COVID-19 has been declared as global epidemic and currently there is no drug/vaccine available to treat COVID-19. All over the world, several studies are being conducted to discover the antiviral drugs against COVI-19. Traditional medicinal plants have long history to treat viral infections. We adopted in silico approach to find out if unique phytocompounds such as emodin (Rheum emodi), thymol and carvacrol (Thymus serpyllum) and artemisnin (Artemisia annua) could physically bind COVID-19 target proteins such as SARS-CoV-2 spike glycoprotein (PDB ID: 6VXX), SARS-CoV-2 spike ectodomain structure (PDB ID: 6VYB), and SARS coronavirus spike receptor-binding domain (PDB ID: 2AJF) and in turn preventCOVID-19 binding to the host receptor ACE2. Since Chloroquine (a standard antimalarial drug) has been looked as potential therapy against COVID-19, we also compared the binding of chloroquine and plant origin artemisnin antimalarial drug for its interaction with 6VXX, 6VY and 2AJF. Molecular docking studies using AutoDock/Vina software revealed that among all the phytocompounds artemisinin showed best binding affinity with 6VXX, 6VYB and 2AJF with Etotal -10.5 KJ mol-1, -10.3 KJ mol-1, and -9.1 KJ mol-1 respectively. Whereas emodin, carvacrol and thymol binds with 6VXX, 6VYB and 2AJF with Etotal -6.4, -6.8, -6.9 KJ mol-1, -8.8, -6.8, -7.4 KJ mol-1, and -6.9, -7.4, -7.2 respectively. Similarly, with Autodock/Vina chloroquine showed less binding affinity with 6VXX (-5.6 KJ mol-1), 6VYB (-5.9 KJ mol-1) and 2AJF (-6.4 KJ mol-1) as compared to all phytocompounds. Toxicity prediction showed non-toxicity and non-carcinogen by admetSAR and PROTOX‑II software.
Research Article
Phytocompounds of Rheum emodi, Thymus serpyllum and Artemisia annua inhibit COVID-19 binding to ACE2 receptor: In silico approach
https://doi.org/10.21203/rs.3.rs-30938/v1
This work is licensed under a CC BY 4.0 License
Version 1
posted
You are reading this latest preprint version
CoVID-19
Antimalarial drugs
chloroquine
Artemisnin
Phytocompounds
Emodin
Thymol
In silico
COVID-19 caused by a family of Coronavirus (CoV) has threatened the survival of Human beings on the Earth and it has been declared as global health emergency by World Health Organization (WHO) (Sohrabi et al., 2020). Coronavirus (CoV) comes under the family of viruses which has the ability to cause illness. It starts with the common cold and ends with more severe diseases such as Middle East Respiratory Syndrome (MERS-CoV) and Several Acute Respiratory Syndrome (SARS-CoV). A new strain novel corona virus (nCoV) has been come into knowledge which is mainly found in humans. In Latin, Corona means “halo” or “crown” thus the name represents the structure of the virus which consists of crown like projections on its surface (Islam, 2017). In 1937, corona virus was isolated from an infectious bronchitis virus in birds which was responsible to ruin the poultry stocks (Bracewell, 1977). Further, human corona virus was identified in the year 1960 in the nose of patient suffering from common cold and OC43 and 229E were the two human corona viruses responsible for common cold. Corona viruses are the type of viruses that directly affect the respiratory tract. These are associated with the common cold, pneumonia, gut as well as severe acute respiratory syndrome. Corona viruses are zoonotic, which means they are transmitted between animals and humans (Ksiazek et al., 2003).
The first case of Middle East respiratory syndrome (MERS-CoV) was seen in the year 2012, a businessman in Saudi Arabia who died from viral pneumonia (Zaki et al., 2012). Later, this disease started appearing in the people living outside the Saudi Arabia due to their close contact with individual living in other country (European Centre for Disease Prevention and Control, Severe respiratory disease associated with MERS-CoV, Stockholm: ECDC; 11 June 2015) in 2016, a report on 1698 was published by World Health Organization (WHO) regarding the confirmed cases of MERS-CoV infection and the death rate was approximately 36% (Middle East Respiratory Coronavirus (MERS-CoV) Bialek et al. (2014). The biggest outbreak with first ever confirmed case of this disease came into existence in the year 2015 in South Korea. Including the China, the confirmed cases extend to 186 with total 36 deaths (Cowling et al., 2015). Recently, case regarding the novel coronavirus came in to existence among the population of Wuhan, China on December 8, 2019. Pneumonia was the first symptom of infection and most of the cases were linked to a local fish and animal market. During the research it was seen that 2019 novel coronavirus was recognized as pathogenic agent responsible for evolution of pneumonia (Zhu et al., 2019). At the very first China was unaware about the direct transmission of 2019 novel coronavirus (2019-nCoV). However, patients without symptoms were recognized as the major source of infection as well as human-to-human transmission was also confirmed (Rothe et al., 2020). There was increase in the number of confirmed cases from 1 to 15. On January 20, 2020 laboratory in Korea confirmed the first case of Coronavirus. On 23 January, 2020, the government of China announced the total shutdown of country and advised the people for undergoing personal isolation. On 30 January, 2020, World Health Organization declared this problem as public health emergency of international concern (Sohrabi et al., 2020).
