A total of 28 studies were included in the analysis. Of these studies, only one did not report the number of patients. Among the remaining 27 studies, there were a total of 2 543 483 patients. Specifically, 900 994 patients had prostate cancer and received ADT, 1 262 905 patients had prostate cancer but did not receive ADT, and 334 682 patients did not have prostate cancer and did not receive ADT. Table 1 provides a summary of the variables analyzed and the quality assessment.
ADT and Dementia
The included studies analyzed the risk of various forms of cognitive decline associated with ADT, including dementia, Alzheimer's, and vascular dementia.
Dementia
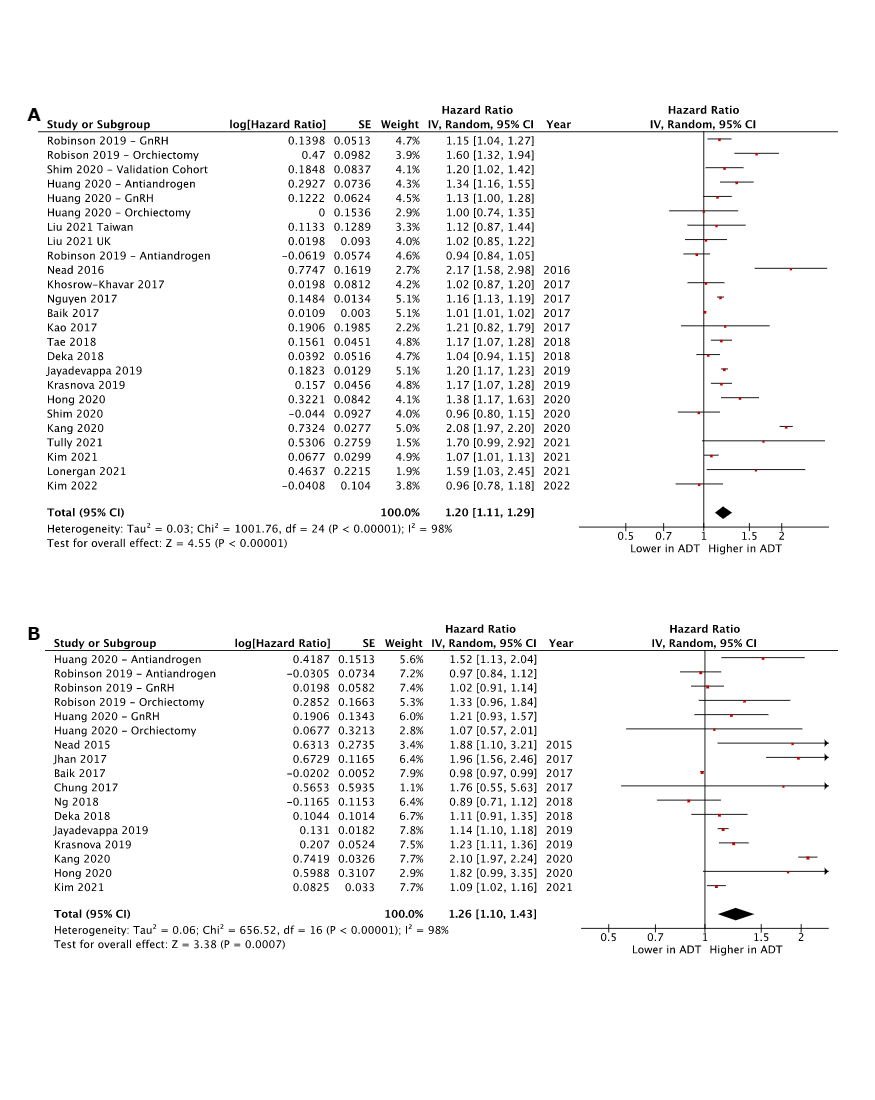
The risk of dementia was analyzed in a total of 20 studies. The analysis revealed a statistically significant HR of 1.20 [1.11, 1.29], p < 0.00001, indicating an increased risk of dementia associated with ADT. Figure 1 displays these findings, and a comprehensive breakdown of the included studies can be found in eFigure 2.A.
Alzheimer’s Disease
Thirteen studies were included in the analysis of the risk of developing AD. The analysis of these studies concluded a statistically significant risk with a HR of 1.26 [1.10, 1.43], p < 0.00001, indicating an increased risk of AD in patients undergoing ADT. These findings are visually displayed in Fig. 1, and a detailed breakdown of the included studies can be found in eFigure 2.B.
