This study is one of the few to compare changes in skeletal muscle mass with prognosis in patients with PPFE. This study highlights the importance of these two evaluation aspects. First, a decrease in ESMCSA was associated with prognosis in patients with PPFE. Second, the assessment of skeletal muscle mass in PPFE may reflect a better prognosis than BMI.
It has been suggested that a lower ESMCSA may be associated with the prognosis of PPFE, including secondary PPFE (SPPFE). SPPFE is caused by haematopoietic stem cell transplantation, hypersensitivity pneumonitis, non-tuberculous mycobacterial infection, and chemotherapy [16]. However, it is possible that such comorbidities may simply be comorbid and not affect the patient and that IPPFE is included in the SPPFE. There were no significant differences in the laboratory data, respiratory complications, or survival rates between the idiopathic and secondary PPFE groups [17]. Known prognostic factors for IPPFE include older age, male, lower BMI, elevated KL-6, and lower FVC [4, 18]. This study also found that older age, elevated KL-6 levels, and lower FVC were associated with prognosis; however, no previous reports have shown an association between lower ESMCSA and prognosis. Suzuki et al. also reported an association between PPFE and ESMCSA, but no significant difference was found in prognosis. The reasons for the different results are unclear but could be explained as follows. First, both studies included small numbers of patients and may have observed different phenotypes. Second, approximately half of the patients with PPFE enrolled in this study were underweight, whereas most patients with PPFE reported by Suzuki et al. were underweight, with a BMI of < 18.5 kg/m2. Therefore, it is possible that the patients with PPFE in the report by Suzuki et al. had a longer disease-modifying period than those in this study and already had a more reduced skeletal muscle mass. The ESMCSA in this study was independent of laboratory findings and pulmonary function tests in the multivariate analysis. Therefore, it is important to monitor ESMCSA in patients with PPFE.
In this study, ESMCSA was significantly correlated with age and BMI but not with %FVC or KL-6 values. The correlation of ESMCSA with age and BMI could be related to a decrease in skeletal muscle mass with increasing age or decreasing body weight [19]. However, it is noteworthy that despite a significant difference in survival within 3 years for ESMCSA, there was no significant difference in BMI. This finding may be related to body weight components. Body weight comprises muscle mass, body fat mass, and the amount of inorganic matter in the skeleton. The lack of a significant difference in prognosis with respect to BMI may be because BMI is calculated based on body weight, including body fat and muscle mass. Weight loss can occur for various reasons, including starvation caused by reduced food intake preserving skeletal muscle mass and cachexia resulting in reduced skeletal muscle mass [20].
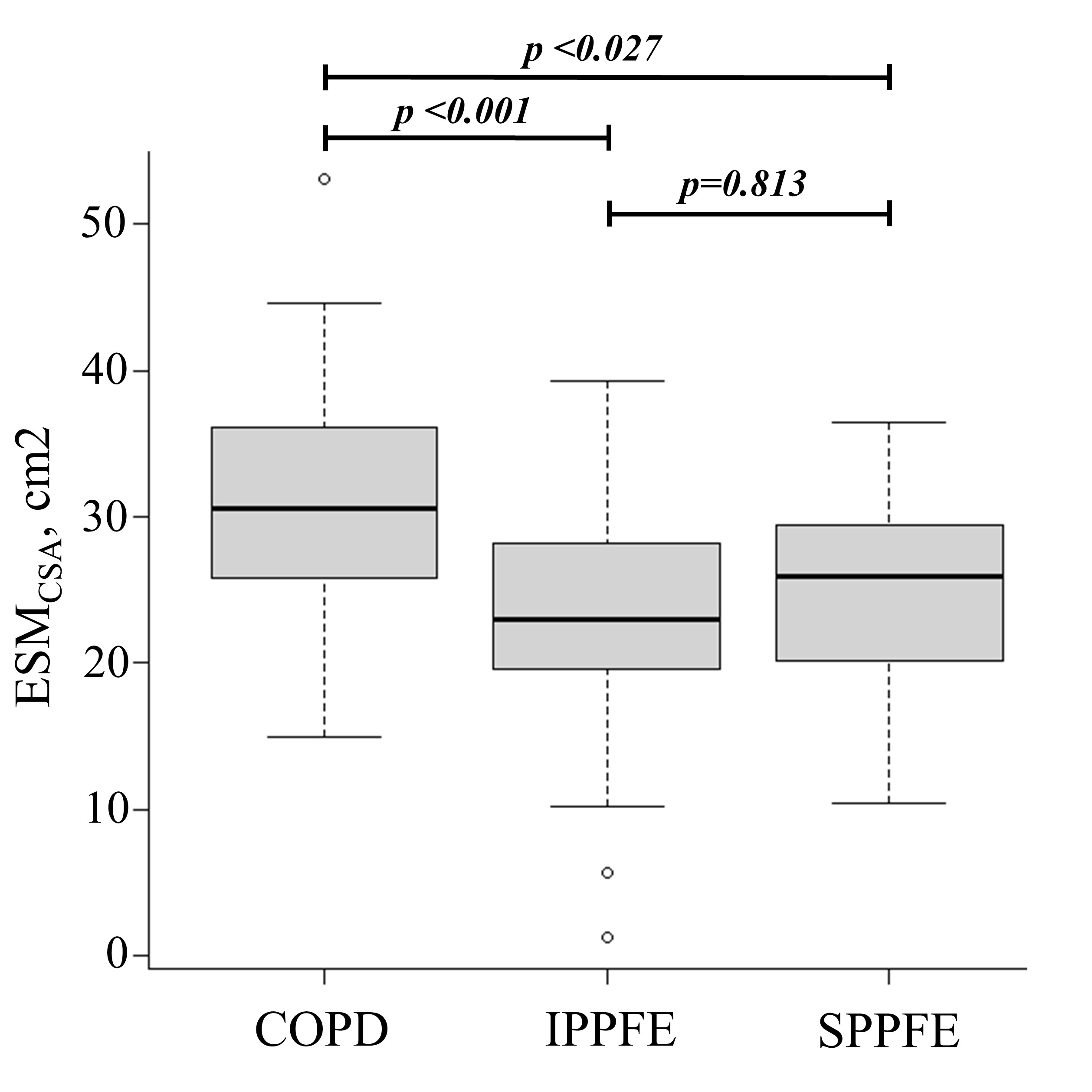
Cachexia is caused by increased energy expenditure due to inflammatory-induced cytokines such as tumour necrosis factor (TNF)-α, interleukin (IL)-1 and IL-6, decreased appetite and increased protein catabolism associated with leptin and ghrelin, and skeletal muscle atrophy due to angiotensin II [21, 22]. Cachexia occurs in cancer patients and is a cause of reduced skeletal muscle mass in COPD patients [9]. Compared to healthy controls, patients with COPD, IPF, and PPFE have lower ESMCSA [12, 14], and those with PPFE have even lower amounts of ESMCSA than those with IPF [14]. In this study, the