Virus particle consists mainly of four structural proteins. The spike (S), membrane (M), envelop (E), and proteins (N) are the four structural proteins which encodes with 3’ end of the viral genome (Wang et al., 2020; Zhou et al., 2018). Among all, S protein plays an important role in viral attachment, fusion, entry, and also act as a target for development of antibodies, entry inhibitors and vaccines (Du et al., 2009; Wang et al., 2016). The S1 domains of coronaviruses may contain receptor-binding domains (RBDs) that directly bind to the cellular receptors (Babcock et al., 2004; Wong et al., 2004). The SARS-CoV surface exhibit two components: S1, which contains the receptor binding domain (RBD); and S2, which contains the fusion peptide. SARS-CoV gains entry into cells through interaction of the SARS-SRBD with the cell surface receptor angiotensin converting enzyme 2 (ACE2) (Anand et al., 2003; Perlman et al., 2009). These interactions are followed by endocytosis, and at the low pH in endosomes, SARS-S is cleaved by a cellular protease called cathepsin L, thereby exposing the S2 domain of the spike protein for membrane fusion (Bosch et al., 2003; Yang et al., 2004). The minimal RBD of SARS-CoV S protein is located in the S1 subunit (AA 318–510) and is responsible for viral binding to host cell receptors (Dimitrov, 2003; Xiao et al., 2003). Besides the main receptor, angiotensin-converting enzyme 2, there are several alternative receptors, such as dendritic cell-specific intercellular adhesion molecule-3-grabbing non-integrin and/or liver/lymph node-specific intercellular adhesion molecule-3-grabbing integrin (DeDiego et al., 2011). SARS-CoV and MERS-CoV RBDs recognize different receptors. SARS-CoV recognizes angiotensin-converting enzyme 2 (ACE2) as its receptor, whereas MERS-CoV recognizes dipeptidyl peptidase 4 (DPP4) as its receptor (Li et al., 2003; Raj et al., 2013). Similar to SARSCoV, SARS-CoV-2 also recognizes ACE2 as its host receptor binding to viral S protein (Zhou et al., 2020). Two residues (AA 479 and AA 487) in RBD determine SARS progression and tropism, and their mutations may enhance animal-to-human or human-to-human transmission (Wong et al., 2004). Some residues (AA 109, 118, 119, 158, 227, 589 and 699) in S protein are critical strategies against this deadly viral agent, especially in high-risk groups, including people of every age group (Cinatl et al., 2003).According to the previous data, the ACE2 receptor expressing cell fused with SARS-S- expressing cells adds to the cell surface by pH independent mechanism (Xiao et al., 2003). It enhances the cell stress responses and apoptosis (Jeffers et al., 2004). Binding is very critical for pathogenesis if the binding is blocked, then COVID will not bind with Human cell receptor (ACE2), hence infection stopped. Traditional medicinal plants produce large number of compounds which is used as therapeutics to kill the pathogens (Iyengar, 1985). In the recent years so many reports published on antimicrobial activity of the medicinal plants. It is expected that plant extracts and phytocompounds showing the target site other than antibiotics, a very little information is available on this type of activity of medicinal plants (Hasegawa et al., 1995; Lee et al., 1998). Extracts of medicinal plants has been used from ancient times and these plants are known for their antiviral properties and less side effects. Traditionally, thyme was acclimated to treat asthma and loosen congestion in the throat and stomach (Heilmeyer, 2007). The pharmacological manuscript of Chailander medical codex (15th and 16th centuries) mentions the utilizations of wild thyme for the treatment of headaches caused by cold and laryngitis (Jaric et al., 2014). During the Renaissance period (16th and 17th centuries), wild thyme was utilized internally to treat malaria and epilepsy (Adams et al., 2012). Traditionally in many countries areal part of T. serpyllum utilized as anthelmintic, a vigorous antiseptic, an antispasmodic, a carminative, deodorant, diaphoretic, disinfectant, expectorant, sedative, and tonic (Chevallier, 1996). Thymus serpyllum additionally used to treat respiratory quandaries (Menkovic et al., 2011; Jarić et al., 2015). In western Balkans thymus species used to amend blood circulation and as anticholesterolemic, immunostimulant (Mustafa et al., 2015). Carvacrol and thymol are isomers, belonging to the group of monoterpenic phenols with potent antiseptic properties. Chauhan et al. (2010) reported thymol (25-200 mg kg-1) as immunomodulatory in cyclosporine –A, treated Swiss albino mice by enhancing the expression of cluster of differentiation 4 (CD4), cluster of differentiation 8 (CD 8) and Th1 cytokines via upragulation of IFN-4expression and enhanced secreation of interleukin -12 (IL-12). Thymol increase the production of antibody titers against the Nwcastle diseases virus in broiler chickens (Khajeal et al., 2012).
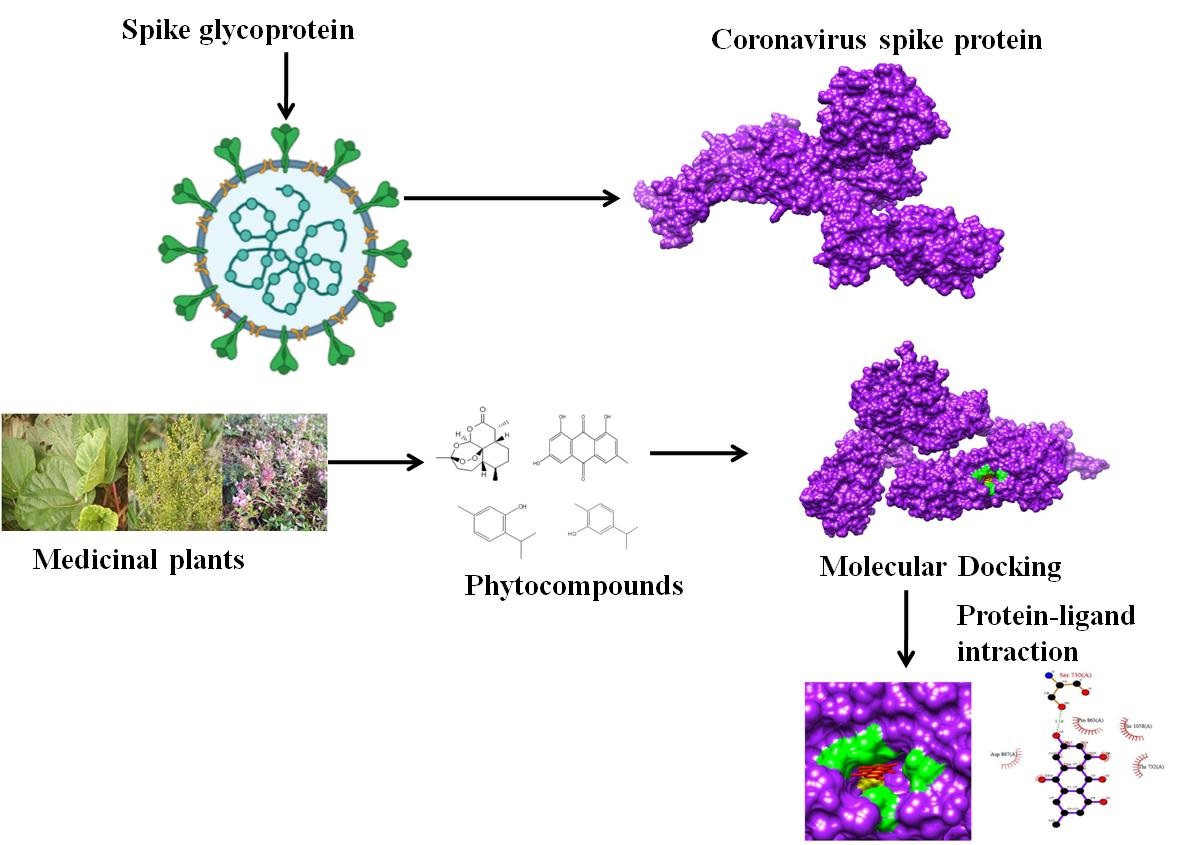
Antiviral property of Thymus serpyllum (Herrmann et al., 1969) and thymol is already reported (Rustaiyan et al., 2000). Pilau et al. (2011) reported the antiviral activity of carvacrol from Lippia graveolens against human and animal virus (herpes simplex virus, acyclovir-resistant herpes simplex virus 1, bovine herpesvirus 2, respiratory syncytial virus; human rotavirus, bovine viral diarrhoea virus). Antiviral nature of Emodin was also reported in several studies (Hsiang and Ho, 2008; Dai et al., 2017; Zhu et al., 2019). Study from Efferth et al. (2008) showed in vitro antiviral properties of artemisinin against Hepatitis B virus, Hepatitis C virus and Bovine viral diarrhea. Keeping in view the antiviral potential of Himalayan herbs, the current study was focused on the identification of potent phytocompounds from Himalayan herbs (Rheum emodi, Thymus serpyllum and Artemisia annua) to cure a dangerous COVID-19 (Fig. 1).