Vascular Dementia
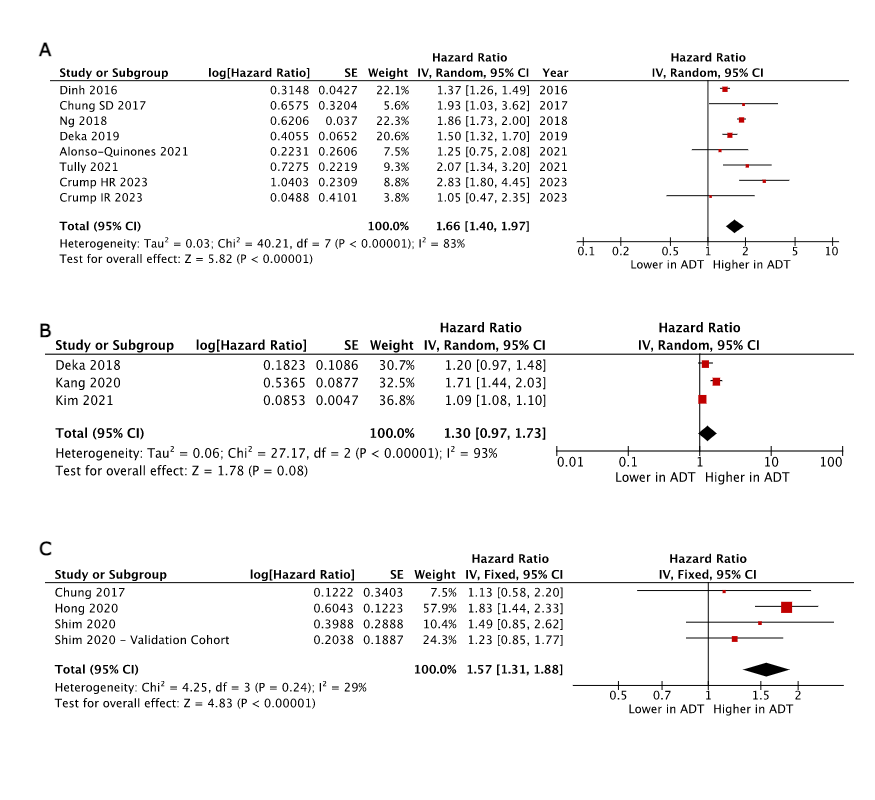
The risk of vascular dementia was assessed in 3 studies. The pooled analysis of these studies indicated a non-significant risk with a HR of 1.30 [0.97, 1.73], p < 0.00001. These findings are depicted in Fig. 1, and a comprehensive breakdown of the included studies can be found in eFigure 3.B.
Depression
The development of depression related to ADT was analyzed in a total of 7 studies. The analysis of these studies revealed a significant risk of depression in patients undergoing ADT, with a HR of 1.66 [1.40, 1.97], p < 0.00001. These findings are visually presented in Fig. 1, and a detailed breakdown of the included studies can be found in eFigure 3.A.
Parkinson’s Disease
The association between Parkinson's Disease and ADT was examined in 3 studies, and the pooled analysis demonstrated a significantly increased risk with a HR of 1.57 [1.31, 1.88], p < 0.00001. These findings are presented in Fig. 1, and a comprehensive breakdown of the included studies can be found in eFigure 3.C.
ADT Modality and Dementia
A subgroup analysis was conducted to stratify the risk of dementia or Alzheimer's disease (AD) based on different modalities of ADT, including orchiectomy, GnRH agonists/antagonists, and antiandrogens.
