In this study, we investigated for the first time the clinical effectiveness of AIP for predicting thrombotic events in AAV patients. We demonstrated that AAV patients with AIP ≥ 0.11 exhibited the significantly reduced cumulative CVA-free survival rate compared to those with AIP < 0.11 over 20.2 months. Our findings indicate that AIP at diagnosis is an independent predictor for CVA during follow-up among various conventional risk factor for serious thromboses as well as AAV-specific indices and acute phase reactants.
We compared AIP in AAV patients with control subjects who had no serious medical conditions including malignancies, fatal infectious disease, and chronic inflammatory diseases, particularly vasculitis. We found that AIP of AAV patients was significantly elevated compared to that of controls (0.01 vs. –0.12, P < 0.001). In previous studies, AIP of non-obese controls was found to be –0.04 ± 0.28 [17],, that of post-menopausal women controls without CVD was assessed as 0.10 ± 0.27 [9] and that of non-systemic lupus erythematosus controls was reported to be 0.24 ± 0.21 [18].. Meanwhile, AIP in patients the end-stage renal disease was reported to be 0.47 (interquartile range 0.26–0.66). Moreover, AIP in patients with ankylosing spondylitis receiving anti-tumour necrosis factor-α inhibitor and that in those with AS not receiving were reported to be –0.085 ± 0.378 and –0.119 ± 0.343, respectively. Therefore, the range of AIP in patients and controls appear to vary based on ethnicity, geographical factors and medical conditions. For this reason, we believe that it was clinically significant to determine AIP of Korean patients with AAV as 0.01 for the first time.
In the cross-sectional comparative analysis of variables at diagnosis between patients with AIP < 0.11 and those with AIP ≥ 0.11, only serum total protein levels showed a statistically significant difference between the two groups. However, this difference was not clinically significant because there was no correlation between AIP and serum total protein (r = –0.072, P = 0.356). Furthermore, reduced serum total protein level has not been reported to directly associated with thrombotic events except nephrotic syndrome.
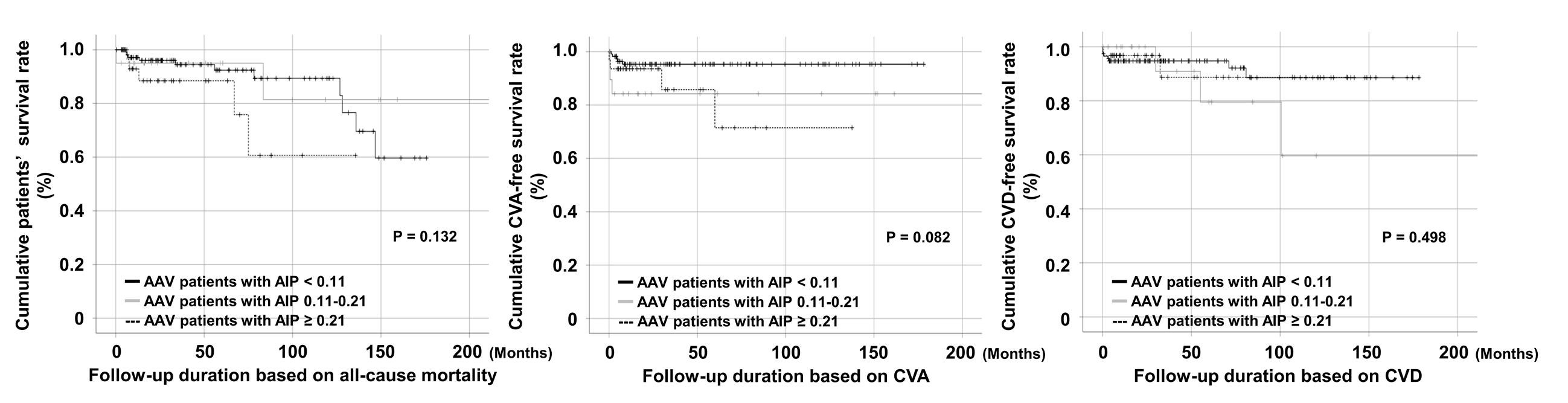
In this study, we chose AIP of 0.11 as the cut-off for predicting CVA for three reasons. First, we investigated the cumulative poor outcome-free survival rate according to low (< 0.11), intermediate (0.11–0.21) and high risk (≥ 0.21) based on AIP using the Kaplan-Meier survival analysis. In terms of death, the cumulative patients’ survival rate in AAV patients with AIP < 0.11 was lower than that in those with AIP of 0.11–0.21 and in terms of CVD, the cumulative CVD-free survival rate for patients with AIP 0.11–0.21 was the lowest among three groups. However, in terms of CVA, although statistical significance was not reached, it can be apparently seen that the frequency of CVA increased as the risk of thromboses based on AIP increases (Supplementary Fig. 2)..
