Surgery for colon cancer with liver metastasis is a critical and controversial issue and continues to this day. Though most researchers believe that completed resection of both of primary and metastatic lesions would provide a survival advantage than systemic therapy, the mainly dispute is whether palliative resection of part of lesions is benefit for patients, especially resection only to primary colon cancer or liver metastasis[27]. What’s more, systemic chemotherapy, molecular targeted therapy, immunotherapy, portal vein or hepatic artery embolization and radiofrequency ablation play a gradually more important role in mCC treatment, which might provide a potentially longer survival and downstaging of tumor[5, 23, 27, 28]. This situation causes that surgery occupies a gradual weakening trend in CLM treatment, and many studies support the view that surgery would bring more trauma, stress and immunosuppression for CLM patients and probably prompt tumor growth, recurrence and wouldn’t bring survival benefit [24, 29–33]. However, there are also some studies stated clearly that resection primary colon cancer or liver metastasis associated with improved survival, and suggested a more aggressive method for the incurable diseases[23, 34–36].
This dilemma is amplifying in M-CLM, because MC is always characterized by peritoneal implant and metastases at multiple sites which increase difficulty of completed resection[18, 20, 37]. What’s more, most studies consider MC histology is an adverse prognostic for survival, as well as in M-CLM, which aggravate the concern of surgery[10, 15, 17]. However, the relatively low response to systemic therapy of MC compared with AC draws a dilemma in treatment of M-CLM, which evokes the rethinking of surgery in M-CLM[15, 37]. In this study, we found M-CLM also had general features as MC that such as more right colon location, larger tumor size and advanced pT and pN stage compared with A-CLM, but the long-term survival of overall M-CLM and A-CLM were comparable. These overturn the traditional knowledge of MC had poorer survival than AC, especially diagnosed at a high stage (III/IV)[14, 38]. However, our findings were consistent with some recent studies that survival of overall MC was poorer than AC, but stage IV MC had similar survival as AC[17, 39]. These findings indicated that though M-CLM had specific clinicopathological features, the long-term survival is comparable with A-CLM.
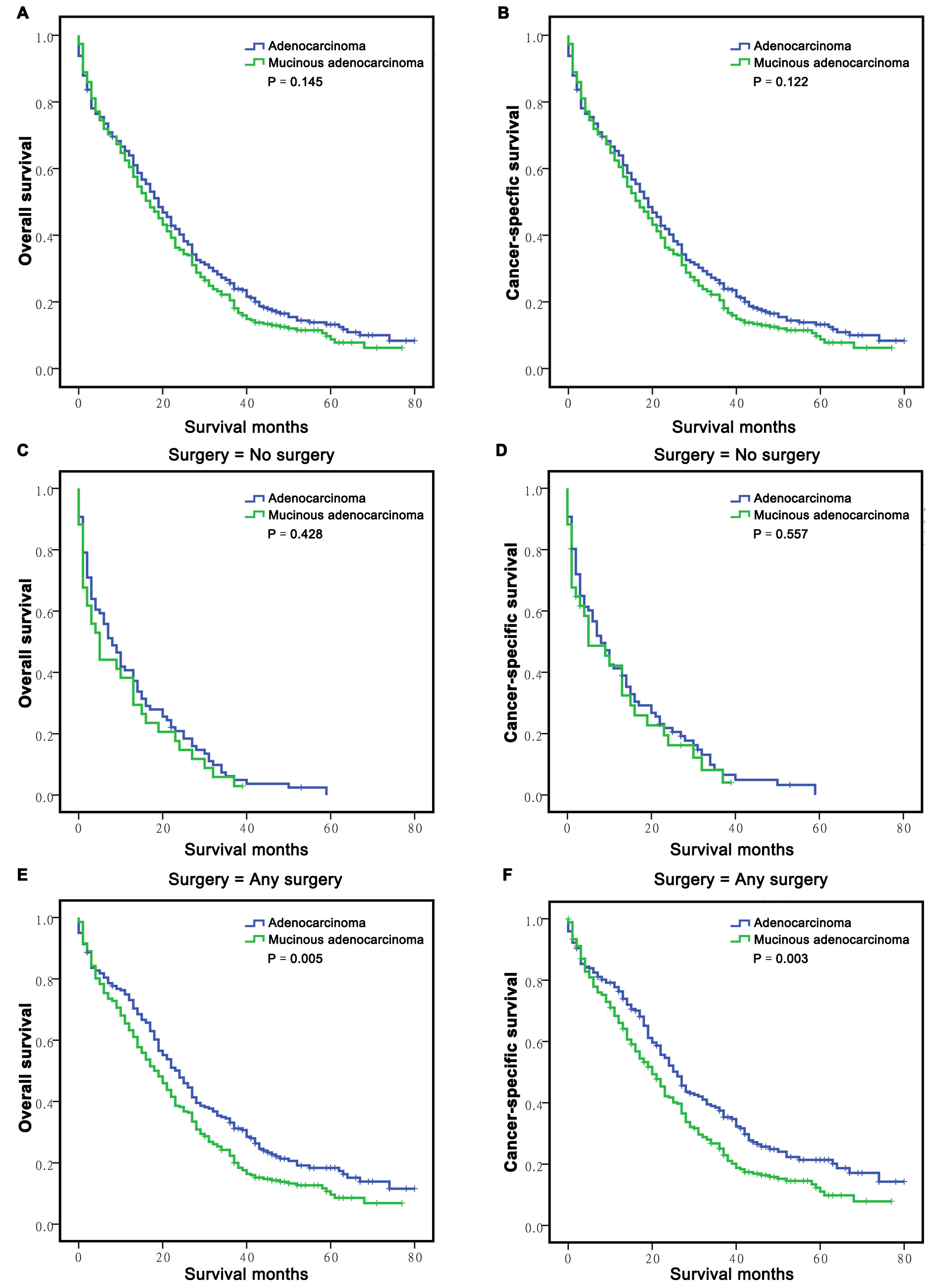
Another important finding of the present study was no matter surgery to both primary and metastatic lesions or only to any of the lesions of CLM patients, the survival were better than that of no surgery. This conclusion was also verified by stratification of M-CLM and A-CLM, and confirmed the importance of surgery for survival benefit of M-CLM, which was also supported by some former studies[34, 36]. We also explored the potential independent risk factors for survival of M-CLM by univariate and multivariate analyses. Results also showed surgery played a dominated role for favor OS and CSS, no matter surgery to both primary and metastatic lesions or any of the lesions. These results once again