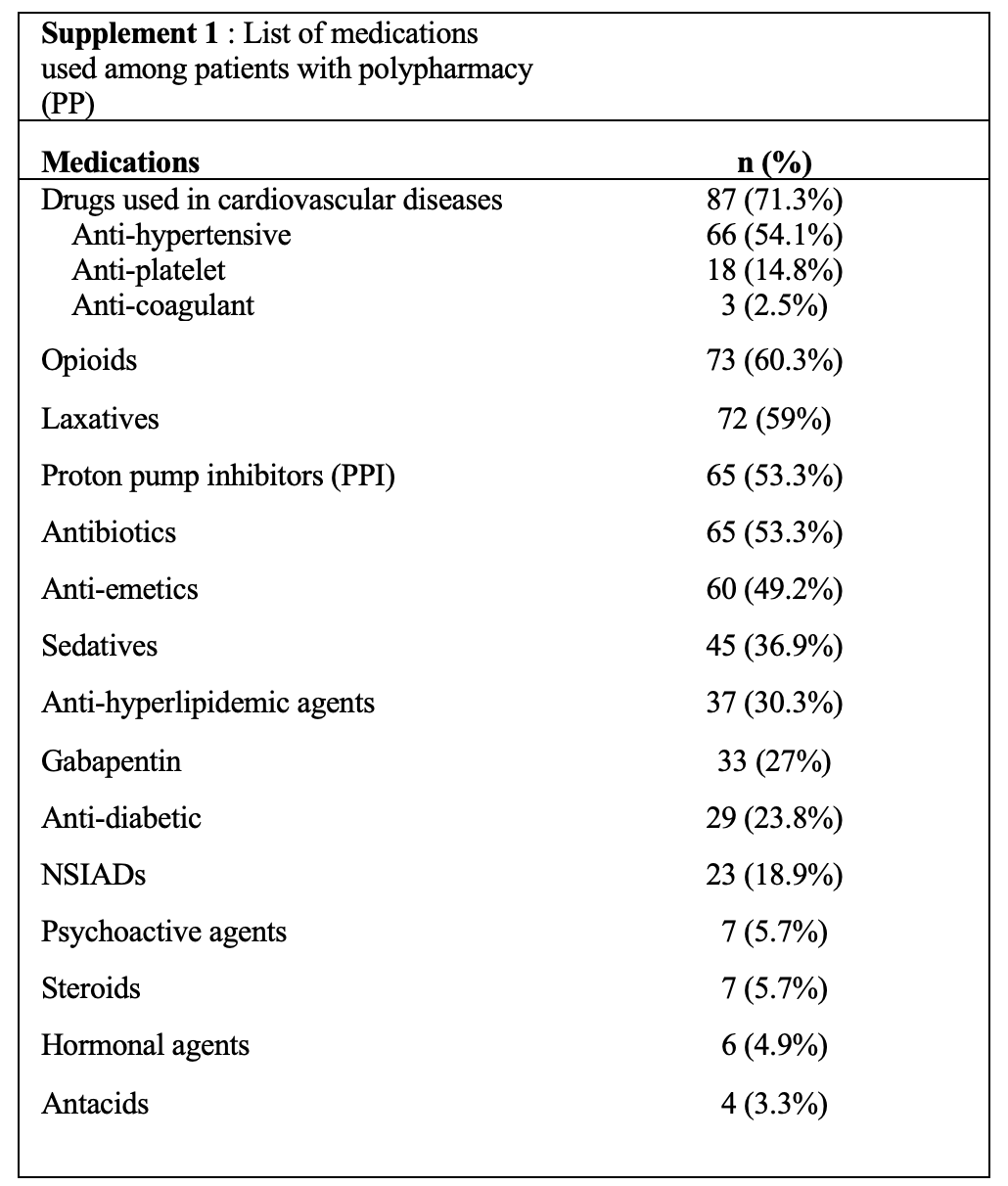
Relying on the definition of PP, from 11–96% of the elderly cancer patients were exposed to excessive medications.5 This study practically defined PP in numerical term; however, duration of continuing medications would have been more logical to be determined, if long-term association with adverse events were the outcome of interest. The prevalence of PP and hyper-PP of 67.8% and 20%, respectively were not doubtfully outstanding compared with those reported by studies conducted among Asian populations. Khaledi, et al reported the strikingly 88% frequency among cancer patients unselected by age group.18 Yeoh, et al. reported 58% of the elderly cancer patients in Singapore had PP.8 Takemoto, et al. showed that 23.1% and 32.6% of the elderly Japanese cancer patients in curative and palliative settings, respectively had PP.9 The most recent data from the Western countries was reported by Ramsdale, et al. She and her colleagues collected data from a randomized study enrolling patients aged ≥ 70 years with advanced cancer conducted at University of Rochester Cancer Center. Among 718 patients (mean age 77.6 years), PP (≥ 5 medications) and hyper-PP (≥ 10 medications) were identified in 61.3% and 14.5%, respectively.19 The investigators also found that PP and hyper-PP were both associated with existing co-morbidities; however, age (as differentiated between less than and more than 70 years old), sex, staging, type and cancer stage were not. As determined by Charlson co-morbidity index (CCI), the more serious co-morbidities a patient had, the higher number of concomitant medications were prescribed. The association between PP and co-morbidity was still existed when the sensitivity analysis was performed by exclusion of opioid analgesics, laxatives and anti-emetics. Turner, et al. evaluated the prevalence and factors associated with PP in the elderly Australian cancer patients and demonstrated that when adjusting for age, sex, instrumental activities of daily living (IADLs), Karnofsky Performance Scale (KPS), physical function (using SF-36), pain (using 10-point visual analogue scale, VAS), exhaustion (using CES-D) and distress (using 10-point VAS), polypharmacy was remained independently associated with higher CCI scores.15 This