Bioinformatics tools: Open Babel GUI (O'Boyle et al., 2011), UCSF Chimera 1.8.1(Pettersen et al., 2004), Pubchem (www.pubchem.com), RCSB PDB (http://www.rscb.org/pdb), PDBsum (www.ebi.ac.uk/pdbsum), and Autodock software (Trott and Olson, 2010) were used in the present investigation.
Ligand preparation
Four major phytocompounds of three medicinal plants- emodin of Rheum emodi, thymol, and carvacrol of Thymus serpyllum and artemisnin of Artemisia annua were used for the docking studies. The 3-dimensional structures of all the phytocompounds and chloroquine were obtained from pubchem (www.pubchem.com) in .sdf format. The .sdf file of the phytocompounds was converted into PDB and pdbqt format by using the Open Babel tool (Wang et al., 2009). Table-1 showed molecular structure, molecular weight, pharmacological properties, plant source, percentage of phytocompounds in plant and antimalarial drug chloroquine. Tragets of phytocompounds and standard drug chloroquine was predicted by using SwissADME online server.
Table 1: Molecular structure, molecular weight, and pharmacological properties plant source and percentage of selected phytocompounds and chloroquine.
|
Name of phytocompounds |
Plant source |
Molecular structures |
Percentage (%) of phytocompounds in plants |
Molecular weight (g mol-1) |
Pharmacological properties |
|
Emodin |
Rheum emodi |
|
23.24 (Rolta et al., 2020) |
270.24 |
Antiviral (Schwarz et al., 2011), antimicrobial (Cao et al., 2015) |
|
Artemisinin |
Artemesia annua |
|
0.77–1.06 (Castilho et al., 2008) |
282.33 |
Antimalarial (Tu youyou, 2011); Antiviral ( Efferth et al., 2008) |
|
Thymol |
Thymus serpyllum |
|
8.3 (Gul et al., 2018) |
150.22 |
Antiseptic, antibacterial, antifungal and antioxidant properties (Jeric et al., 2015), Antivirotic (Rustaiyan et al., 2000) |
|
Carvacrol |
Thymus serpyllum |
|
3.03 (Gul et al., 2018) |
150.22 |
Antimicrobial, antithrombotic, anti-inflammatory, acetyl cholinesterase inhibitory properties (Jeric et al., 2015), Antiparasitic (Can Baser, 2008), Antiviral (Pilau et al., 2011) |
|
Chloroquine |
Standred antimalarial drug |
|
Standard Antimalarial drug |
319.9 |
FDA is allowing the use hydroxychloroquine treat coronavirus disease 2019 (COVID-19) (Jaffe, 2020). |




Protein preparation
Three target proteins of COVID-19 were SARS-CoV-2 spike glycoprotein (PDB ID: 6VXX) and SARS-CoV-2 spike ectodomain structure (PDB ID: 6VYB) (Walls et al., 2020) and SARS coronavirus spike receptor-binding domain, (PDB ID: 2AJF) (Li et al., 2005) were used to analyze the interactions of major phytocompounds of R. emodi, T. serpyllum and A. annua. The 3-Dimensional structures of selected target proteins were retrieved from PDB (Protein Data Bank) (http://www.rscb.org/pdb). Both proteins had co-crystallized ligand (X-ray ligand) in their binding site. The complexes bound to the receptor molecule, such as non-essential water molecules, including heteroatoms were removed from the target receptor molecule and hydrogen atoms were added to the target receptor molecule. Active site of three target proteins of COVID-19 were SARS-CoV-2 spike glycoprotein (PDB ID: 6VXX) and SARS-CoV-2 spike ectodomain structure (PDB ID: 6VYB) and SARS coronavirus spike receptor-binding domain was determined by grid box generation. Grid box was generated by adjusting the grid parameter (X, Y, Z coordinates values) using AutoDock software. The grid values were recorded in the config.txt file format. Three dimensional structures of target proteins of COVID-19 proteins are shown in Fig. 2.