Dementia
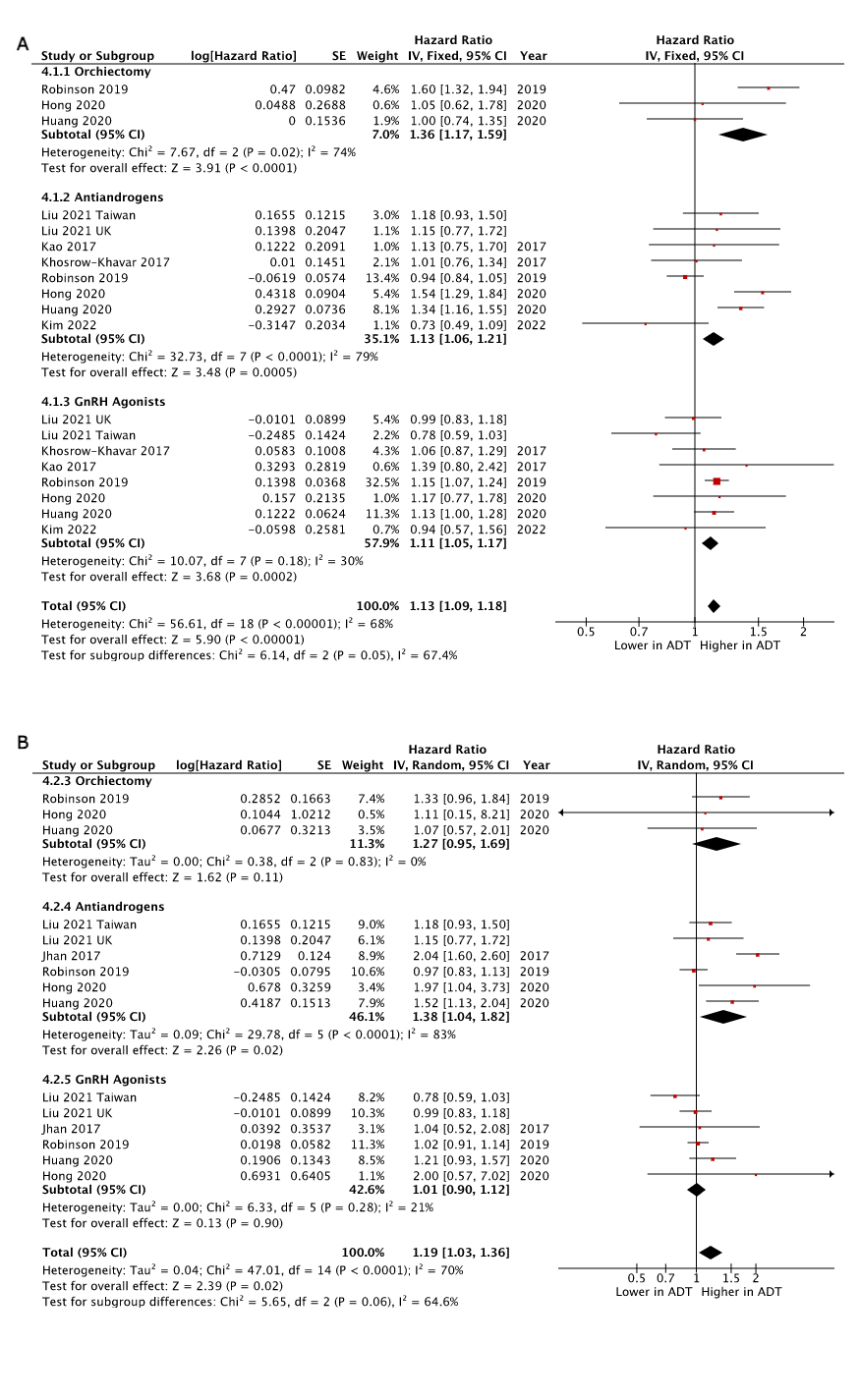
The three therapies above, including bilateral orchiectomy, GnRH agonists/antagonists, and antiandrogens, were analyzed, and significant increases in risk were observed for all three forms of therapy. Among them, the highest risk was associated with bilateral orchiectomy, with a HR of 1.36 [1.17, 1.59], p < 0.0001. It is important to note that this subgroup had the lowest number of included studies (three). These findings are presented in Fig. 2, and a detailed breakdown of the included studies can be found in eFigure 4.A.
Alzheimer’s Disease
The analysis of various individual ADT modalities and the risk of AD indicates that orchiectomy and antiandrogens are associated with a significantly increased risk. These findings are depicted in Fig. 3, and a comprehensive breakdown of the included studies can be found in eFigure 4.B.
Treatment Duration
Studies that provided risk stratification based on treatment duration were included to analyze the impact of duration on the risk of ADT.