study excluded the elderly patients who had not received active anti-cancer management mainly due to an oncologist’s discretion. Presumably, most of them were either frail or unfitted for aggressive cancer care. Therefore, the investigators concluded that CCI was still independently associated with PP and hyper-PP among elderly cancer patients fitted for aggressive cancer management. The study by Yeoh, et al. (still presented in abstract) also demonstrated the same co-relation.8 Cardiovascular agents (including anti-hypertensive, anti-platelets, anticoagulants and miscellaneous), proton-pump inhibitors and antibiotics were the top pharmacological classes most frequently prescribed in this cancer patients’ cohort. In accordance with a recent study in the USA, Ramsdale, et al. reported that cardiovascular drugs were the most prevalent in the elderly cancer patients.20 Nightingale, et al. also mentioned that among ambulatory elderly cancer cares, the prevalence of PP was high and cardiovascular drugs, anti-lipidemic drugs and drugs modulating GI system were the most prevalent ones.7 Earlier studies reporting the prevalence in Denmark showed that analgesics, acid-suppressing drugs, and antibiotics were most frequently prescribed up to six months preceding cancer diagnosis.6Among studies investigating the consequences of PP in the broader populations, Guthrie, et al. showed that cardiovascular drugs, and drugs affecting the CNS and GI systems were the most frequent prescribed in a Scottish community and they also speculated that not only the prevalence of PP was rising, but the prescribed drug combinations would be more complicated and potentially harmful.20 A warning signal from a South Korean study conducted by Cho, et al. would represent the burden of PP in Asian countries. Cho and colleagues found that nearly half of the elderly South Korean patients had PP and the combinations of cardiovascular, anti-lipidemic and acid-suppressing drugs were most commonly prescribed.4 Based on these evidences, there has been the global trend towards more and more perplexed prescriptions of the drug classes affecting or modulating cardiovascular and nervous systems representing the burdens of non-communicable diseases (NCDs) in the ageing society emerging in many parts of the world.