ADMET and toxicity prediction of phytocompounds
Absorption, distribution, metabolism, excretion, and toxicity (ADMET) screening was done to determine the absorption, toxicity, and drug-likeness properties of the ligands.The 3-Dimensional structures of ligands such as emodin, thymol carvacrol, artemisinin and chloroquine were saved in .smiles format and drug were uploaded on SWISSADME (Molecular Modeling Group of the SIB (Swiss Institute of Bioinformatics), Lausanne, Switzerland), admetSAR (Laboratory of Molecular Modeling and Design, Shanghai, China), and PROTOX webservers (Charite University of Medicine, Institute for Physiology, Structural Bioinformatics Group, Berlin, Germany) for ADMET screening. SWISSADME is a web tool used for the prediction of ADME and pharmacokinetic properties of a molecule. The predicted result consists of lipophilicity, water solubility, physicochemical properties, pharmacokinetics, drug‑likeness, medicinal chemistry, and Brain or Intestinal Estimated permeation method (blood–brain barrier and PGP ± prediction) (Dainaet al., 2017). admetSAR provides ADMET profiles for query molecules and can predict about fifty ADMET properties. Toxicity classes are as follows: (i) Category I contains compounds with LD50 values ≤ 50 mg kg-1, (ii) Category II contains compounds with LD50 values > 50 mg kg-1 but 500 mg kg-1 but 5000 mg kg-1 (Cheng et al., 2012; Yang et al., 2019). PROTOX is a Rodent oral toxicity server predicting LD50 value and toxicity class of query molecule. The toxicity classes are as follows: (Class 1: fatal if swallowed (LD50 ≤5), Class 2: fatal if swallowed (55000) (Banerjee et al., 2018).
Docking of COVID-19 receptors and phytocompounds
The docking of selected ligands to the catalytic triad of protein was performed by using AutoDock/Vina (Trott and Olson, 2010). Docking was performed to obtain populations of conformations and orientation for ligands at binding sites. Docking was performed to study the interactions between COVID-19 receptors 6VXX, 6VYB and receptor binding domain (2AJF) with major phytocompounds of R. emodi, T. serpyllum and A. annua and .pdb file of proteins-ligand complexes were generated. All bonds of ligands were set to be rotatable. All calculations for ligand flexible protein-fixed docking were performed using the Lamarckian Genetic Algorithm (LGA) method. The best conformation was chosen with the lowest docked energy, after the completion of docking search. The .pdb complex of protein and ligands were analyzed by PDBsum (www.ebi.ac.uk/pdbsum) to study the list of interactions between protein and ligands. Detailed visualization and comparison of the docked sites of target proteins and ligands were done by using Chimera (Pettersen et al., 2004) and LigPlot (Laskowski and Swindells, 2011). Schematic representation experiments are shown in Fig. 2.
ADMET prediction and toxicity analysis of selected phytocompounds
The comparative ADME properties predicted by SwissADME of selected phytocompounds and drug Chloroquine are summarized in Table 2. Consensus Log Po/w value of ˂5 indicates good aqueous solubility, which means that an adequate amount of drug can reach and be maintained inside the body through oral administration. All the selected phytocompounds have consensus Log Po/w value of < 5 (Table 2). TPSA indicates permeability of compounds into the cells. A TPSA value of < 140 Å2 is required for good permeation of compound into the cell membrane and value < 90 Å2 is required to permeate through blood–brain barrier. All the selected phytocompounds have TPSA value < 90 Å2, except 94.83 for emodin, indicating good permeability of selected phytocompounds through blood–brain barrier. Lipinski’s rule of five helps to determine drug‑likeness of the compound; an orally active drug should not violate the Lipinski’s rule. All the ligands follow Lipinski’s rule of five (Table 2) and active site of phytocompounds are shown in Table 3.
Table 2: ADME properties of selected phytocompounds and Chloroquine predicted by SwissADME.
|
Phytocompounds |
SwissADME |
||||||||
|
Consensus Log PO/W |
Water Solubility |
GI Absorption |
TPSA (Å2) |
Lipinski Rule |
Ghose Rule |
Veber Rule |
Egan Rule |
Muegge Rule |
|
|
Emodin |
1.87 |
S |
H |
94.83 |
Y |
Y |
Y |
Y |
Y |
|
Thymol |
2.8 |
S |
H |
20.23 |
Y |
No |
Y |
Y |
No |
|
Carvacrol |
2.82 |
S |
H |
20.83 |
Y |
No |
Y |
Y |
No |
|
Artemisnin |
2.50 |
S |
H |
53.99 |
Y |
Y |
Y |
Y |
Y |
|
Chloroquine |
4.15 |
MS |
H |
28.16 |
Y |
Y |
Y |
Y |
Y |
Y: Yes; H: High; S: Soluble; MS: Moderate Soluble
Table 3: Predicted targets of phytocompounds and standard drug chloroquine
|
Name of phytocompounds |
Predicted Targets |
|
Emodin |
Estrogen receptor alpha, Estrogen receptor beta, Serine/threonine-protein kinase PIM1, Casein kinase II alpha, Protein-tyrosine phosphatase 4A3 |
|
Artemisinin |
Cytochrome P450 1A2 |
|
Thymol |
Transient receptor potential cation channel subfamily A member 1, Cyclooxygenase-1, GABA-A receptor; alpha-1/beta-2/gamma-2, Serotonin 2b (5-HT2b) receptor, GABA-A receptor; alpha-1/beta-3/gamma-2 |
|
Carvacrol |
Cyclooxygenase-1, Transient receptor potential cation channel subfamily A member 1, Serotonin 2b (5-HT2b) receptor, Carbonic anhydrase II, GABA-A receptor; alpha-1/beta-3/gamma-2, |
|
Chloroquine |
Voltage-gated calcium channel alpha2/delta subunit 1, Serotonin 1a (5-HT1a) receptor, Histamine H3 receptor, Histamine N-methyltransferase , Alpha-1d adrenergic receptor |
Toxicity of the phytocompounds and Chloroquine was predicted by PROTOX‑II and admetSAR and results are summarized in Table 4. It was observed that all the selected phytocompounds are non-carcinogenic and non-cytotoxic in nature and are safe to administer. However, LD50 value of emodin and artemisinin calculated from Protox II was higher than that of all other phytocompounds and chloroquine, indicating that these natural phytocompounds are safer than that of chemically synthesized chloroquine.
