In line with the knowledge that patients with CIDs are at increased risk of developing CVDs, several studies have demonstrated that the risk of CVDs is heightened in AAV patients. A long-term population-based study revealed that the risk of CVD and CVA in AAV patients were 3- and 8-fold higher than those in matched subjects [22]. In addition, a retrospective study that was performed in the United Kingdom has shown that AAV patients have high incidence of arterial and venous thrombosis [23]. Moreover a meta-analysis by Houben et al. demonstrated that the risk of developing cardiovascular events was higher in AAV patients compared to the general population [24]. Therefore, it is clinically important to uncover predictors that could help estimate the development of CVDs in AAV patients, as this could be a potentially life-threatening event.
To the best of our knowledge, this is the first study that evaluated the clinical effectiveness of using AIP to predict CVA and CVD in AAV patients. Consistent with what was initially expected, the observations from this study demonstrated that AAV patients had significantly higher AIP compared to healthy controls (0.01 vs. -0.12, P < 0.001). Moreover, AAV patients with AIP ≥ 0.11 on diagnosis exhibited significantly higher disease activity at baseline, and the occurrence of CVA events during the follow-up was more frequent compared to those with AIP < 0.11. In addition, Cox hazards analysis revealed that AIP ≥ 0.11 at diagnosis is an independent predictor for CVA during follow-up, even when various conventional risk factors for CVDs, ANCA types, AAV-specific indices, and acute phase reactants were taken into consideration [17, 18, 25-28]. On the basis of the results of this study, it could be suggested that the occurrence of CVA should be actively monitored in AAV patients, especially in those with AIP ≥ 0.11, when the initial diagnosis is established.
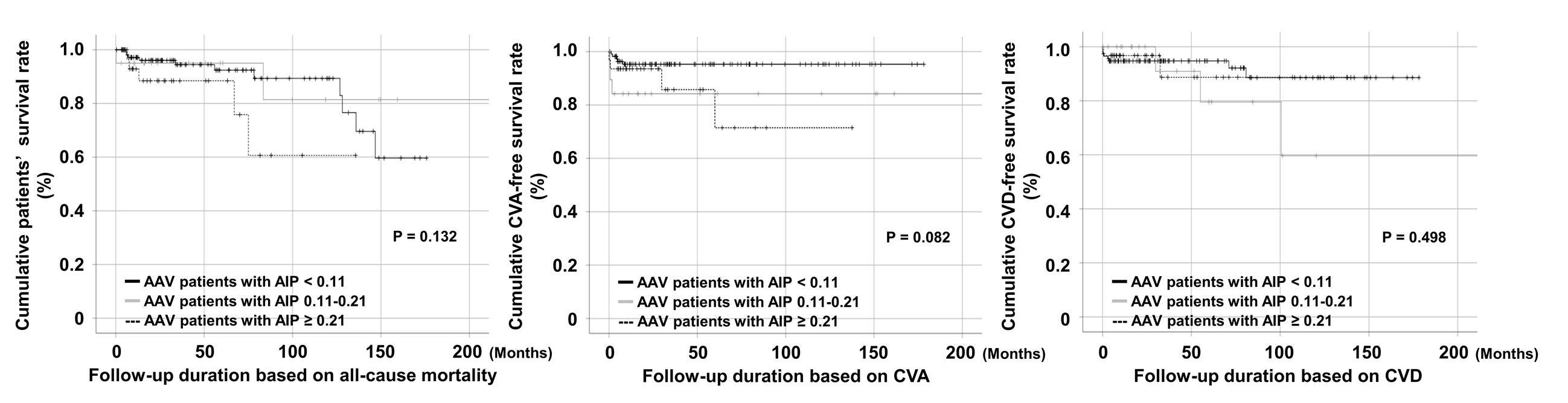
In the present study, the cut-off value of AIP ≥ 0.11 was adopted to predict de novo CVA events in AAV patients; this was done since the number of patients with AIP 0.11-0.21 (N=20) and AIP > 0.21 was small (N=32) and since the events of CVA and CAD were observed in a relatively small number of patients. Therefore, categorizing patients into the three different groups of AIP < 0.11, AIP 0.11-0.21, and AIP > 0.21 could result in a false negative result owing to a low statistical power. Indeed, when the clinical outcomes were compared by dividing the patients into three groups, the patients with AIP < 0.11 were less likely to experience CVA compared to those with AIP 0.11-0.21 and AIP > 0.21, even though the risk of developing CVA was not directly incremental (Additional File 1).
