Programmed cell death is crucial for the normal growth and development of an organism [30]. As a special kind of cell, cancer cell, is also controlled by programmed cell death via its specific patterns. Additionally, the imbalance of programmed cell death in a cell may be also cancerogenic [30]. Among them, apoptosis, ferroptosis and autophagy have been the most extensively studied. Further, programmed cell death is relational to the cancer metastasis as well as prognosis [31–33].
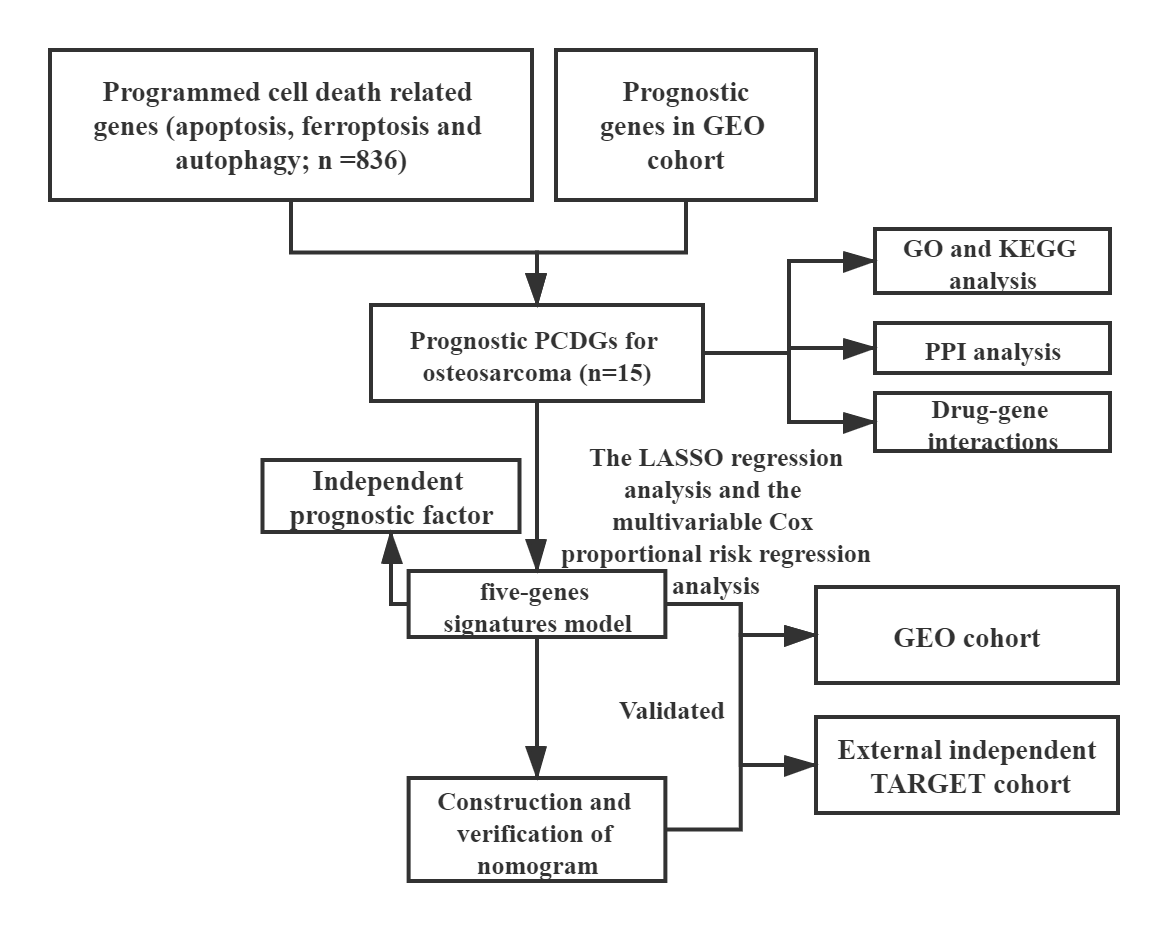
In the previous studies, there are several gene expression-based signatures for the prognosis of osteosarcoma [34–40]. Moreover, gene signatures based on cell death have been reported in diverse cancers, such as lung cancer, hepatocellular carcinoma and gastric cancer[32, 33, 41]. Although an earlier study indicated the importance of apoptosis, little attention was paid to PCDGs in prognosis prediction of osteosarcoma [36]. In this study, we explored and analyzed the prognostic PCDGs in GEO merged osteosarcoma dataset. Via drug-gene interactions, relational available drugs were excavated. LASSO regression as well as multivariate Cox regression with stepwise method analyses were exerted to develop five prognostic markers for GEO merged cohort. In the GEO merged cohort, risk scores significantly stratified patient outcomes. Further, both univariate and multivariate analysis showed that the risk score an independent prognostic indicator. Subsequently, the nomogram consisting of significant risk factors was established. More importantly, in the external independent TARGET cohort, the prognostic efficacy of the five-gene signature as well as the nomogram were verified.