Table 4: Toxicity prediction of phytocompounds and Chloroquine predicted by admetSAR and PROTOX‑II software
|
Compounds
|
admet SAR |
Protox II |
||
|
Carcinogens |
Rate Acute toxicity (LD50) kg/mol |
LD50, (mg/kg) |
Cytotoxicity |
|
|
Emodin |
non-carcinogen |
2.5826 (III) |
5000 (Class 5) |
Inactive |
|
Thymol |
non-carcinogen |
2.202 (III) |
640 (Class 4) |
Inactive |
|
Carvacrol |
non-carcinogen |
2.531 (III) |
1190 (Class 4) |
Inactive |
|
Artemisinin |
non-carcinogen |
1.79 (V) |
4228 (Class 5) |
Inactive |
|
Chloroquine |
non-carcinogen |
2.684 (II) |
311 (Class 4) |
Inactive |
Molecular Docking analysis of phytocompounds and Chloroquine with spike receptors and receptor binding domain of COVID-19
Docking results with selected molecular targets of covid-19 spike protein i.e. SARS-CoV-2 spike glycoprotein (6VXX), SARS-CoV-2 spike ectodomain structure (6VYB), and SARS coronavirus spike receptor binding domain (2AJF) showed that selected phytocompounds had a good binding affinity and better binding modes than that of standard drugs chloroquine. All the 4 phytocompounds the best binding affinity, among all the phytocompound artemisinin (-10.5 kcal mol-1) showed the best followed by thymol (-6.9 kcal mol-1), carvacrol (-6.8 kcal mol-1), emodin (-6.4 kcal mol-1) and chloroquine (-5.6 kcal mol-1) with SARS-CoV-2 spike glycoprotein (6VXX) (Table 5, fig. 3 and S1).
In case of SARS-CoV-2 spike ectodomain structure (6VYB) artemisinin (10.3 kcal mol-1 ) showed best binding affinity followed by emodin (-8.8 kcal mol-1), carvacrol (-6.8 kcal mol-1), thymol (-6.7 kcal mol-1) and chloroquine (-5.9 kcal mol-1) (Table 5 and fig. 4 and S2).
In case of SARS coronavirus spike receptor binding domain (2AJF) artemisinin (-9.1 kcal mol-1) followed by carvacrol (7.4 kcal mol-1), thymol (-7.2 kcal mol-1), emodin (6.4 kcal mol-1) and chloroquine (6.4 kcal mol-1) (Table 5, fig. 5 and S3).
Furthermore, nature of hydrogen bonds was determined on the basis of donor-acceptor distances in protein secondary structure elements. Jeffrey and Jeffrey (1997) categorizes hydrogen bonds with donor-acceptor distances of 2.2-2.5 Å as "strong, 2.5-3.2 Å as "moderate (mostly electrostatic), and 3.2-4.0 Å as "weak, electrostatic". Hydrogen bond interaction, and hydrophobic interactions of these phytocompounds with all receptors were analyzed through Ligplot and summarized in table 5.
Table 5: E-total of ligands (emodin, thymol, carvacrol artemisnin and chloroquine) with COVID-19 targets by using Autodock vina software.
|
Receptor |
Ligands |
E total (kcal mol-1) |
Interacting amino acids |
|
|
H-bonding |
Hydrophobic interaction |
|||
|
SARS-CoV-2 spike glycoprotein (6VXX) |
Emodin |
-6.4 |
SER 1003, ARG 1014 (weak) |
GLN 1010, ALA 958, THR 1006, TYR 1007, THR 961, GLN 965 |
|
Thymol |
-6.9 |
- |
NO INTRACTION |
|
|
Carvacrol |
-6.8 |
HIS 1058, ALA 1056 (moderate) |
THR 778, GLY 1059, PHE 782, ILE 870, LEU 865, PRO 863, SER 730 |
|
|
Artemisnin |
-10.5 |
THR 778, SER 730 (week) |
LEU 865, PHE 782, ASP 867, PRO 863, HIS 1058, ILE 870. ALA 1056GLY 1059, VAL 729 |
|
|
Chloroquine |
-5.6 |
VAL 826 (weak) |
THR 778, SER 730, PRO 863, ALA 1056, ILE 870, ASP 867, LEU 867, HIS 1058, PRO 1057, PHE 823, THR 827 |
|
|
SARS-CoV-2 spike ectodomain structure (6VYB) |
Emodin |
-8.8 |
THR 778, SER 730 (weak) |
VAL860, LEU 861, THR 732, LYS 733, PRO 863, MET 731, HIS 1058, ALA 1056, ASP 867, PHE 823 |
|
Thymol |
-6.7 |
SER 730, THR 778 (moderate) |
LEU 865, PRO 863, PHE 782, ILE 870, ALA 1056, GLY 1059 |
|
|
Carvacrol |
-6.8 |
SER 730, THR 778 (moderate) |
VAL 729, PHE 782, ILE 870, ASP 867, ALA 1056, GLY 1059, LEU 865 |
|
|
Artemisnin |
-10.3 |
SER 730, THR 778 (weak) |
HIS 1058, ALA 1056, GLY 1059, VAL 729, PRO 863, LEU 865, PHE 782, ILE 870, ASP 867 |
|
|
Chloroquine |
-5.9 |
SER 730, HIS 1058 (weak) |
PRO863, PRO 1057, ALA 1056, ASP 867, THR 827 |
|
|
SARS coronavirus spike receptor-binding domain (2AJF) |
Emodin |
-6.9 |
TYR 385 (weak) |
HIS 401, HIS 378, ASP 382, ALA 348, ASP 350, TRP 349, PHE 40 |
|
Thymol |
-7.2 |
- |
GLU 232, PRO 235, LEU 236, PHE 592, GLU 589, LEU 585 |
|
|
Carvacrol |
-7.4 |
GLU 589 (moderate) |
LEU 236, GLU 232, PHE 592, LEU 585, PRO 235 |
|
|
Artemisnin |
-9.1 |
- |
PHE 390, ARG 393, ASP 350, PHE 40 |
|
|
Chloroquine |
-6.4 |
ASN 394 (moderate) |
LEU 73, ALA 99, LEU 100, TRP 69, PHE 390, ARG 393, ASP 350, PHE 40 |
|
From the beginning of 21st century, three corona viruses have crossed the species barrier and resulted in deadly pneumonia in humans: severe acute respiratory syndrome coronavirus (SARS-CoV) (Ksiazeket al., 2003), Middle-East respiratory syndrome coronavirus (Zakiet al., 2012) (MERS-CoV) and SARS-CoV-2 (Huang et al., 2020; Zhu et al., 2020). Nowadays, SARS-CoV-2 has been caused death of approximately 75,000 people all around the world. There is no specific antiviral treatment recommended for COVID-19, and no vaccine is currently available. The treatment is symptomatic, and oxygen therapy represents the major treatment intervention for patients with severe infection. Mechanical ventilation may be necessary in cases of respiratory failure refractory to oxygen therapy, whereas hemodynamic support is essential for managing septic shock. Researchers from worldwide are continuing to work on developing vaccine against Covid-19. Professor Didier Raoult from infectious diseases institute, IHU Méditerranée Infection in Marseille (France) has reported successful results from a new treatment for Covid-19, with early tests suggesting it can stop the virus from being contagious in just six days. Chloroquine phosphate and hydroxychloroquine have previously been used to treat coronavirus patients in China, in ongoing COVID-19 clinical trials. Kaletra, a US-based antiviral drug used to treat HIV, is another medicine that is being tested in the fight against the deadly virus. Emodin act as inhibitor of 3a ion channel of corona virus SARS-CoV and HCoV-OC43 as well as virus release from HCoV-OC43. They reported emodin is a potent inhibitor of the 3a channel with a K1/2 value of about 20 M. The reduction of extracellular viral RNA copies by emodin reflects inhibition of virus release. At high concentrations of emodin also intracellular levels of viral RNA copies were reduced suggesting that the high concentrations may also inhibit other stages of the virus life cycle (Schwarz et al. 2011). Ho et al. (2007) identified emodin as an effective to block the interaction of the SARS-CoV S protein with the ACE2 and the infection by S protein-pseudo-typed retrovirus. Similar to our study, Kumar et al (2020) reported the binding affinity of Nelfinavir (‐8.4), Rhein (‐8.1), Withanolide D (‐7.8), Withaferin A (‐7.7), Enoxacin (‐7.4), and Aloe‐emodin (‐7.4) with COVID 19 main protease (6LU7).
