. E3: Online Supplement).), however by higher neutrophil counts (p = 0.002) and lower lymphocyte counts (p = 0.002) (Fig. 4 c).
Table 3 Associations of laboratory parameters with variables of microcirculation

The multivariate linear regression model shows associations of laboratory parameters with the dependent variables AVR, CRAE, CRVE. D-Dimer was measured in n=36, thrombocytes and ferritin in n=37, TAG, CXCL10, IL8, IL-6, IgG4 and MCP-1 in n=38. In the multivariate modelb, age, gender, obesity, arterial hypertension and nicotine abuse were included. The respective R2 are shown for the multivariate modelb after correction. For modela F-statistic was not significant.
{kind=link}