Dementia
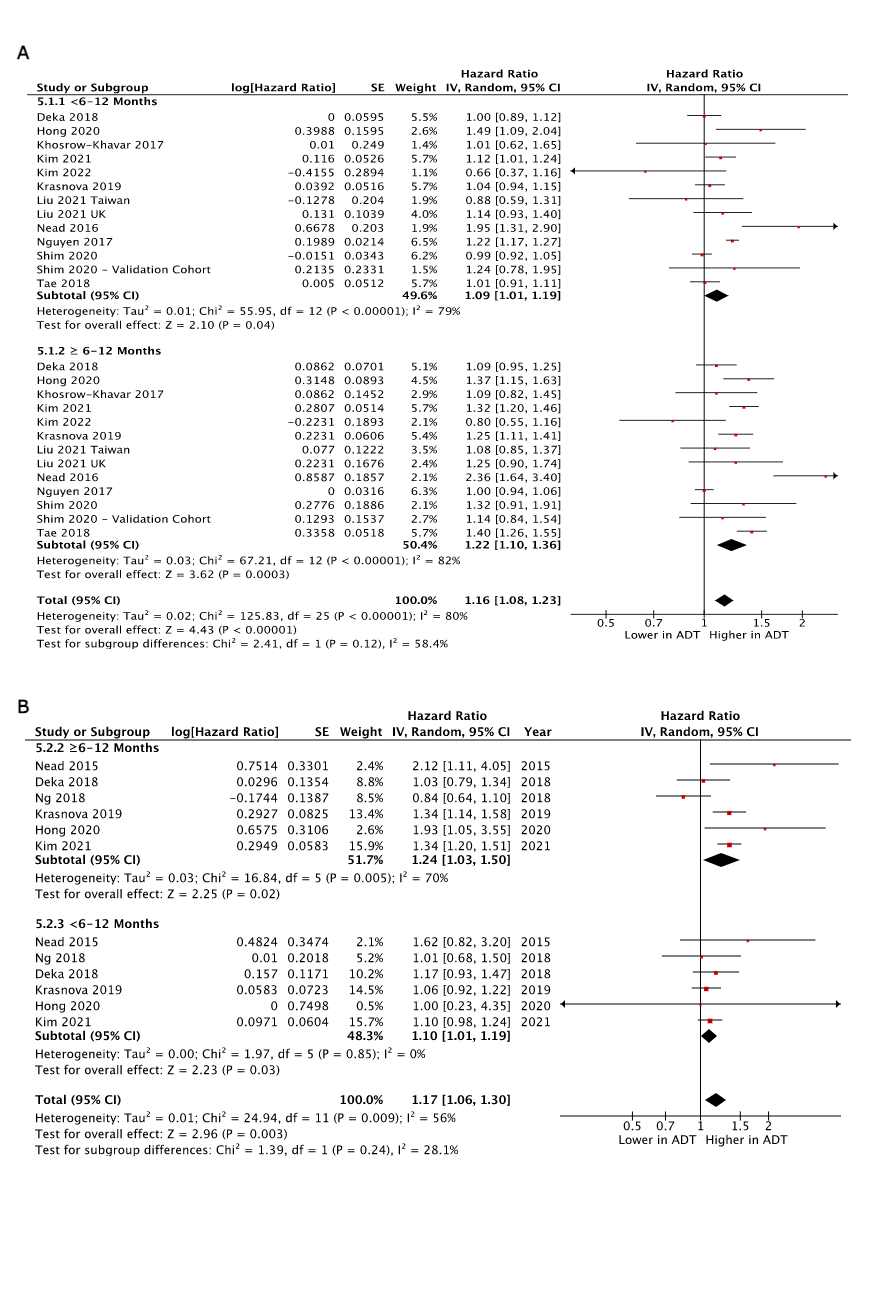
Both therapies lasting less than 6–12 months and those lasting more than 6–12 months were associated with a significantly increased risk of dementia. However, the risk was higher in longer duration therapy, with a HR of 1.22 [1.10, 1.36], p < 0.0001. These findings are visually presented in Fig. 2, and a comprehensive breakdown of the included studies can be found in eFigure 5.A.
Alzheimer’s Disease
The analysis of treatment duration and the risk of developing Alzheimer's disease (AD) indicated an increased risk regardless of the duration of treatment. These findings are presented in Fig. 3, and a detailed breakdown of the included studies can be found in eFigure 5.B.