patients with PPFE had an even lower ESMCSA than those with COPD. This suggests that PPFE may be more strongly affected by cachexia than COPD or IPF. Oral nutritional supplements are often used to treat cachexia, and the ghrelin receptor agonist, anamorelin, has recently proved effective in cancer patients [23, 24]. Ghrelin is an appetite-enhancing peptide secreted from the stomach, which binds to the growth hormone secretagogue receptor-1a (GHSR-1a) and regulates appetite and energy metabolism [25, 26]. Ghrelin and its analogues exhibit appetite-stimulating effects by promoting the expression of agouti-related neuropeptides and neuropeptide Y [27–29] and preventing weight loss [30]. In addition to its appetite-enhancing effects, ghrelin also suppresses energy expenditure by suppressing leptin-induced inflammatory cytokines such as IL-1β, IL-6, and TNF-α, which are central to the pathogenesis of cachexia [31], and reduces skeletal muscle catabolism induced by angiotensin II [32]. Ghrelin may also be effective for PPFE patients with possible skeletal muscle loss due to cachexia. However, non-cancer cachexia is still difficult to study compared to major diseases because of issues such as research funding and lack of public awareness. Therefore, the relationship between PPFE and cachexia, including inflammatory cytokines, remains uncertain and there are few reports on nutritional therapy and anamorelin in interstitial pneumonia, including PPFE. The symptoms of cachexia, such as severe weight loss, anorexia, early satiety, and oedema, are not clear in the early stages of the disease, and the time required for symptom onset greatly depends on the rate of progression of the underlying disease and host responses, such as activation of the systemic inflammatory response and metabolic, immune, and neuroendocrine changes [33]. It is difficult to correct undernutrition in advanced cachexia, and prevention at an early stage is considered important [34]. Although body weight and BMI are often used to assess cachexia [35, 36], the quantitative analysis of body composition using ESMCSA is a better prognostic parameter than body weight or BMI [12]. The results of this study suggest that in PPFE, as in COPD, ESMCSA may be a stronger prognostic factor than BMI.
This study has several limitations. First, it was a retrospective study; thus, it was impossible to assess patients' clinical symptoms, such as dyspnoea, or ADLs at the time of diagnosis of PPFE. Second, although this was not a single-centre study, the number of patients included was relatively small. Third, the study included patients with PPFE who were not pathologically diagnosed. Although pathological evaluation is necessary for a definitive diagnosis of IPPFE, surgical lung biopsy is often not performed due to the risk of postoperative lung leaks, pneumothorax, and acute exacerbation [37, 38]. Therefore, Watanabe et al. [15] proposed a method for diagnosis without surgical biopsy. Finally, the cross-sectional area of the erector spinae muscle was measured as an antigravity muscle that may influence ADL; however, other antigravity muscles, such as the iliopsoas and quadriceps muscles [39], were not assessed. Future prospective studies are required to evaluate various skeletal muscles to overcome these limitations.
In conclusion, we investigated the relationship between the quantification of skeletal muscles using CT and PPFE. This study highlights the importance of monitoring ESMCSA in predicting the prognosis of patients with PPFE. This suggests that ESMCSA may be a better prognostic factor for PPFE than BMI and may be more influenced by cachexia than by COPD.
{kind=link}