highlighted the importance of surgery for better prognosis of M-CLM. However, we further found M-CLM had the poorer OS and CSS than A-CLM in hierarchy of patients accepted any surgery. This finding was different from studies about surgery to stage IV MC[17, 40], but similar with a recent study from Italy that M-CLM associated with worse OS and disease-free survival[18]. One potential explanation for the discrepancy is the studies of stage IV MC didn’t stratify the sub-classification of M-CLM, since M-CLM always accompanied other sites and/or peritoneal metastasis which would deteriorate the prognosis[15, 18, 37]. Another possible reason is that adjuvant chemotherapy is an important option for postoperative treatment for M-CLM though this study didn’t include the information. However, M-CLM always resistant to systemic chemotherapy which might also lead to relatively poor survival after surgery[15, 41].
Surgery type of primary lesion is also a most debated issue for M-CLM, the most often types are partial colectomy and hemicolectomy or greater. Some surgeons tend to choose the partial colectomy cause M-CLM is a terminal stage and surgery couldn’t improve survival even bring poor prognosis[29–31]. However, others thought extended resection such as hemicolectomy or greater would provide a probability for subsequent curable resection or sensitivity for systemic chemotherapy, which might prolong survival[32, 35, 36]. In the present study, we found partial colectomy provided a similar OS and CSS as hemicolectomy or greater, this finding strengthened the concept of minimizing the trauma for advanced cancer. There are some potential speculation for this, it is most likely that the extended resection would have broken immune system and homeostasis, and sometimes even promoted tumor growth and metastasis[24]. Thus, a more appropriate surgery option should be selected carefully when an operation decision is made for M-CLM.
This study has found the important role of surgery for better survival of M-CLM. However, there were also some limitation in the study. First and foremost, we couldn’t obtain the pre- and/or post-operative systemic therapy information which would weaken the scientific and academic rigour. Secondly, this study couldn’t recognize which patients received primary and metastatic lesions resection synchronously or subsequently. Third, because our study enrolled patients with pathological confirmation and detailed staging information in the SEER database, which would exclude many metastatic disease patients without pathological diagnosis. Thus, more excellent designed retrospective and prospective multi-center studies are needed in the future to overcome these weaknesses.
Despite these limitations, this study concluded M-CLM had distinct clinicopathological characteristics from A-CLM, and highlighted surgery could improve the long-term survival and was the independent favorable prognostic factor for survival even though surgery to any lesion of M-CLM, in addition, partial colectomy might be a better selection for M-CLM from this study. In conclusion, our study updated the understanding of surgery for MAC of metastatic colon carcinoma.
{kind=link}