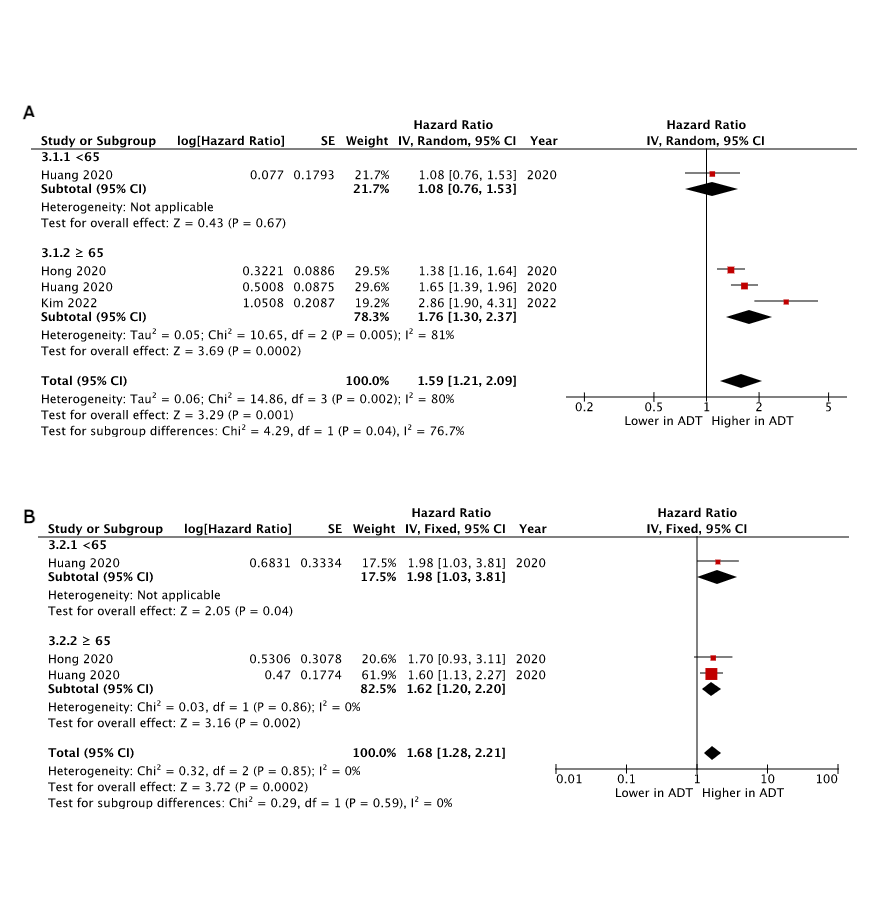
Age, ADT, and Dementia
Among the analyzed studies, only three examined subsets of patients based on age at initiation of ADT. In patients younger than 65, no significant risks were found. However, a significant risk was observed in patients aged 65 and older with a HR of 1.76 [1.30, 2.37], p = 0.0002. These findings are depicted in Fig. 2, and a comprehensive breakdown of the included studies can be found in eFigure 6.A.
The same two studies analyzed age subgroups and AD; however, in this case, the pooled analysis suggested an increased risk for AD regardless of age. These findings are displayed in Fig. 3 with a full breakdown of included studies in eFigure 6.B.
Regional Analysis
A subgroup analysis was conducted based on the continental geographic regions of the included cohorts.
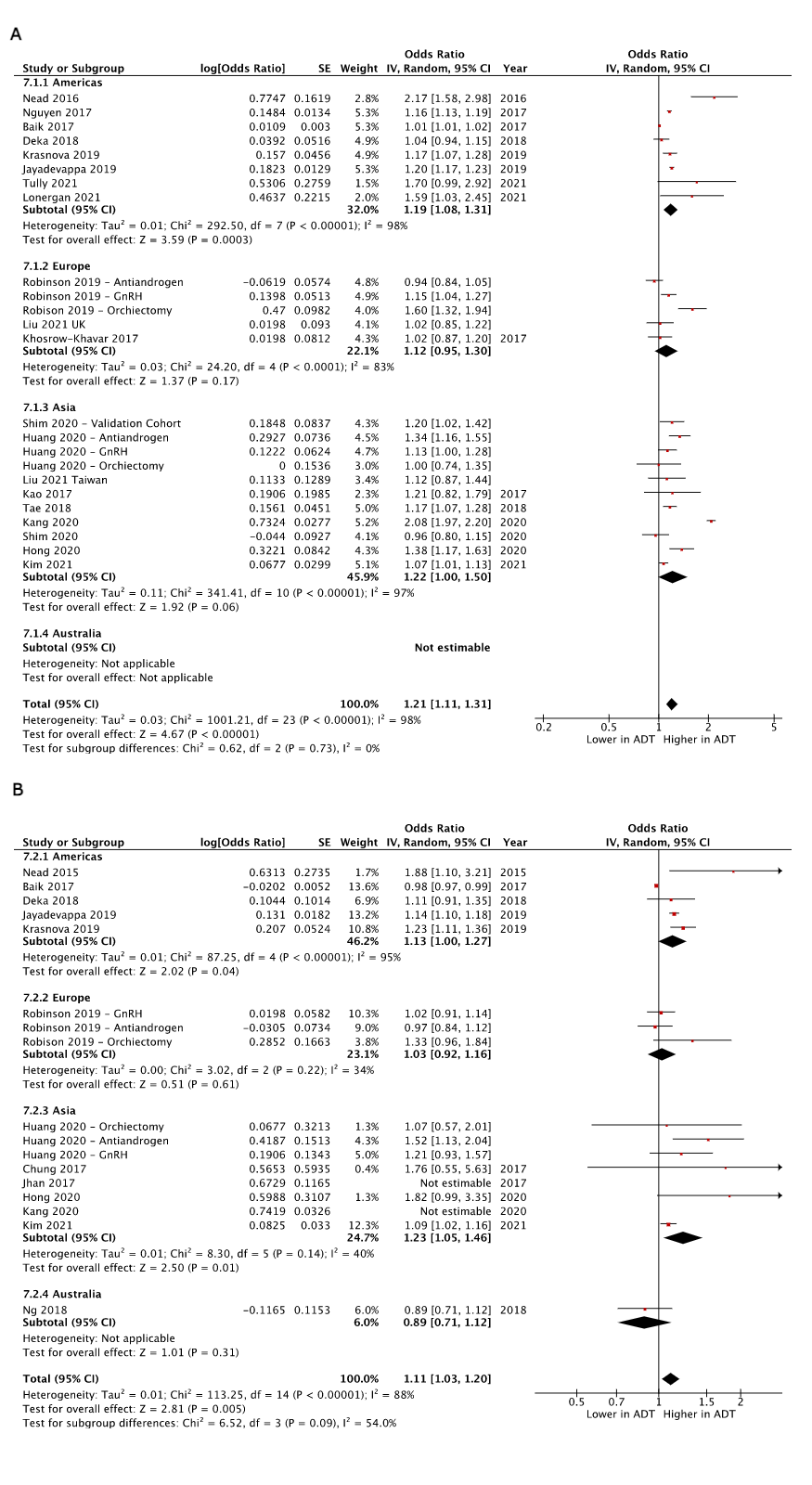
Dementia
The geographical subgroup analysis revealed that only cohorts from America showed an increased risk of dementia with ADT, with a HR of 1.19 [1.08, 1.31], p < 0.0001. These findings are visually presented in Fig. 4, and a comprehensive breakdown of the included studies can be found in eFigure 7.A.
Alzheimer’s Disease
Geographical subgroup analysis revealed that American and Asian cohorts had an increased risk of dementia with ADT, with HR of 1.13 [1.00, 1.27], p < 0.00001) and 1.23 [1.05, 1.46], p = 0.01, respectively. These findings are displayed in Fig. 5, and a comprehensive breakdown of the included studies can be found in eFigure 7.B.