Present study proposed safe and less toxic phytocompounds for the treatment for COVID-19, which can be further validated through in vitro and in vivo studies.
Contribution: All the experimental work was done by Er Rajan Rolta and Ms. Deeksha Salaria. Dr Vikas Kumar provided the technical inputs. Dr Anuradha Sourirajan and Dr Kamal Dev conceived the idea and provided guidance to execute the research project. All the authors have read the manuscript.
Acknowledgements: The authors acknowledge Shoolini University, Solan, for providing infrastructure support to conduct the research work. Authors also acknowledge the support provided by Yeast Biology Laboratory, School of Biotechnology, Shoolini University, Solan, India.
Competing interests: The authors declare no competing interests.
- Anand, K., Ziebuhr, J., Wadhwani, P., Mesters., J.R., Hilgenfeld. R., 2003. Coronavirus main proteinase (3CLpro) structure: basis for design of anti-SARS drugs. Science. 300, 1763-7. https://doi.org/1126/science.1085658
- Babcock, G.J., Esshaki, D.J., Thomas, W.D. and Ambrosino, D.M., 2004. Amino acids 270 to 510 of the severe acute respiratory syndrome coronavirus spike protein are required for interaction with receptor. Journal of 78, 4552-4560. https://doi.org/10.1128/JVI.78.9.4552-4560.2004
- Banerjee, P., Eckert, A.O., Schrey, A.K. and Preissner, R., 2018. ProTox-II: a webserver for the prediction of toxicity of chemicals. Nucleic acids research, special publication. 46, W257-W263. https://doi.org/10.1093/nar/gky318
- Bialek, S.R., Allen, D., Alvarado-Ramy, F., Arthur, R., Balajee, A., Bell, D., Best, S., Blackmore, C., Breakwell, L., Cannons, A., Brown, C., 2014. First confirmed cases of Middle East respiratory syndrome coronavirus (MERS-CoV) infection in the United States, updated information on the epidemiology of MERS-CoV infection, and guidance for the public, clinicians, and public health authorities—May 2014. MMWR. Morbidity and Mortality Weekly Report. 16, 63:431.
- Bosch, B.J., Vander, Z.R., de HAAn, C.A., Rottier, P.J., 2003. The coronavirus spike protein is a class I virus fusion protein: structural and functional characterization of the fusion core complex. Journal of Virology 77, 8801-11. https://doi.org/10.1128/JVI.77.16.8801-8811.2003
- Bracewell, CD., 1977. Serological studies of avian infectious bronchitis virus.
- Can Baser, K.H., 2008. Biological and pharmacological activities of carvacrol and carvacrol bearing essential oils. Current Pharmaceutical Design 14: 3106-19. https://doi.org/10.2174/138161208786404227
- Cao, F., Peng, W., Li, X., Liu, M., Li, B., Qin, R., Jiang, W., Cen, Y., Pan, X., Yan, Z., Xiao, K., 2015. Emodin is identified as the active component of ether extracts from Rhizoma PolygoniCuspidati, for anti-MRSA activity. Canadian Journal of Physiology and Pharmacology 93, 485-93. https://doi.org/10.1139/cjpp-2014-0465
- Castilho PC, Gouveia SC, Rodrigues AI. Quantification of artemisinin in Artemisia annua extracts by 1H‐ Phytochemical Analysis. 2008, 19: 329-34. https://doi.org/10.1002/pca.1053
- Cinatl, J., Morgenstern, B., Bauer, G., Chandra, P., Rabenau, H., Doerr, H.W., 2003. Glycyrrhizin, an active component of liquorice roots, and replication of SARS-associated coronavirus. The Lancet. 361, 2045-6. https://doi.org/10.1016/S0140-6736(03)13615-X
- Cowling, B.J., Park, M., Fang, V.J., Wu, P., Leung, G.M., Wu, J.T., 2015. Preliminary epidemiologic assessment of MERS-CoV outbreak in South Korea, May–June 2015. Euro surveillance: bulletin Europeen sur les maladies transmissibles. Eurosurveillance 20, 21175. https://dx.doi.org/10.2807%2F1560-7917.es2015.20.25.21163
- Dai, J.P., Wang, Q.W., Su, Y., Gu, L.M., Zhao, Y., Chen, X.X., Chen, C., Li, W.Z., Wang, G.F., Li, K.S., 2017. Emodin inhibition of influenza A virus replication and influenza viral pneumonia via the Nrf2, TLR4, p38/JNK and NF-kappaB pathways Molecules. 22:1754. https://doi.org/10.3390/molecules22101754
- DeDiego, M.L., Nieto-Torres, J.L., Jiménez-Guardeño, J.M., Regla-Nava, J.A., Alvarez, E., Oliveros, J.C., Zhao, J., Fett, C., Perlman, S., Enjuanes, L., 2011. Severe acute respiratory syndrome coronavirus envelope protein regulates cell stress response and apoptosis. PLoSPathog 7, e1002315. https://dx.doi.org/10.1371%2Fjournal.ppat.1002315
- Dimitrov, D.S., 2003. The secret life of ACE2 as a receptor for the SARS virus. Cell 115, 652-53. https://doi.org/10.1016/S0092-8674(03)00976-0
- Du, L., He, Y., Zhou, Y., Liu, S., Zheng, B.J. and Jiang, S., 2009. The spike protein of SARS-CoV—a target for vaccine and therapeutic development. NatureReviews Microbiology 7, 226-236. https://doi.org/10.1038/nrmicro2090
- Efferth, T., Romero, M.R., Wolf, D.G., Stamminger, T., Marin, J.J., Marschall, M., 2008. The antiviral activities of artemisinin and artesunate. Archives of Clinical Infectious Diseases 47: 804-11.