Previous studies have demonstrated a variable range of AIPs, and the variations could arise because of differences in ethnicity, gender, geographical factors, and the medical conditions investigated. A study by Zhu et al. has shown that the mean AIP values in Chinese people with and without obesity were 0.13 and -0.04 [29]. On the other hand, Wu et al. identified the mean value of AIP in postmenopausal women with CAD and without CAD as 0.20 and 0.10, respectively; furthermore, a study that estimated AIP in subjects undergoing chronic dialysis reported median values of AIP as 0.47 [13, 30]. Notably, several studies have been performed to evaluate AIP levels in CIDs, and a study that compared AIP levels in patients with SLE and controls showed that SLE patients had significantly higher AIP levels than controls, which is consistent with the result of this study [31]. Moreover, it was also described that AIP could be a predictor of subclinical atherosclerosis, particularly carotid artery intima-media thickness, in subjects with SLE, Behçet disease, and ankylosing spondylitis, emphasizing that subjects with higher AIP could be more vulnerable to CVA among patients with CIDs [31-33]. However, as most of the studies that were performed in patients with CIDs did not directly evaluate the incidence of CVAs, additional research is necessary to determine the relationship between AIP and CVAs in CIDs.
Besides AIP, previous data have proposed that higher cholesterol levels, such as TC, LDL-cholesterol, and TG could be used to predict the incidence of CVDs, even though inconsistent results were obtained across studies [34-37]. Accordingly, when the predictive value of these different laboratory measures was investigated, AIP ≥ 0.11 and HDL-cholesterol were found to be significantly associated with the incidence of CVA. However, given that AIP and HDL-cholesterol are closely associated because AIP level also includes the level of HDL-cholesterol in its calculation, further research is necessary to identify which is the most appropriate measure in estimating CVDs in AAV.
It has been acknowledged that higher disease activity is generally associated with increased risk of CVDs in patients with CIDs [38, 39]. Accordingly, on comparing the baseline characteristics of patients with AIP ≥ 0.11 and AIP < 0.11, it was found that the difference of BVAS between the groups was significant (P = 0.041). Furthermore, in regard to the medications administered during follow-up, both cyclophosphamide (63.5% vs. 47.0%, P = 0.048) and rituximab (26.9% vs. 13.0%, P = 0.028) were administered more commonly to AAV patients with AIP ≥ 0.11 than to those with AIP < 0.11 (Additional File 2). Based on the recommendations for the management of AAV, either cyclophosphamide or rituximab together with glucocorticoid should be given to AAV patients with life-threatening disease [40]. Taken together, it can be speculated that the inflammatory burden in AAV patients with AIP ≥ 0.11 is significantly higher than that of patients with AIP < 0.11 during follow-up, leading to an increased risk for CVA. In particular, it should be noted that the sum of the inflammatory burdens could not be simply estimated through BVAS, which consists of multiple measures that may not properly indicate the dynamic changes of vascular inflammation [41].
