A 51-year-old man with gradual worsening of painless jaundice for >1 month was admitted on January 17, 2020 to the Department of Gastroenterology and Hepatology at the First Medical Center of PLA General Hospital in Beijing, China. Past medical history included vascular replacement (2009) and endovascular repair (2014) of a thoracoabdominal aortic aneurysm. A daily regimen of oral steroid (prednisolone acetate, 10 mg) and immunosuppressant (azathioprine, 100 mg) had also been followed for 10 years as treatment of Behcet’s disease. At the onset of jaundice, which he alone ascribed to primary biliary cirrhosis, the patient arbitrarily boosted his oral steroid dosage to 60 mg/day.
Upon admission, tapering the high-dose steroid was refused. Serum concentrations of total bilirubin (TBIL, 386.8 µmol/L [peak]), direct bilirubin (DBIL, 344.7 µmol/L [peak]), and CA199 (>20000 µ/ml [peak]) were substantially elevated and showed an upward trend. Meanwhile, outcomes of several imaging studies (enhanced abdominal CT, magnetic resonance imaging [MRI], and magnetic resonance cholangiopancreatography [MRCP]) were jointly suggestive of hepatic portal cholangiocarcinoma. On February 7, 2020, the patient underwent percutaneous transhepatic cholangiodrainage, lowering the postprocedural TBIL level to ~100 µmol/L. Surgical intervention was anticipated as liver function further improved.
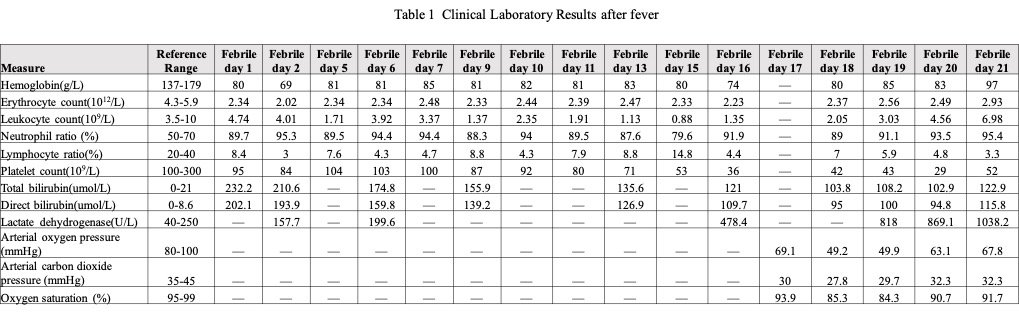
On February 14, 2020, however, a high fever (39.9º C) developed (Figure 1), without cough, sputum, dyspnea, or other respiratory symptoms. Chest CT performed February 15, 2020 (febrile Day 2) showed inflammation in middle and lower lobes of right lung, with bilateral pleural effusions (Figure 2-A). Leukocyte counts had gradually dwindled, falling below normal values, with similar declines in hemoglobin and platelets (Table 1). The patient denied travel to Wuhan or known contact with confirmed or likely sufferers of COVID–19. In consultation with Respiratory Medicine and the Fever Clinic, COVID–19 was not the primary consideration. A consultant from the Hematology Department raised the possibility of hemophagocytic syndrome due to severe systemic inflammation, but subsequent blood transfusion (February 17, 2 units of suspended erythrocytes) and use of granulocyte stimulating factor were not helpful.
After a 12-day experimental antimicrobial treatment (cefoperazone/sulbactam plus levofloxacin), repeat CT imaging of the chest on February 20 (febrile Day 7, Figure 2-B) and on February 24 (febrile Day 11, Figure 2-C) indicated some resolution of pneumonia and effusions, in support of bacterial infection. Still, high fever persisted almost daily (Figure 1). All cultures (blood x 4, sputum, and bile) and oropharyngeal swabs (influenza A and B) obtained during this period were negative.
Meanwhile, in chest CT of February 24, slight newly emergent ground-glass opacities (GGOs) were visible in subpleural peripheral distribution (Figure 2-D), and the patient complained of increasing fatigue (Figure 1). An oropharyngeal swab tested for SARS-CoV–2 by real-time RT-PCR proved negative (February 25). Although fungal β-d-glucan was quite high (134.9 pg/ml), Aspergillus galactomannan antigen and T-cell spot test for tuberculosis (T-spot. TB; Oxford Immunotec, Abingdon, UK) were negative, as were screenings for human immunodeficiency virus (HIV), Epstein-Barr virus, and cytomegalovirus. Meropenem and voriconazole, given in combination for potential fungal infection, failed to lower the body temperature, which exceeded 39º C; and the leukocyte count continued to drop, falling to 0.88×109/L on February 28 (Table 1).
A chest CT on February 28 (febrile Day 15) showed progression to diffuse GGOs in both lungs (Figure 2-E/F), as in patients with severe confirmed COVID–19, and the patient grew increasingly dyspneic (Figure 1). A second oropharyngeal swab for SARS-CoV–2 testing was again negative. Through multidisciplinary consultation with the Fever Clinic and other divisions (Departments of Respiratory Medicine, Medical Imaging, Rheumatology, Cardiovascular Medicine, and Gastroenterology), a consensus diagnosis of PJP (rather than COVID–19) was reached. Voriconazole was then replaced by caspofungin and trimethoprim-sulfamethoxazole (TMP/SMX), administered in conjunction with intravenous prednisolone acetate (80 mg/day). Normal body temperature was restored the evening of February 28, and the leukocyte count began to normalize. Above therapeutic responses seemed to validate the diagnosis of PJP.
Unfortunately, an exacerbation of dyspnea occurred the night of March 1, 2020, diminishing oxygen saturation. Noninvasive ventilation (NIV) sufficed initially, but fever resumed on March 2, 2020, at which time a third oropharyngeal swab for SARS-CoV–2 tested negative. To address possible co-infections, teicoplanin and ganciclovir were started and soon lowered his body temperature to normal. Cough developed March 4, 2020 (febrile Day 20, Figure 1), and dyspnea was aggravated by a spontaneous pneumothorax. Chest radiographs taken separately on March 4 and March 5, 2020 continued to show diffuse interstitial opacities and consolidation. Non-invasive ventilation was no longer tenable, but the patient himself (with support of his family) declined mechanical ventilatory assistance, succumbing to pneumonia and respiratory failure on March 7, 2020.
{kind=link}