- Gul, R., Jan, S.U., Taimor. M., Rabbani. T., Jahan, N., 2018. Validation of a hHigh Performance Liquid Chromatography Technique for the investigation of Thymol and Carvacrol in Thymus serpyllum indigenous to balochistan. Indo American Journal of PharmaceuticalSciences 5: 7429-35.
- Hajeali Y., Kheiri F., Rahimian Y., Faghani M., Namjo A. (2012). Effect of use different levels of caraway (Carum carvi) powder on performance, some blood parameters and intestinal morphology on broiler chickens.World Applied Sciences Journal 19 1202–1207.
- Hasegawa, H., Matsumya, S., Yamasak, K., 1995. Reversal of efflux mediated tetracycline resistance in Staphylococcus aureus clinical isolates by Ginseng prosaponenins. PhytotherapyResearch 9, 260–263. https://doi.org/10.1002/ptr.2650090406
- Heilmeyer M. Ancient herbs. Getty Publications; 2007.
- Herrmann, Jr. E.C., Kucera, L.S., 1967. Antiviral Substances in Plants of the Mint Family (Labiatae). III. Peppermint (Mentha piperita) and other Mint Plants. Proceeding of the Society for Experimental Biology and medicine 124, 874-8.
- Ho, T.Y., Wu, S.L., Chen, J.C., Li, C.C. and Hsiang, C.Y., 2007. Emodin blocks the SARS coronavirus spike protein and angiotensin-converting enzyme 2 interaction. Antiviral research 74: 92-101. https://doi.org/10.1016/j.antiviral.2006.04.014
- Hsiang, C.Y., Ho, T.Y., 2008. Emodin is a novel alkaline nuclease inhibitor that suppresses herpes simplex virus type 1 yields in cell cultures. British Journal of Pharmacology 155, 227-35. https://doi.org/10.1038/bjp.2008.242
- Huang, C., Wang, Y., Li, X., Ren, L., Zhao, J., Hu, Y., Zhang, L., Fan, G., Xu, J., Gu, X. and Cheng, Z., 2020. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The Lancet. 395, 497-506. https://doi.org/10.1016/S0140-6736(20)30183-5
- Islam, M.T., 2017. Studies on coronaviruses causing enteric infections in domestic animals in Japan.
- Iyengar, M.A., 1985. Study of Crude Drugs, 2nd edn. College of Pharmaceutical Sciences, Manipal, pp. 13–78.
- Jaffe S. Regulators split on antimalarials for COVID-19. The Lancet. 2020, 395: 1179. https://doi.org/10.1016/S0140-6736(20)30817-5.
- JJarić, S., Mitrović, M., Pavlović, P., 2015. Review of ethnobotanical, phytochemical, and pharmacological study of Thymus serpyllum Journal profile Evidence-Based Complementaryand Alternative Medicine 2015. https://doi.org/10.1155/2015/101978
- Jeffers, S.A., Tusell, S.M., Gillim-Ross, L., Hemmila, E.M., Achenbach, J.E., Babcock, G.J., Thomas, W.D., Thackray, L.B., Young, M.D., Mason, R.J., Ambrosino, D.M., 2004. CD209L (L-SIGN) is a receptor for severe acute respiratory syndrome coronavirus. Proceedings of the National Academyof Sciences 101, 15748-53. https://doi.org/10.1073/pnas.0403812101
- Jeffrey, G.A., Jeffrey, G.A., 1997. An introduction to hydrogen bonding. New York: Oxford university press. 12, pp. 228.
- Ksiazek, T.G., Erdman, D., Goldsmith, C.S., Zaki, S.R., Peret, T., Emery, S., Tong, S., Urbani, C., Comer, J.A., Lim, W., Rollin, P.E., 2003. A novel coronavirus associated with severe acute respiratory syndrome. New England Journal of Medicine 348, 1953-66. https://doi.org/1056/NEJMoa030781
- Kumar D, Chandel V, Raj S, Rathi B. In silico identification of potent FDA approved drugs against Coronavirus COVID-19 main protease: A drug repurposing approach. Chemical Biology Letters. 2020, 7: 166-75.
- Laskowski, R.A., Swindells, M.B., 2011. LigPlot+: multiple ligand–protein interaction diagrams for drug discovery. Journal of Chemical Information 51, 2778-86. https://doi.org/10.1021/ci200227u
- Lee, C.K., Kin, H., Moon, K.H., Shun, K.H., 1998. Screening and isolation of antibiotic resistance inhibitors from herb materials - resistance inhibition of volatile components of Korean aromatic herbs. Archives of Pharmacal Research 21, 62–66.
- Li, F., Li, W., Farzan, M., Harrison, S.C., 2005. Structure of SARS coronavirus spike receptor-binding domain complexed with its receptor. 5742, 1864-1868. https://doi.org/10.1126/science.1116480
- Li, W., Moore, M.J., Vasilieva, N., Sui, J., Wong, S.K., Berne, M.A., Somasundaran, M., Sullivan, J.L., Luzuriaga, K., Greenough, T.C., Choe, H., 2003. Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature 426, 450-4. https://doi.org/10.1038/nature02145
- O'Boyle, N.M., Banck, M., James, C.A., Morley, C., Vandermeersch, T., Hutchison, G.R. 2011. Open Babel: An open chemical toolbox. Journal of Cheminformatics 3, 33.