As a result of the difficulty in determining serious true drug-to-anti-cancer treatment interactions, the investigators evaluated the association between PP/PIMs and unexpected hospitalizations instead. The investigators found that both corrected PP (excluding opioids, laxatives and anti-emetics) and hyper-PP, male gender and metastatic disease at cancer diagnosis were the independent factors associated with repeated unexpected hospitalizations. Interestingly, the causes of hospitalization were fundamentally related to infections, both associated with and un-associated with cancer-treatment-induced neutropenia. However, due to non-specific presentations among the elderly patients, altered consciousness presumptively diagnosed to have sepsis would rather be the manifestations of undesired side effects from drug interactions from excessive medications used. Due to the ever-changing numbers of prescribed medications and their exact duration of truly administered drugs, the investigators found inconclusive effect of PIMs to survival and hospitalizations. There were incoherent evidences demonstrating the detrimental effects of PP and PIMs among cancer patients. Sehgal et al. performed a retrospective analysis in a general patient population and found that the presence of concomitant PIMs and PP had a statistically significant tendency to increased hospital readmissions; nevertheless, PIMs alone was not significantly correlated.21 Maggiore et al. conducted a secondary analysis of a prospective study to determine the prevalence and the effect of PP and PIMs on chemotherapy-related adverse events (AEs) and revealed no meaningful association found between either PP or PIMs and AEs or hospitalization. They also further explored the consequence of taking one or more of the 6 high-risk pharmacologic classes of medications potentially related to serious AEs (i.e., anticoagulants, antiplatelet agents, opioids, insulin, oral hypoglycemics and antiarrhythmics) and again they found no specific pharmacologic class significantly associated with either outcome.22 Sganga, et al. carried out a prospective cohort study conducted in elderly patients (not cancer patients in particular) who had discharged from acute care hospitals to determine the rate of re-hospitalization and mortality within 1 year after discharge also demonstrated that multiple-drug uses (defined as more than 8 drugs a day) was at increased risk of re-hospitalization.13 A systemic review and meta-analysis by Mohamed MR et al. concluded that even though various definitions of PP, heterogeneities in terms of both study designs and populations, PP was associated with post-operative complications, chemotherapy toxicities and both physical and functional decline.10
Regarding the association between PP/PIMs and survival, there were scant evidences intended to determine the effect of PP/PIMs on survival in particular. The investigators demonstrated that more advanced age (≥ 70 years), primary pulmonary cancer, metastatic disease at cancer diagnosis, unexpected hospitalizations were the significant predictive factors of 1-year mortality. However, the investigators failed to demonstrate both PP and hyper-PP with the mortality. Elderly patients with primary pulmonary cancer and advanced stage at diagnosis were unquestionably vulnerable subgroups requiring properly tailoring cancer management. More extreme age and repeated hospitalizations were the factors to be elucidated. Even though cancer is the disease of ageing; however, age alone should not be the solitary factor of exclusion of ageing patients from active cancer treatment. Co-morbidities and ageing exist independently and the prevalence of co-morbid conditions climbs with increasing age.23 Numerous data have emphasized on assessing biological rather than chronological age in individual cancer patients. The comprehensive geriatric assessment (CGA) can provide extensive information of both functional and physiological age of an elderly person with cancer in particular. Several domains, including physical function, cognition, nutrition, comorbidities, psychological status, and social support are evaluated together. Although it consumes clinical visiting time, its results can guide a physician to choose proper management more systemically.24, 25 The multi-comorbidity was not the independent factor for survival in this elderly cancer patients’ cohort; however, a probability of the fact that some co-morbid conditions were more predictive than the others cannot be excluded. Provocatively, a real-world data reported by Karuturi et al. supported the drawback of PP/PIMs on mortality as the investigators’ results did. They analyzed a substantially large elderly cancer patients’ cohort including 1595 breast cancer patients and 1528 colorectal cancer patients from the SEER database. They demonstrated that among elderly breast cancer patients, 37.5% had 1 or more adverse outcomes (emergency room (ER) visit, hospitalization or death). PP, advanced stage, higher co-morbidity, and prior ER visits/hospitalizations were significantly associated with such adverse outcomes. PIMs (defined as using any drugs included in DAE list) was associated with an increased risk of death. In line with the elderly breast cancer cohort, 45% of the elderly colorectal cancer patients had at least 1 adverse outcome. Again PP, more older age, female sex, and higher comorbidity were the independent factors. Confusingly, baseline PIMs did not co-relate with time to any events of adverse outcomes.26 Whether PP and PIMs are associated with the mortality in the elderly cancer patients receiving aggressive oncological management is a subject to debate. The investigators noticed that secondary data from randomized clinical trials would not represent the realistic point of view because clinical trials usually recruit highly-selective participants compared to the real world practices do. Recent GAP70 + randomized trial demonstrated that applying the geriatric assessment intervention could ameliorate serious adverse events, falls and polypharmacy in elderly patients with advanced cancer patients receiving oncological treatment including chemotherapy.27 The investigators suggest that among such vulnerable patients, judicious and more vigilant prescriptions are advocated. Such strategy will lead to reduction in medical futility and avoidance of unexpected adverse events.
