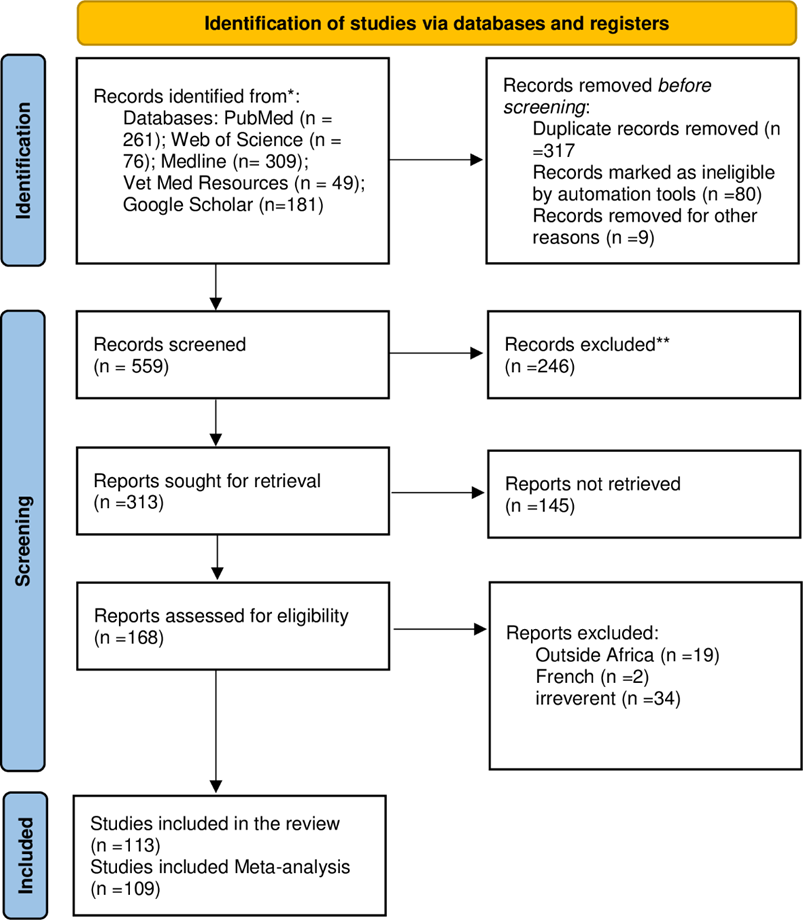
This review sought to evaluate the effectiveness of the interventions for the control of FMD and expound on its epidemiology in Africa. A total of 876 articles were obtained from five search engines with Medline followed by PubMed, and after screening 168 articles met the inclusion criteria. Out of these, 113 articles were eligible for this study, 4 articles were used for the effectiveness of interventions, and 109 articles were used for the meta-analysis. The articles were got from 20 out of 54 African countries: the highest number came from Ethiopia, Nigeria, Cameroon, Uganda, and 16 other countries in descending order. The East African region had the highest number of articles, followed by Western, Northern, Southern, and Central Africa. The animal species that were studied were cattle, goats, sheep, buffaloes, pigs, wildlife, and camels in descending order. The different diagnostic tests that were used to test for FMD in the studies were: ELISA, PCR, Several tests, and BTVIA in descending order. The FMD virus serotype SAT2 was a widely distributed serotype followed by Serotype O, Serotype A, serotype SAT1, and Serotype SAT3. Most articles reported cross-sectional study design, Field investigation, longitudinal study, retrospective, serological, and survey.
The overall estimated pooled seroprevalence of FMD in Africa was 16%. The subgroup analysis was performed at regions, and showed that the estimated pooled seroprevalence for the disease was highest in Central Africa followed by Northern, Western, Eastern, and least Southern Africa. The subgroup analysis that was performed at the species level gave the estimated pooled seroprevalences highest in the buffaloes followed by goats, sheep, cattle, pigs, and least in wildlife. The heterogeneity was extremely high at 100% (I2100%), and the LFK index of 4.83 indicated major asymmetry. The major interventions for control of FMD in Africa were vaccination and quarantine.
The finding of more articles in these search engines especially PubMed is in line with (19) who found out that the PubMed search engine is accessed for free, offers optimal update frequency, has online early articles, it’s an optimal tool for biomedical electronic search and is important resource technocrats and researchers.
The limited number of studies from countries that were got could have had an effect on the findings of the study. In countries where the disease was absent meant no published articles. It is also possible that FMD is not a priority disease in some countries. In some countries, FMD outbreaks could be limited to some locations/foci and easily contained. The capacity to diagnose FMD is limited or inadequate in some countries, this could be translated into fewer studies published from the country. The inadequate capacity to diagnose FMD is in line with the findings of (10, 20).
The few articles from individual countries could be linked to the issue of concealing FMD with fear of trade-related consequences this agrees with the finding (21) that countries conceal disease for the fear of trade and travel barriers. (22) that farmers were concealing the epidemics. This translates to the country level. It is also possible that the limited research on FMD in some countries led to few studies published on FMD in the countries.
The East African region had the highest number of articles that contributed to the review. This could have been a reflection of the ongoing work and research on the disease in those countries. It was also eminent that countries were at different levels of the Progressive Control Pathway for the control of FMD (PCP-FMD). The disease is taking a long time to be eliminated due to the fact that the different countries are at different levels of PCP-FMD in relation to compliance levels and the constraints that are faced. The review finding is in line with the finding by(20) found that 92.3% of East African countries were below stage 3 of the PCP-FMD.(23) found out that the PCP-FMD needs to be in alignment with the pathway outcomes of the surveillance system components.