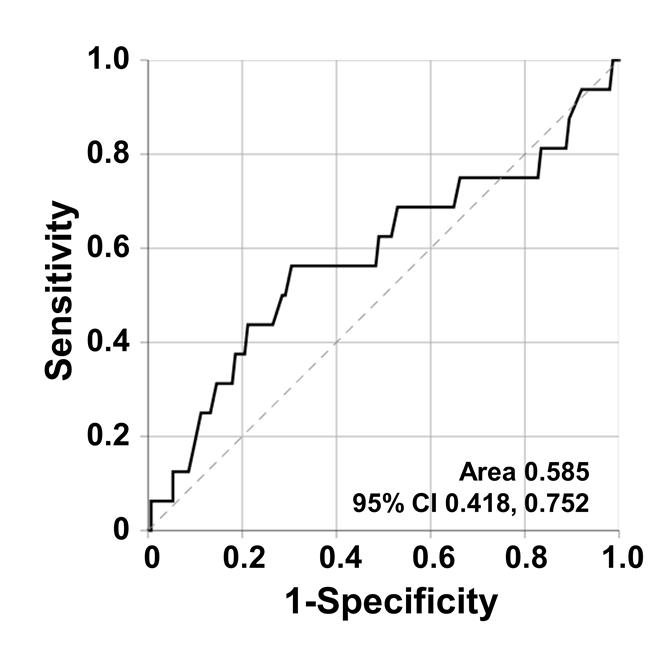
Second, if an AAV-specific cut-off of AIP to predict CVA in AAV patients was defined, we could determine the high-risk group and apply close monitoring for CVA occurrence during follow-up by shortening the interval duration or recommending a regular check-up for CVA. For this reason, the AAV-specific cut-off of AIP for CVA occurrence was extrapolated by calculating the receiver operator characteristic (ROC) curve and selecting the maximised sum of sensitivity and specificity. However, no significant cut-off was obtained (area 0.585, 95% CI 0.418, 0.752) owing to no consideration of the follow-up duration in this method (Supplementary Fig. 3).. Third, when AAV patients were divided into groups based on AIP of 0.21, only 32 of 167 patients were assigned to the AIP ≥ 0.21 group. In this case, the specificity of thrombosis is high, but it is not suitable for screening or monitoring because of the low sensitivity. Therefore, we suggest that physicians should inform all AAV patients with AIP ≥ 0.11 that they are of high risk of CVA occurrence and actively recommend a regular check-up for CVA.
Of the medications administered during follow-up, both cyclophosphamide (63.5% vs. 47.0%) and rituximab (26.9% vs. 13.0%) were administered more commonly to AAV patients with AIP ≥ 0.11 than to those with AIP < 0.11 %. Based on the latest recommendations for the management of AAV proposed by the European League Against Rheumatism and the European Renal Association-European Dialysis and Transplant Association, either cyclophosphamide or rituximab together with glucocorticoid should be applied to newly diagnosed patients with life-threatening AAV [19].. Therefore, it can be reasonably speculated that the sum of the inflammatory burden in AAV patients with AIP ≥ 0.11 might be significantly higher than that of patients with AIP < 0.11 during follow-up, leading to an increased risk for CVA. Furthermore, it should be noted that the sum of the inflammatory burden could not simply be estimated by BVAS at diagnosis and rather, it might be reflected by the frequency of the exposure to cyclophosphamide and rituximab.
Of the conventional risk factors for thrombosis, AAV-specific indices, acute phase reactants and AIP [12–14, 20, 21],, CVA occurrence was significantly associated with both AIP ≥ 0.11 and CRP in the univariable Cox hazards analysis and with only AIP ≥ 0.11 in the multivariable Cox model hazards analysis. BVAS at diagnosis tended to be associated with CVA but it did not get to statistical significance (P = 0.066). Also, it was beyond expectation that FFS at diagnosis, which is a prognostic factor in AAV patients, was not associated with CVA occurrence. Therefore, we concluded that AIP ≥ 0.11 at diagnosis can be used as an independent predictor of CVA during follow-up in AAV patients.
However, we expected the synergistic effect of AIP ≥ 0.11 with hypertension and diabetes mellitus which are strong conventional risk factors for thrombosis [21],, and, they were not associated with CVA during the follow-up period per Cox hazards model analysis. Moreover, smoking is well known to be closely related to CVA [22],, however, it was not associated with CVA in this study. We assumed that the influence of smoking on CVA occurrence was underestimated owing to the small number of former smokers (a total six patients).