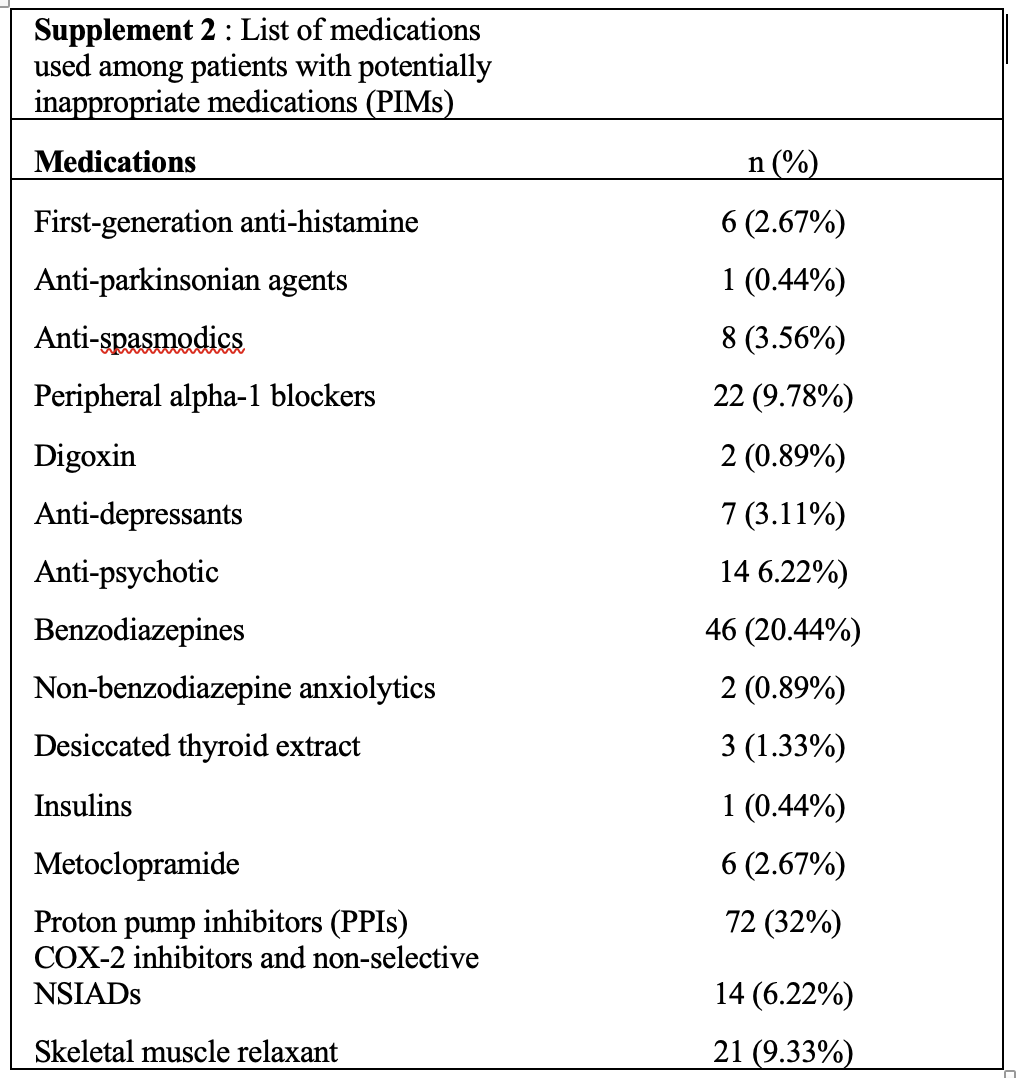
In conclusion, the investigators revealed the prevalence of PP among elderly cancer patients eligible for systemic cancer treatment was 67.8% and the prevalence of PIMs of 69.4% was also unacceptably high. The investigators speculated that the number of prescribed drugs depended on a pre-existing patient’s co-morbidity; therefore it would be possible to prescribe if physicians carefully determined the necessity. Extreme ageing cancer patients, primary pulmonary cancer, metastatic disease at diagnosis, and repeated unexpected hospitalizations were associated with short survival. Such vulnerable patients were among those who need comprehensive geriatric assessment (CGA) to determine the most proper cancer care. Moreover, cancer patients with extreme age, metastatic disease at diagnosis and hyper-PP had strong tendency towards more unexpected hospitalizations. A physician should be more vigilant in taking care and prescribing such patients who are more likely to succumb to serious adverse events.
Strengths
The investigators conducted a prospective cohort study in a real-world situation and followed up the participants long enough to determine the adverse outcomes.
Limitations
The investigators did not collect the data regarding socio-economic status and performance status. According to the latest evidences and systemic reviews, the socio-economic status was less clinical relevant to cancer treatment outcomes compared to other factors presented in this cohort study. Due to advances in cancer treatment and accessibility to the less toxic hormonal agents in some breast cancer patients and the epidermal growth factor receptor tyrosine kinase inhibitors in some lung cancer patients, patients with poorer performance status (ECOG PS 2) would gain benefits from active cancer treatment; therefore, the investigators recruited the participants solely based on an oncologist’s discretion. Moreover, this study determined PP in numerical basis only; however, duration of drug exposure would be a significant factor to elucidate the long-term association with adverse events.

{kind=link}
{kind=link}