The Southern African Territories (SAT) serotypes can be traced back to the mid-fifteenth to mid-sixteenth century (24). The FMDV serotype SAT2 was the most widely distributed in Africa. This is in agreement with the findings of Bastos et al., (2003) who found out that SAT 2 is the serotype most often associated with outbreaks of foot-and-mouth disease (FMD) in livestock in Africa. This could also be due to the fact that FMD serotype SAT2 has been in existence for a long time this is in agreement with the finding of (25). The history of FMD in Africa is traced back to the 1780s (26).
In the review, FMD was more published by cross-sectional study designs. This is in line with the study by(27) and(28) that cross-sectional studies are relatively quick and inexpensive to conduct, do not follow individuals up over time, they have no ethical difficulties, data on all variables are only collected at one-time point, multiple outcomes and exposures can be studied, they are easy for generating hypotheses, and many findings can be used to create an in-depth research study.
The disease FMD is endemic in most African countries (29), with the exception of a few southern African countries (Botswana, Namibia, and South Africa) where it has been controlled and declared free. This possess a danger of hot spot for those countries where the disease has been eliminated and controlled. The epidemiology of FMD in Africa is multifaceted due to the presence of many serotypes where six of the seven FMD V serotypes are present in Africa except Asia 1 (1); antigenic variation; animal movement; wildlife (1, 29). Studies from Southern Africa have shown that wildlife plays a role in the epidemiology of the disease (29–31) but the mechanism is not fully understood (29). (32) highlighted that animal movement, trade, animal numbers, mixing of animal herds and species, contact of domestic and wildlife, and climatic factors are the contributing risk factors.
The high prevalence of FMD in Africa is due to contact of livestock with wildlife especially African Buffaloes, multi serotypes, animal movement, trade, animal numbers, mixing of animals, climatic factors, and poor control measures where the quality of the vaccines is not monitored renders the vaccine ineffective. The more animal species included in the studies could be due to the priority of those animals in the different countries. These are for trade, and sources of people’s livelihood. There is a tendency to prioritize the importance of certain animal species as compared to others. The pastoral communities tend to value cattle over other species. The livestock-keeping communities have a practice of keeping and mixing different animal species and age groups together. Other practice discriminative application of the control measures. The different animals have varying susceptibilities to the diseases. The presence of wild animals has been shown to play a role in the transmission and spread of the disease hence its epidemiology. Research is being conducted on different animal species such as camels and other wildlife species other than the classical cloven susceptible animals to FMD. Requires revision and proper documentation with references.
The highest pooled seroprevalence of FMD was highest in Central African countries and least in Southern African countries. This can be explained by the finding of(14) who found out that there was a long-distance spread of the FMDV serotypes within the North, West, Central, and East regions of Africa. In the different African regions, the production of animal systems for the search for water, pastures, and trade were present except in the Southern African countries (14). In Southern African countries, the African buffaloes are extensively studied(14) and the disease is largely controlled by fencing (33), but the buffaloes are more distributed in other regions and there is limited control of the disease. It is from Southern African countries that are able to export animal products to European countries.
The highest pooled seroprevalence of FMD in buffaloes was high compared to other animals. This was in line with the findings of(34) that the African buffaloes are systemically affected by the FMD virus. Studies by(35) showed that the FMD viruses persisted in the African buffalo, which serves as their wildlife reservoir (29). However, the FMD viral persistence in the buffaloes was not unlikely (36, 37), and the transmission mechanism is not known (29). The study by Duchatel et al., (2023) showed impala population act as an intermediate host between the cattle and buffalo populations and plays a role in the circulation of the viruses. The study by(38) revealed that geographic features, such as rivers, influence the circulation of FMDV in buffalo.
The animals that were most studied were cattle (72%) other included goats, sheep, buffaloes, pigs, wildlife, and camels. The cattle were the most studied animal species because of their social-cultural and economic role; and source of livelihood. The lower pooled seroprevalence in the goats and sheep is in line with the findings of Wolf et al (2020) that clinical signs of the disease do not manifest well in these species.
The diagnostic technique that was used in the study of FMD was mostly by antigen ELISA. This agrees with the findings of(39) who found that the most serological technique used to diagnose FMD, is by antigen ELISA. A few studies employed PCR techniques and this is in agreement with the findings of(40) that in endemic settings the PCR field techniques are used because of their simplicity, sensitivity, and rapid detection.
The interventions were by vaccination and quarantine or restricted animal movement. The effectiveness was 75% partial, and 25% not effective. The findings were attributed to many animals that go unvaccinated during the outbreaks, the vaccines being expensive, and the long period of time it takes to respond to the outbreak (41). The presence of wildlife such as African buffaloes which act as reservoirs for FMDV like SATs(41, 42) hindered the efficiency of the control measures. Further to that, vaccines are insufficient to provide herd immunity to control the disease at the population level (43). The available vaccines in most countries are able to control the outbreaks caused by the same serotype found in the vaccines but was not able to prevent the infection and eliminate the disease (44). There is a need to improve the quality, incorporate more serotypes into the vaccine, maintenance of the cold chain, vaccine research and studies, awareness creation and improvement of the vaccination services. That is how the vaccines will be able to serve the purpose as suggested by (45).
{kind=link}