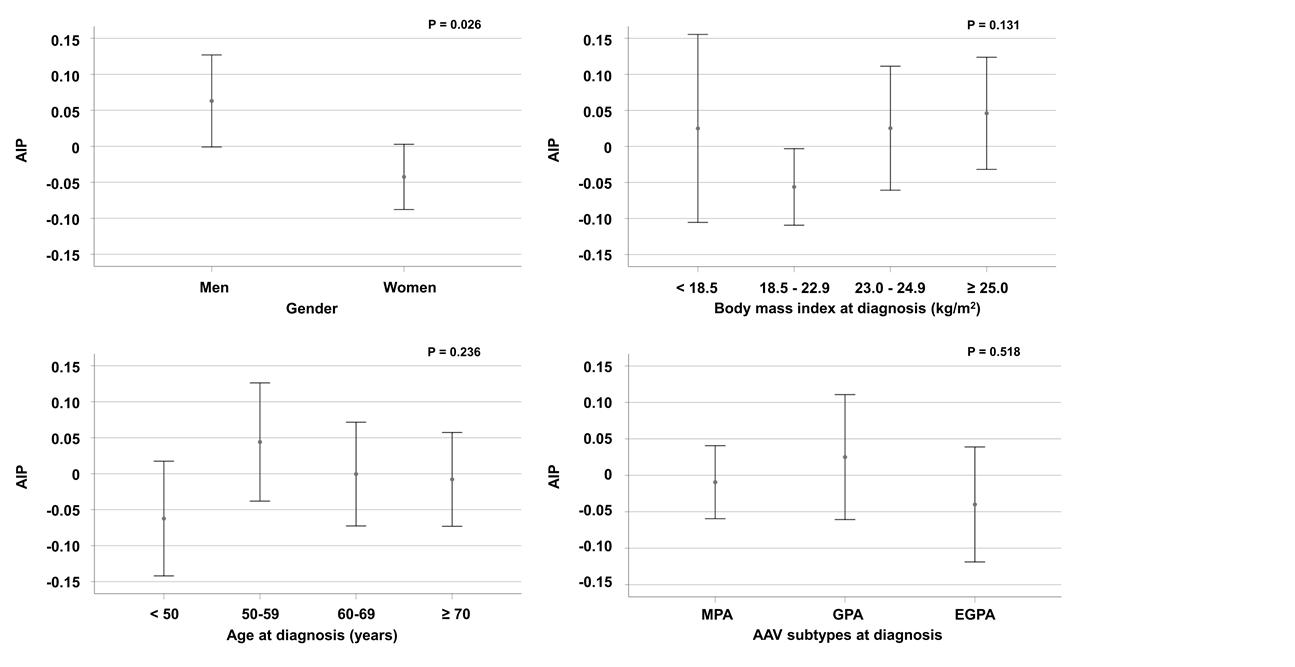
A previous study suggested that the major factors influencing AIP were gender, obesity, and older age [42]. Accordingly, in this study, a subgroup analysis was performed to determine whether these factors affected the level of AIP. Of note, even though it was also revealed that male AAV patients exhibited significantly elevated AIP levels compared with females, which is similar to the previous studies, AIP was not found to differ based on BMI, age, and disease subtypes in the present study. Even though this discrepancy could be explained by the difference in the study population and the study design, it seems apparent that the impact of AIP in health and diseases could be variable and should be better investigated.
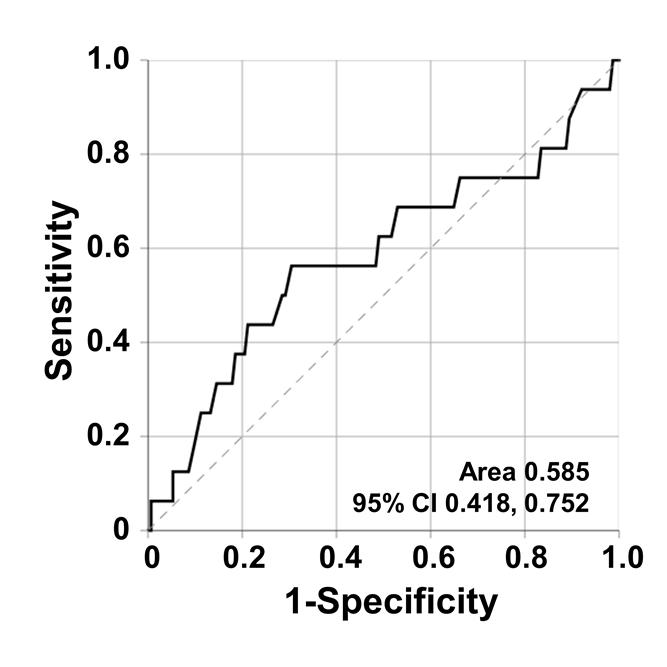
The most important strength of the present study was that it demonstrated, for the first time, that AIP at diagnosis is an independent predictor for CVA. However, several issues should be considered as limitations. First, the study was performed retrospectively and the clinical outcomes of the patients were identified by reviewing the hospital’s medical records. In addition, the optimal cut-off value of AIP in predicting CVA could not be defined by this study. Second, because only laboratory data at initial diagnosis was used to calculate AIP, it is unclear whether dynamic changes in AIP levels might be more relevant to the risk of CVDs. Third, the precise mechanism of how AIP is associated with increased CVA events could not be elucidated. Future prospective studies with a larger number of patients will help verify the results of this study and provide more information regarding the potential of AIP in predicting CVA in AAV.
{kind=link}
{kind=link}
{kind=link}