Sensitivity analysis suggests that, for the American subgroup, the main drivers of heterogeneity were Nead et al., Baik et al., and Deka et al. However, these studies did not significantly alter the results and exhibited high interstudy heterogeneity. Robinson et al. were the main drivers of heterogeneity in the European cohort. Partial exclusion of the antiandrogen and orchiectomy subgroups significantly increased risk, while the full exclusion of Robinson et al.'s cohort resulted in non-significant differences. In the Asian region, Kang was the main driver of heterogeneity, and its exclusion did not significantly alter the results.
In the geographical analysis of AD, Baik was identified as the main driver of heterogeneity for the American cohorts. However, excluding Baik did not significantly alter the results. In the Asian cohorts, Jhan and Kang et al. were identified as the main drivers of heterogeneity, but excluding them did not affect the results.
Localized and Adjusted Disease
Ten studies were included for analysis, which consisted of populations featuring only patients with localized prostate cancer or whose propensity scoring successfully adjusted for disease stage. The overall Hazard Ratio (HR) for dementia was 1.23 [1.03–1.38], with a p = 0.0009.
Overlapping Databases
The included studies examined large institutions such as Surveillance Epidemiology and End Results (SEER) and the Korean Health Insurance Information Service (KHIS). Therefore, there may be overlap in the analyzed populations across these studies. Upon excluding the overlapping studies, the HR was determined to be 1.15 [1.07, 1.24], p = 0.0002.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}