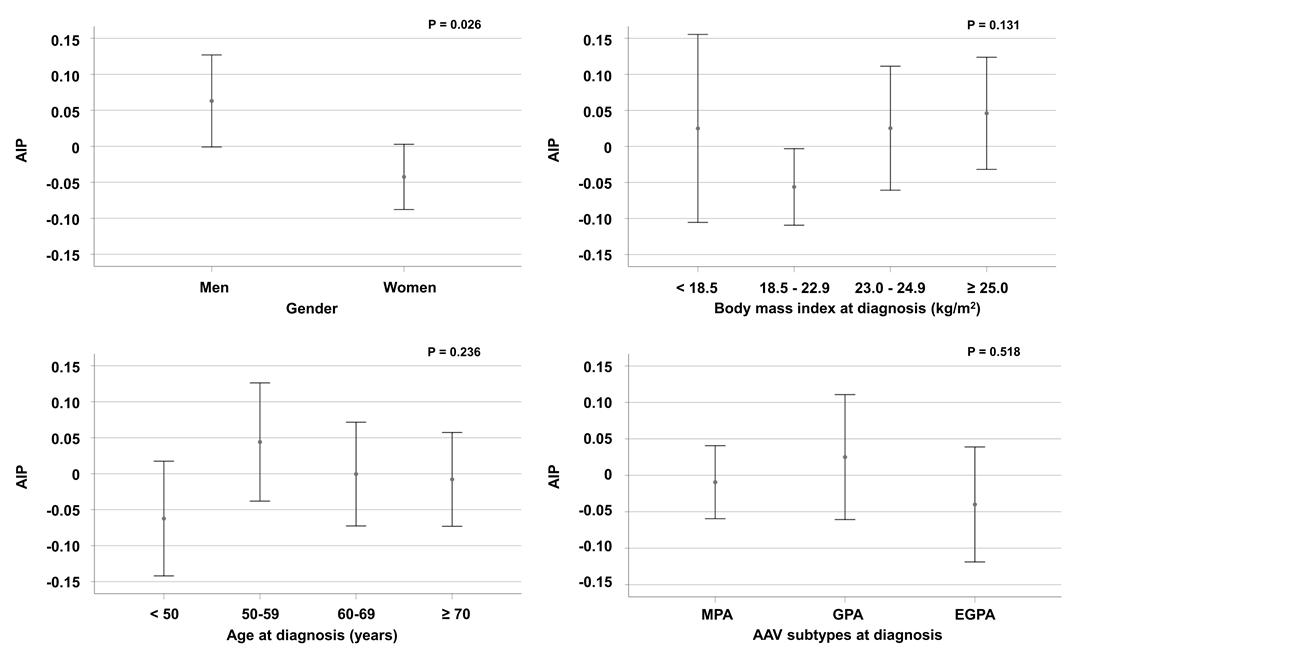
A previous study suggested the major factors to increase AIP such as male gender, obesity and increased age [23].. Similarly, male patients with AAV exhibited significantly elevated AIP compared to female ones (Supplementary Fig. 1),, however; AIP was not affected by obesity based on body mass index and age in this study. With regard to body mass index, there was a tendency of AIP to decrease along with decreased body mass index-range among normal weighed, overweighted and obese patients. However, it was rebounded up in underweighted patient with AAV. We could not explain exactly about this phenomenon, but we tried to understand this pattern by the U-shape pattern of cholesterol based on body mass index [24].. With regard to age, age was positively correlated with body mass index with a statistical significance (r = 0.213, P = 0.006). however, AIP based on age apparently showed the opposite pattern from AIP based on body mass index. With these results, it is believed that AIP in vasculitis patients exhibits a different movement from AIP in the general population. AAV subtype did not seem to contribute to AIP levels.
This study has merit in that we determined that AIP at diagnosis is an independent predictor for CVA during follow-up in a considerable number of patients with AAV for the first time. However, our study has several issues such as a retrospective study design, a monocentric study and not a large number of AAV patients included. in addition, since AIP does not include other subtypes of cholesterols, such as LDL-cholesterol, total cholesterol and non-LDL cholesterol, we could not clarify the relationship between these cholesterol subtypes and CVA occurrence through AIP in this study. We expect that future prospective studies with a larger number of AAV patients and plenty of laboratory data related to thrombosis will provide better and dynamic information of AIP in predicting thrombotic events as serious complications of AAV.
{kind=link}
{kind=link}
{kind=link}