In previous researches, it has been shown that the five genes contained in the signature are all related to cancer. MUC1, a membrane tethered mucin glycoprotein, as a high-risk related gene in our study, was proved a kind of oncogene by most human carcinomas [42, 43]. In the facet of apoptosis, MUC1 often acted as an inhibitory of apoptosis in cancer cells while inducing apoptosis of activated human T cells in the study by Gimmi et al. [44–47]. As an inhibitor of apoptosis, MUC1 conferred the resistance of a variety of drugs as well as radiation treatment on cancer cells [48–51]. Further, many studies indicated the relationship between the high expression of MUC1 and poor prognosis with enhanced metastasis [52, 53]. A possible underlying mechanism by Zhao and his colleagues is that, MUC1 could prolong the survival of circulating tumor cells [54]. TCF7L2, transcription factor 7-like 2, is a critical member of the Wnt/beta-catenin canonical signaling pathway and a moderator of apoptosis [55, 56]. In a variety of tumors, such as colorectal cancer, acute myeloid leukemia and clear cell renal cell carcinoma, this factor was proved related to the metastasis and poor prognosis [57–60]. Further, in beta-estradiol treatment process of osteosarcoma, TCF7L2 was observed reduce the expression with other members involved in Wnt/beta-catenin canonical signaling pathway [61]. TRIAP1 (TP53 regulated inhibitor of apoptosis 1) is a notable inhibitor of apoptosis controlled by TP53 and an available target by epirubicin in osteosarcoma [62]. CBS, cystathionine β-synthase, was associated with homocysteine metabolism, remethylation metabolism, the generation of H2S, drug resistance, oxidative stress and ferroptosis [63–65]. In many neoplasms, CBS was proven differentially expressed to normal tissue and harmful to prognosis. As for osteosarcoma, HU Yang and his group revealed the difference of gene expression of CBS between tumor and normal samples, but did not explore the impact of CBS and its mechanism [66]. TGFB2 encodes a secreted ligand of the transforming growth factor-beta (TGF-β2) superfamily of proteins. TGF-β2 is capable of suppressing interleukin-2-dependent growth of T lymphocytes, and TGF-β2 can be either a proto-oncogene or a tumor suppressor [67]. According to early studies, the function of TGF-β2 was controversial and heterogeneous. On the one hand, TGF-β2 promoted the progress of malignant tumors, such as glioblastoma and breast cancer [68, 69]. On the other hand, TGF-β2 may play a tumor inhibition in pancreatic ductal adenocarcinoma as well as squamous cell carcinomas [70, 71]. Further, TGF-β2 introduced the dormancy of malignant disseminated tumor cells in the bone marrow and TGF-β2 introduced the restriction of metastasis in lungs [72–74].
For osteosarcoma population, our 5-gene risk score model based on PCDGs was shown to be a reliable predictor of prognosis. However, the present study still has some limitations. Firstly, the race and district of patient were heterogeneous because of the retrospective multiple-platform study. Secondly, integrated and uniform clinical characteristic was incomplete for osteosarcoma cohort, needing preferable clinical follow-up and data collection.

{kind=link}