- Perlman, S., Netland, J., 2009. Coronaviruses post-SARS: update on replication and pathogenesis. NatureReviews Microbiology 7, 439-50. https://doi.org/10.1038/nrmicro2147
- Pettersen, E.F., Goddard, T.D., Huang, C.C., Couch, G.S., Greenblatt, D.M., Meng, E.C. and Ferrin, T.E., 2004. UCSF Chimera—a visualization system for exploratory research and analysis. Journalof Computational Chemistry 25, 1605-1612. https://doi.org/10.1002/jcc.20084
- Pilau, M.R., Alves, S.H., Weiblen, R., Arenhart, S., Cueto, A.P., Lovato, L.T., 2011. Antiviral activity of the Lippiagraveolens (Mexican oregano) essential oil and its main compound carvacrol against human and animal viruses. Brazilian Journal of Microbiology 42, 1616-24.
- Raj, V.S., Mou, H., Smits, S.L., Dekkers, D.H., Müller, M.A., Dijkman, R., Muth, D., Demmers, J.A., Zaki, A., Fouchier, R.A. and Thiel, V., 2013. Dipeptidyl peptidase 4 is a functional receptor for the emerging human coronavirus-EMC. Nature495, 251-254. https://doi.org/10.1038/nature12005
- Rolta, R., Kumar, V., Sourirajan, A., Upadhyay, N.K. and Dev, K., 2020. Bioassay guided fractionation of rhizome extract of Rheum emodi wall as bio-availability enhancer of antibiotics against bacterial and fungal pathogens. Journal of Ethnopharmacology 257, 112867. https://doi.org/10.1016/j.jep.2020.112867
- Rothe, C., Schunk, M., Sothmann, P., Bretzel, G., Froeschl, G., Wallrauch, C., Zimmer, T., Thiel, V., Janke, C., Guggemos, W., Seilmaier, M., 2020. Transmission of 2019-nCoV infection from an asymptomatic contact in Germany. New England Journal of Medicine 10, 970-971. https://doi.org/1056/NEJMc2001468
- Rustaiyan, A., Masoudi, S., Monfared, A., Kamalinejad, M., Lajevardi, T., Sedaghat, S., Yari, M., 2000. Volatile constituents of three Thymus species grown wild in Iran. Planta Medica 66, 197-8. https://doi.org/1055/s-0029-1243136
- Schwarz, S., Wang, K., Yu, W., Sun, B., Schwarz, W., 2011. Emodin inhibits current through SARS-associated coronavirus 3a protein. AntiviralResearch 90, 64-9. https://doi.org/10.1016/j.antiviral.2011.02.008
- Sohrabi, C., Alsafi, Z., O’Neill, N., Khan, M., Kerwan, A., Al-Jabir, A., Iosifidis, C. and Agha, R., 2020. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). International Journalof Surgery 76, 71-76. https://doi.org/10.1016/j.ijsu.2020.02.034
- Trott, O. and Olson, A.J., 2010. AutoDock Vina: improving the speed and accuracy of docking with a new scoring function, efficient optimization, and multithreading. Journalof Computational Chemistry 31, 455-61. https://doi.org/10.1002/jcc.21334
- Tu, Y., 2011. The discovery of artemisinin (qinghaosu) and gifts from Chinese medicine. Nature Medicine 17, 1217-20. https://doi.org/10.1038/nm.2471
- Walls, A.C., Park, Y.J., Tortorici, M.A., Wall, A., 2020, Seattle Structural Genomics Center for Infectious Disease (SSGCID).
- Wang, K., Tang, D., Wang, M., Lu, J., Yu, H., Liu, J., Qian, B., Gong, Z., Wang, X., Chen, J., Gu, M., 2009. MER3 is required for normal meiotic crossover formation, but not for presynaptic alignment in rice. Journalof Cell Science 122, 2055-63. https://doi.org/1242/jcs.049080
- Wang, Q., Wong, G., Lu, G., Yan, J. and Gao, G.F., 2016. MERS-CoV spike protein: Targets for vaccines and therapeutics. Antiviral Research 133, 165-177. https://doi.org/10.1016/j.antiviral.2016.07.015.
- Wong, S.K., Li, W., Moore, M.J., Choe, H., Farzan, M.A., 2004. 193-amino acid fragment of the SARS coronavirus S protein efficiently binds angiotensin-converting enzyme 2. International Journal ofBiological and Chemical Sciences 279, 3197-201.
- Xiao, X., Chakraborti, S., Dimitrov, A.S., Gramatikoff, K., Dimitrov, D.S., 2003. The SARS-CoV S glycoprotein: expression and functional characterization. Biochemicaland Biophysical Research Communications 312, 1159-64. https://doi.org/10.1016/j.bbrc.2003.11.054
- Yang, Z.Y., Huang, Y., Ganesh, L., Leung, K., Kong, W.P., Schwartz, O., Subbarao, K., Nabel, G.J., 2004. pH-dependent entry of severe acute respiratory syndrome coronavirus is mediated by the spike glycoprotein and enhanced by dendritic cell transfer through DC-SIGN. Journal of Virology 78, 5642-50. https://doi.org/10.1128/JVI.78.11.5642-5650.2004
- Zaki, A.M., Van, B.S., Bestebroer, T.M., Osterhaus, A.D., Fouchier, R.A., 2012. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. New England Journal of Medicine 367, 1814-20.
- Zhou, Y., Jiang, S. and Du, L., 2018. Prospects for a MERS-CoV spike vaccine. Expert Reviewof Vaccines17, 677-686. https://doi.org/10.1080/14760584.2018.1506702
- Zhu, N., Zhang, D., Wang, W., Li, X., Yang, B., Song, J., Zhao, X., Huang, B., Shi, W., Lu, R., Niu, P. 2020. A novel coronavirus from patients with pneumonia in China, 2019. New England Journal of Medicine. https://doi.org/1056/NEJMoa2001017
- Zhu, Y.Y., Yu, G., Wang, Y.Y., Xu, J.H., Xu, F.Z., Fu, H., Zhao, Y.H., Wu, J., 2019. Antiviral Activity and Molecular Docking of Active Constituents from the Root of Aconitum carmichaelii. Chemistryof Natural Compounds 55, 189-93. https://doi.org/10.1007/s10600-019-02651-5
{kind=link}